Featured Case
-
Abstract
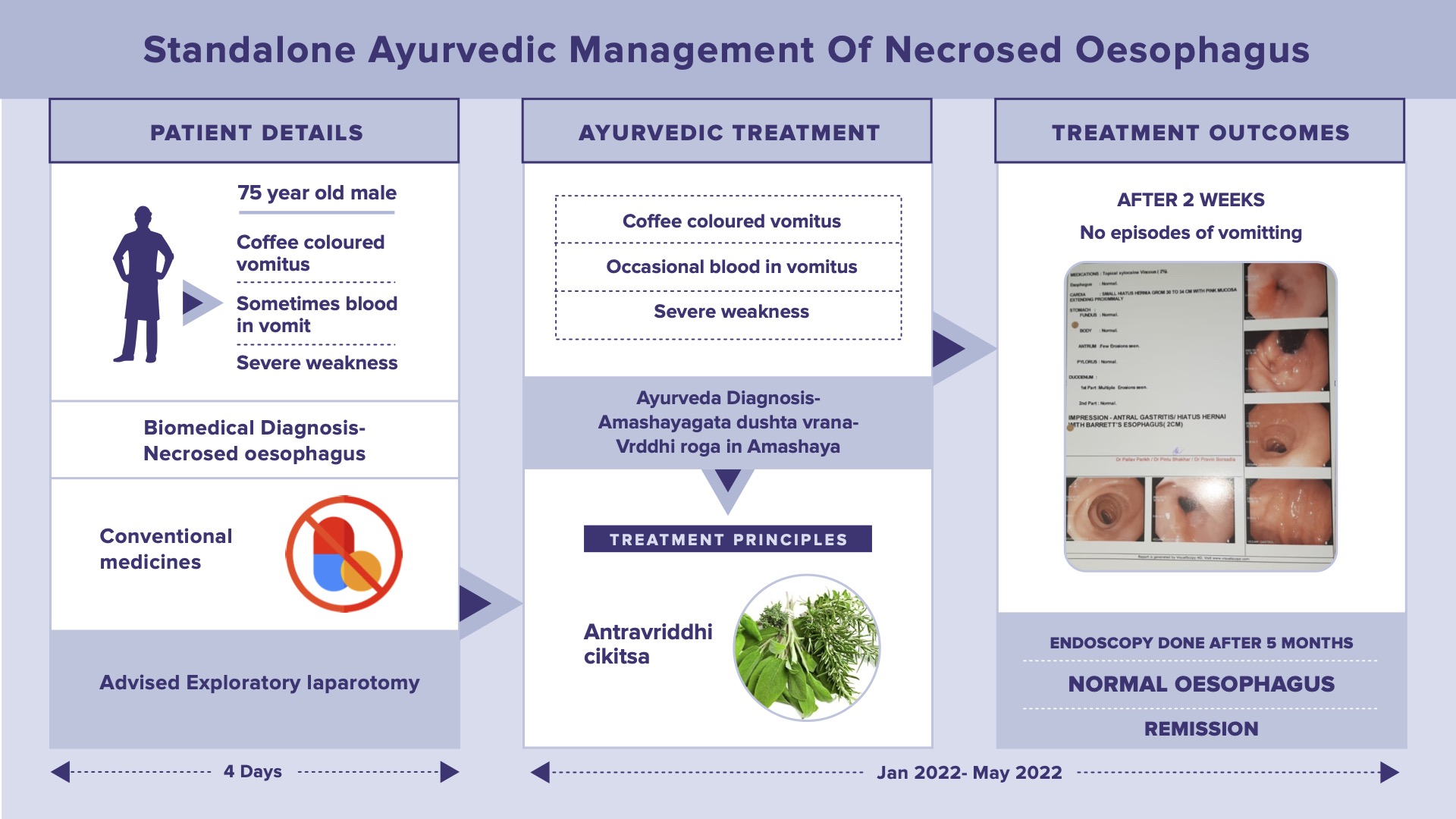
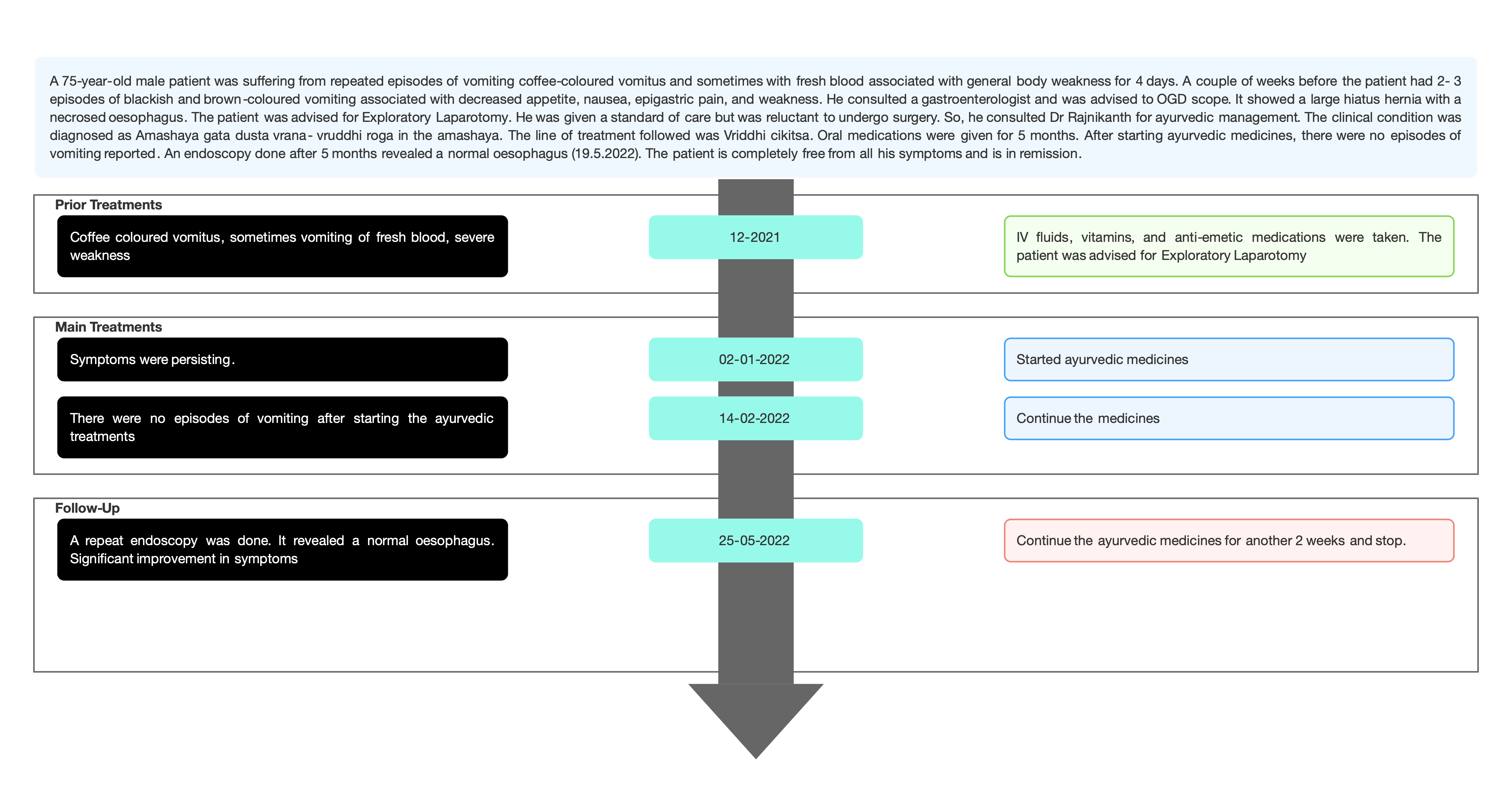
A 75-year-old male patient presented with repeated episodes of vomiting coffee-coloured vomitus and sometimes with fresh blood associated with general body weakness for 4 days. A couple of weeks before the patient had 2- 3 episodes of blackish and brown-coloured vomiting associated with decreased appetite, nausea, epigastric pain, and weakness. He consulted a gastroenterologist and was advised to undergo OGD scope. It showed a large hiatus hernia with a necrosed oesophagus. The patient was advised for Exploratory Laparotomy. He was given standard of care but was reluctant to undergo surgery. So, he consulted Dr Rajnikanth for ayurvedic management. The clinical condition was diagnosed as Amashaya gata dusta vrana- vriddhi roga in the amashaya. The line of treatment followed was Vriddhi cikitsa sutra. Oral medications were given for 5 months. After starting ayurvedic medicines, there were no episodes of vomiting reported. An endoscopy done after 5 months revealed a normal oesophagus (19.5.2022). The patient is completely free from all his symptoms and is in remission.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 75-year-old male patient presented with repeated episodes of vomiting coffee-coloured vomitus and sometimes with fresh blood associated with general body weakness for 4 days. A couple of weeks before the patient had 2- 3 episodes of blackish and brown-coloured vomiting associated with decreased appetite, nausea, epigastric pain, and weakness. He consulted a gastroenterologist and was advised to undergo OGD scope. It showed a large hiatus hernia with a necrosed oesophagus. The patient was advised for Exploratory Laparotomy. He was given standard of care but was reluctant to undergo surgery. So, he consulted Dr Rajnikanth for ayurvedic management. The clinical condition was diagnosed as Amashaya gata dusta vrana- vriddhi roga in the amashaya. The line of treatment followed was Vriddhi cikitsa sutra. Oral medications were given for 5 months. After starting ayurvedic medicines, there were no episodes of vomiting reported. An endoscopy done after 5 months revealed a normal oesophagus (19.5.2022). The patient is completely free from all his symptoms and is in remission.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Standalone ayurvedic management of Necrosed Oesophagus - A case report
Dr Rajnikanth Patel
ABSTRACT
A 75-year-old male patient presented with episodes of vomiting coffee-coloured vomitus and sometimes with fresh blood associated with general body weakness for 4 days. A couple of weeks before the patient had 2- 3 episodes of blackish and brown-coloured vomiting associated with decreased appetite, nausea, epigastric pain, and weakness. He consulted a gastroenterologist and was advised to undergo an OGD scope. It showed a large hiatus hernia with a necrosed oesophagus. The patient was advised for Exploratory Laparotomy. He was given standard of care but was reluctant to undergo surgery. So, he consulted Dr Rajnikanth for ayurvedic management. This was diagnosed as Amashaya gata dusta vrana- vriddhi roga in the amashaya. The line of treatment followed was Vriddhi cikitsa sutra. Oral medications were given for 5 months. After starting ayurvedic medicines, there were no episodes of vomiting reported. An endoscopy done after 5 months revealed a normal oesophagus (19.5.2022). The patient is completely free from all his symptoms and is in remission.
KEYWORDS
Necrosed oesophagus, Amashayagata dusta vrana, Ayurveda, Vriddhi, Case report, Standalone
INTRODUCTION
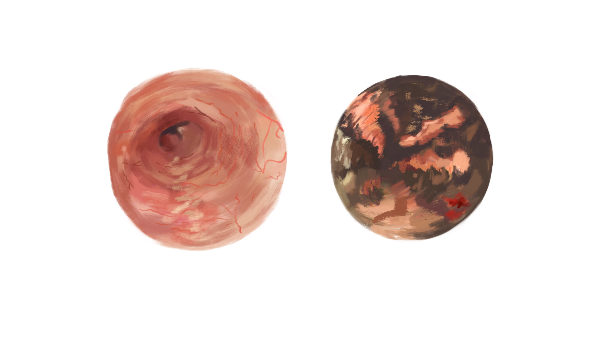
Acute esophageal necrosis is a rare syndrome classically characterized by a striking endoscopic image of diffuse and circumferential black mucosal discolouration of the distal esophagus, with an abrupt transition at the gastroesophageal junction and variable proximal extension. The typical patient is an older male with general debilitation and multiple comorbidities presenting with hematemesis or melena.
The pathophysiology usually involves a combination of oesophagal ischemia, backflow injury from gastric chemical contents and impaired mucosal reparative mechanisms associated with debilitated physical states. It may arise in the setting of hemodynamic compromise, diabetic ketoacidosis, hypothermia, alcoholic intoxication, trauma, inflammatory diseases, esophageal local infection, solid organ transplantation, postoperative status, drugs or acute gastric outlet obstruction, usually in the background of a chronic debilitating process, where the concurrent presence of multiple risk factors, including diabetes mellitus, hypertension, malnutrition, malignancy or alcohol abuse, places a patient at higher risk.
Diagnostic criteria: The characteristic endoscopic appearance establishes the diagnosis. A biopsy is supportive but not required. In this patient, the diagnosis was confirmed with OGD scope/endoscopy.
Management: This is mainly supportive and consists of correcting coexisting conditions, fluid therapy, bowel rest, intravenous proton pump inhibitor therapy and red blood cell transfusion as needed. Although this is a serious life-threatening condition, appropriate treatment may result in a favorable outcome in most patients. [1]
PATIENT INFORMATION
A 75-year-old male patient was suffering from repeated episodes of vomiting coffee-coloured vomitus and sometimes with fresh blood associated with general body weakness for 4 days. He had a similar episode 2 weeks back for which he took treatment and the symptoms subsided.
Medical History: A couple of weeks before (December 2021), the patient had 2- 3 episodes of blackish and brown-coloured vomiting associated with decreased appetite, nausea, epigastric pain and weakness. He consulted a gastroenterologist and was advised to undergo OGD scope (Esophagogastroduodenoscopy) also called endoscopy. It showed a large hiatus hernia with the necrosed oesophagus. The patient was advised for Exploratory Laparotomy. The patient was given standard care, but he was reluctant to undergo surgery and opted for Ayurveda treatment.
CLINICAL FINDINGS/PHYSICAL EXAMINATION
None were done
TIMELINE
Image 1. Timeline of events
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The biomedical diagnosis was done based on the clinical presentation and the endoscopy reports.
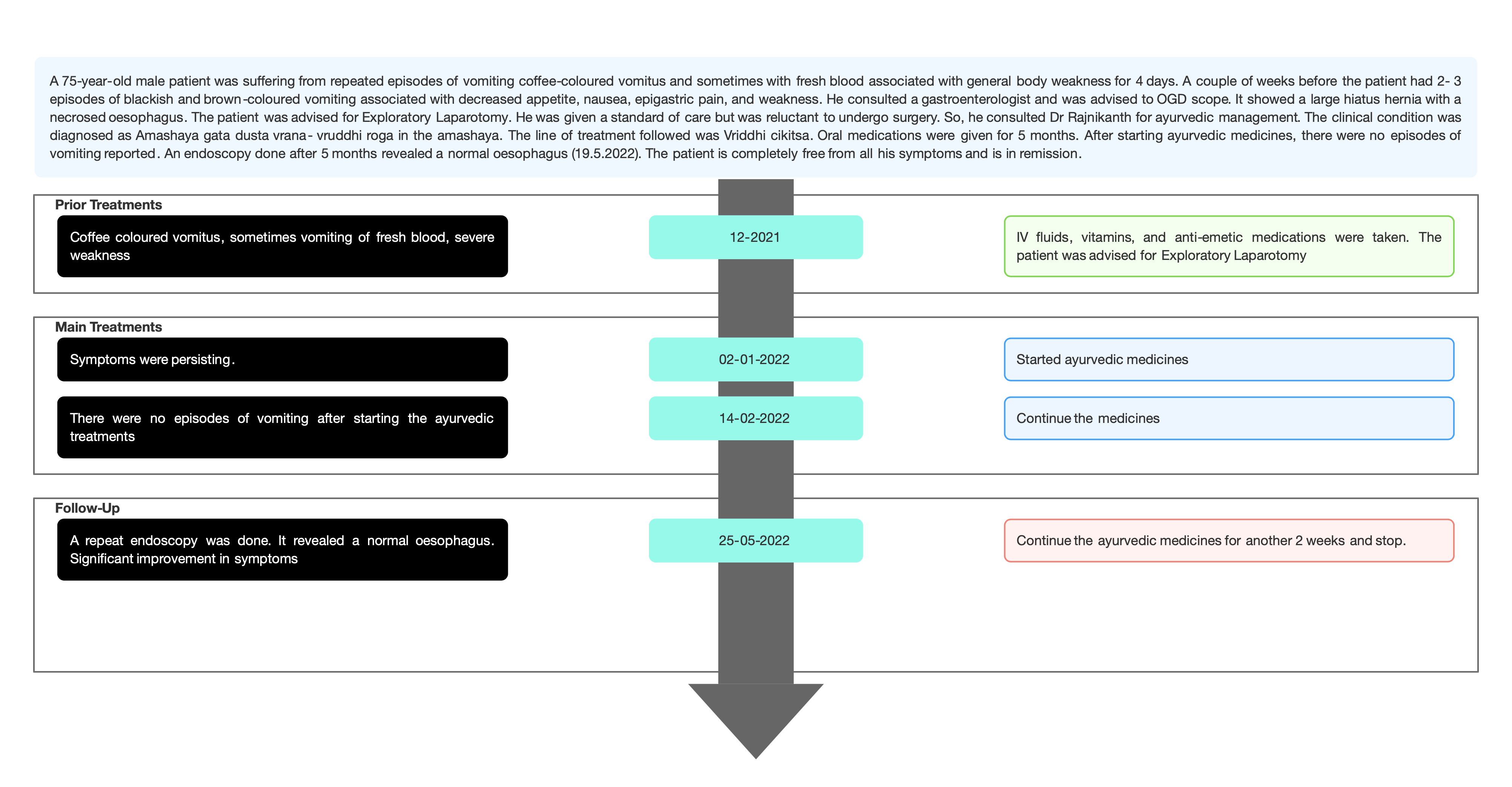
Image 2. Report of OGD scope dated 22.12.2021 added below
Ayurvedic Assessment was done based on the investigation reports and the clinical evaluation by the ayurvedic physician.
Differential Diagnosis- The diagnosis was confirmed with clinical examination and endoscopy.
Prognosis- Overall prognosis is poor with nearly one-third of patients succumbing to the underlying critical illness. The reversible phenomena of the disease and its tendency for spontaneous healing are favourable factors in predicting a complete recovery in otherwise healthy individuals. In this case, the patient had no other co-morbidities and can be considered a favourable factor for complete recovery. The patient was under the standard of care and was suggested for surgical management (In the physician’s words- No supporting documents were available). Oral medications were given for 5 months. In the further follow up the condition improved, and episodes of vomiting were reduced. Endoscopic findings (19/5/2022) revealed a normal oesophagus.
THERAPEUTIC INTERVENTION
See the tab ‘Treatment details’
FOLLOW-UP AND OUTCOMES
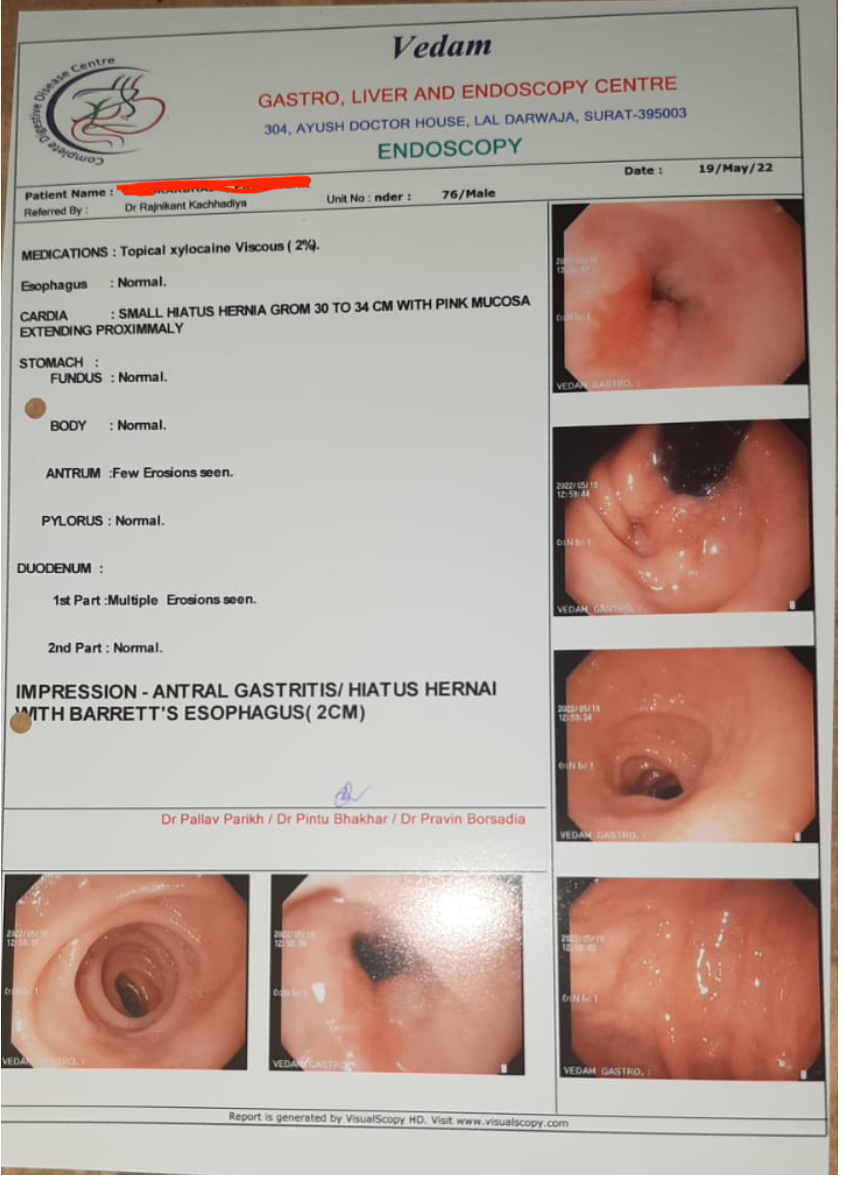
Clinician-based assessment; After starting the Ayurveda treatment, there were no episodes of vomiting reported. The repeat endoscopy done after 5 months of ayurvedic treatment revealed a normal oesophagus. The patient also got complete relief from generalised weakness.
Patient-assessed: Not relevant.
Image 3. Endoscopy dated 19.5.2022 added below
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported.
DISCUSSION
The medicines prescribed were Gandarvahastadi eranda taila - Mentioned in Antravrddhi chikitsa. As the patient had hiatus hernia, this was advised. Nagarjunaabra rasa was prescribed to increase blood circulation. Cardorium plus syrup was prescribed to improve blood circulation. Vriddhibaadika vati is mentioned in Vriddhi cikitsa.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
The 75-year-old male patient tried conventional medicine, for his symptoms of repeated episodes of blackish, brown-coloured vomiting associated with decreased appetite, nausea, epigastric pain and weakness, but did not get relief. When the gastroenterologist suggested exploratory laparotomy, the patient opted for ayurveda. With ayurvedic treatment, he got relief from all his symptoms and there has been no episode of vomiting. A repeat endoscopy revealed a normal oesophagus. With 6 months of ayurvedic treatment, necrosed oesophagus could be successfully reverted. The patient is in remission.
INFORMED CONSENT
Written consent was obtained from the patient to publish the case report.
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
- Dias E, Santos-Antunes J, Macedo G. Diagnosis and management of acute oesophagal necrosis. Ann Gastroenterol. 2019 Nov-Dec;32(6):529-540.
Image 2. Baseline OGD report
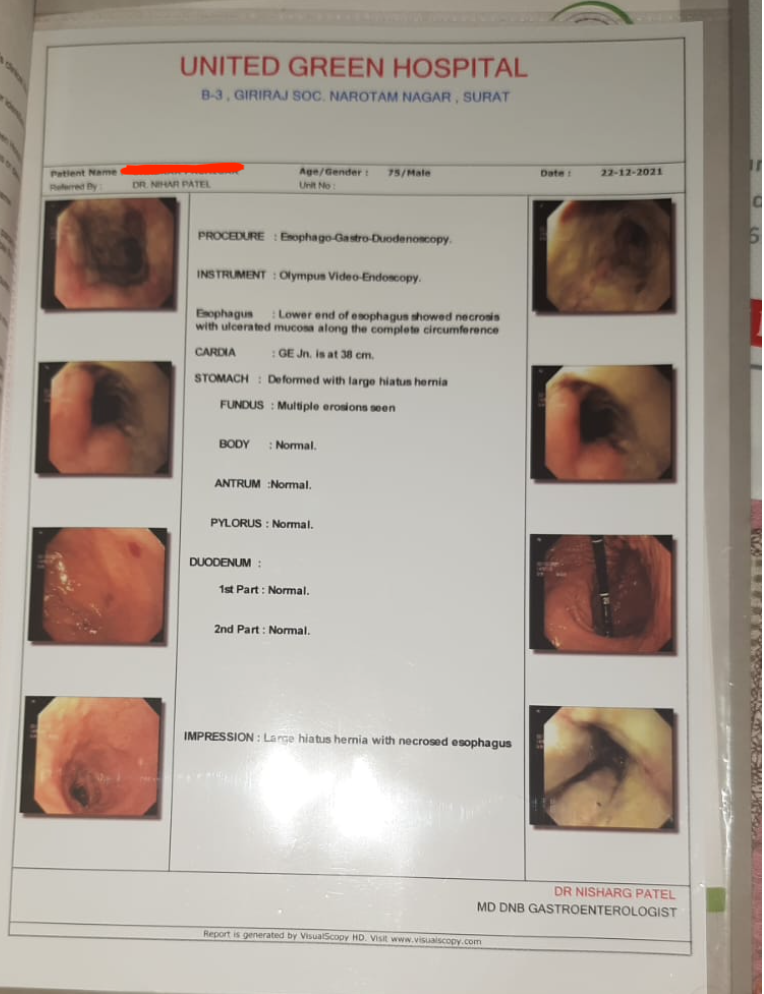
Image 3. Endpoint Scan report
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Necrosed oesophagus
ABOUT THE DISEASE:
Acute oesophagal necrosis is a rare syndrome classically characterized by a striking endoscopic image of diffuse and circumferential black mucosal discolouration of the distal esophagus, with an abrupt transition at the gastroesophageal junction and variable proximal extension. The typical patient is an older male with general debilitation and multiple comorbidities presenting with hematemesis or melena.
The pathophysiology usually involves a combination of oesophagal ischemia, backflow injury from gastric chemical contents and impaired mucosal reparative mechanisms associated with debilitated physical states. It may arise in the setting of hemodynamic compromise, diabetic ketoacidosis, hypothermia, alcoholic intoxication, trauma, inflammatory diseases, esophageal local infection, solid organ transplantation, postoperative status, drugs or acute gastric outlet obstruction, usually in the background of a chronic debilitating process, where the concurrent presence of multiple risk factors, including diabetes mellitus, hypertension, malnutrition, malignancy or alcohol abuse, places a patient at higher risk. In this case report, the 75-year-old male patient was suffering from repeated episodes of vomiting coffee-coloured vomitus and sometimes with fresh blood associated with general body weakness for 4 days. He had a similar episode 2 weeks back for which he took treatment and the symptoms subsided. During this episode, an OGD scope was done and the biomedical diagnosis was confirmed as a large hiatus hernia with a Necrosed oesophagus. He was advised exploratory laparotomy, but the patient was unwilling. So he opted for ayurveda.
Diagnostic criteria: The characteristic endoscopic appearance establishes the diagnosis. A biopsy is supportive but not required. In this patient, the diagnosis was confirmed with OGD scope/endoscopy.
Image 1. OGD scope dated 22.12.2021 added below
Management: This is mainly supportive and consists of correcting coexisting conditions, fluid therapy, bowel rest, intravenous proton pump inhibitor therapy and red blood cell transfusion as needed. Although this is a serious life-threatening condition, appropriate treatment may result in a favourable outcome in most patients. [1]
Reference
- Dias E, Santos-Antunes J, Macedo G. Diagnosis and management of acute oesophagal necrosis. Ann Gastroenterol. 2019 Nov-Dec;32(6):529-540.
Image 1. Baseline OGD report
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Aamashaya gata dusta vrana - Vriddhi roga in amashaya
ABOUT THE DISEASE:
वृणोति यस्मात् रूढे अपि व्रणवत्सु न नश्यति ।
आदेह धार्नात्तस्मात्व्रणैत्युच्च्यते ।As the scar of wound remains even after complete healing and its imprint persists life long, it is called as Vrana. As it causes destruction of the tissue or damage to body part, so it is termed as Vrana.(Sushruta Samhita. Vol 1. Pg 189)
Dushta Vrana lakshana- The vrana is described to be samvruta, kathina, avasanna, with vedana, vivruta, ushna, daha, paka, raga, puyasravya, manojnadarshana, kandu, shopha, pidaka, mrudu, bhairava, putimamsasirasnayu. (Sushruta Samhita. Vol 1. Pg 191) (Ashtanga hridaya 2008. 1066)
In general, dushta vrana is more intense than shuddha vrana. This may require serious medical intervention. In this case report, the physician has diagnosed the condition as Amashaya gata dushta vrana, whose reference cannot be directly obtained from the classical ayurvedic textbooks. The diagnosis is based on the presence of necrosis in the oesophagus.
Treatment: Susruta mentions the Shashtyupakrama for managing the vrana.
General treatments followed in Dusta vrana are:
i) Shamana, Apatarpana, Alepa, Pariseka, Abhyanga, Sweda, Vimlapana, Upanaha, Pacana, Sneha, Vamana, Virecana
2) Chedana, Bhedana, Dharana, Lekhana, Eshana, Aharana, Vyadhana, Visravana, Seevana, Sandhana, Ksharakarma, Agnikarma, Pratisaarana, Lomaapaharana and YantraRopana is a primary target of vrana cikitsa. The treatments chosen should help heal the wound. In the case of dushta vrana, shodhana and ropana may be required. When the vrana becomes free from discharge, smell, burning sensation, itching, and healing, the treatment becomes effective.
The physician has also mentioned Vriddhi in the amashaya as the ayurvedic diagnosis. Vriddhi is normally correlated to hernia, hydrocoele, and scrotal humor. Caraka has included vriddhi in the context of shotha. Susruta has explained 7 types of vriddhi. (SS.Ni.12.3). In this case report, the physician has not exactly mentioned the subtype of vriddhi in the diagnosis, but in the treatment, it is mentioned as Antravriddhi cikitsa.
Prognosis: The vriddhi which is similar to vataja type is asadhya.
In this patient the treatment modality adopted was Antravriddhi cikitsa. The treatments addressed improving and increasing blood circulation.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Gandarvahastadi Eranda Tailam Tailam 2 tsp BD after food with warm water 2022-01-07 - 2022-06-15 AH. Vatavyadhi Cikitsa Nagarjunabhra rasa Tablet 1 BD, after food with warm water 2022-01-07 - 2022-06-15 Ayurveda sara sangraha, Rasayana prakarana Vridhibhadika vati Tablet 3 BD, after food with warm water 2022-01-07 - 2022-06-15 Bhaishajya ratnavali. Arsharoga cikitsa Cardorium plus syrup Syrup 20 ml BD after food 2022-01-07 - 2022-06-15 Patent & proprietary medicine -
Outcome Measures
OUTCOME MEASURES
A 75-year-old male patient was suffering from repeated episodes of vomiting coffee-coloured vomitus and sometimes with fresh blood associated with general body weakness for 4 days. A couple of weeks before the patient had 2- 3 episodes of blackish and brown-coloured vomiting associated with decreased appetite, nausea, epigastric pain, and weakness. He consulted a gastroenterologist and was advised to undergo an OGD scope. It showed a large hiatus hernia with a necrosed oesophagus. The patient was advised for Exploratory Laparotomy. He was given a standard of care but patient was reluctant to undergo surgery. So, he consulted Dr Rajnikanth for ayurvedic management.
The outcomes were measured based on subjective and objective parameters.
Subjective parameters: After starting the Ayurveda treatment, there were no episodes of vomiting reported. There was also a significant improvement in the associated symptom like general body weakness.
Objective parameters: The endoscopy was done after 5 months of ayurvedic treatment and revealed a normal oesophagus.
Image 1. Endoscopy dated 19.5.2022 added below
All the medicines were stopped after 6 months and there was no relapse of symptoms.
Disease-modifying effect: The patient is in remission.
Image 1. Endoscopy report at endpoint
-