Featured Case
-
Abstract
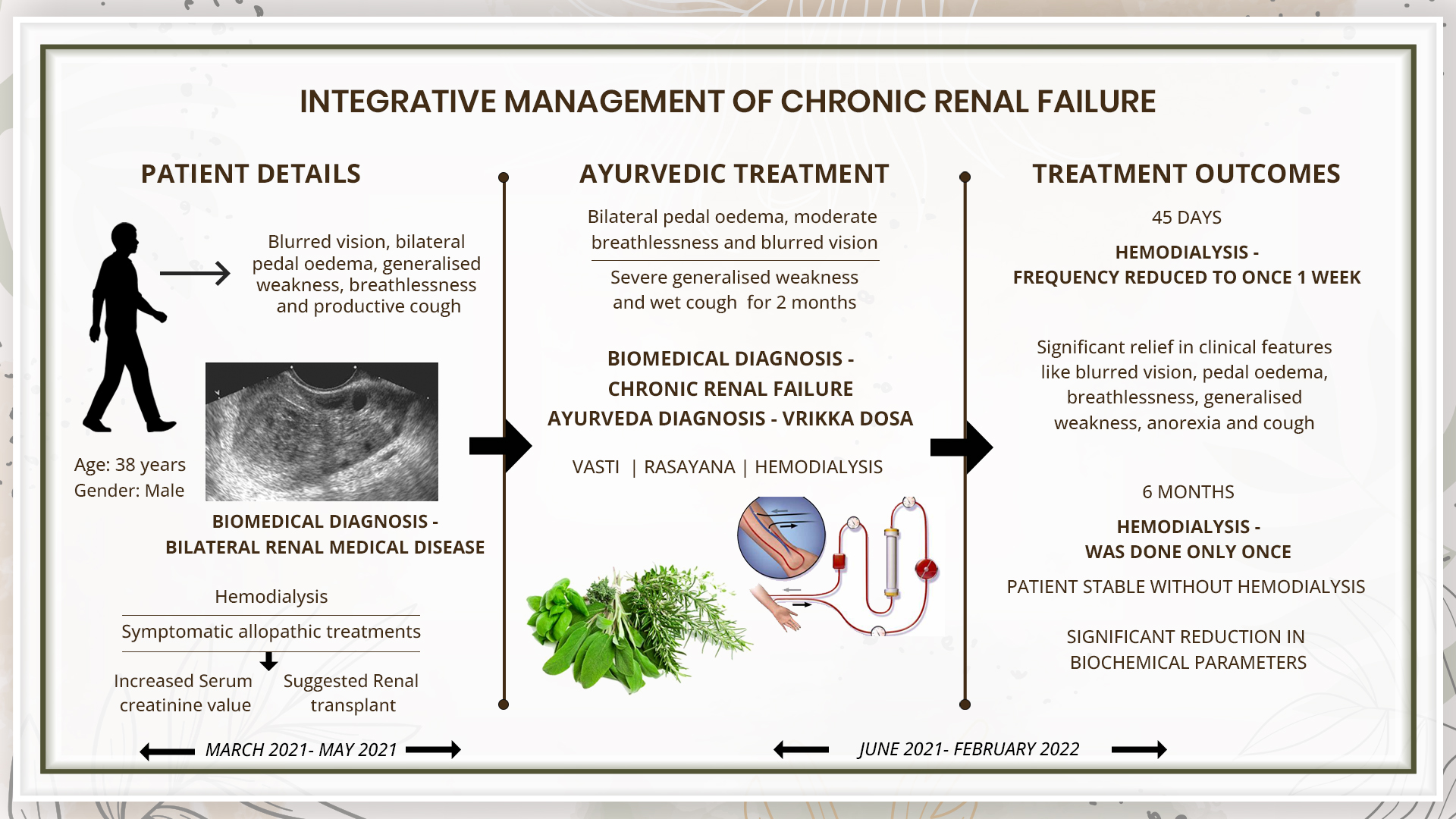
A 38-year-old male patient complained of bilateral pedal oedema, moderate breathlessness, and blurred vision along with severe generalized weakness and wet cough. The Biomedical diagnosis was made based on the USG as bilateral medical-renal disease[1] along with bilateral moderate to gross pleural effusion. His serum creatinine level was recorded as 21.5mg/dl. Patient was then referred to higher centre for haemodialysis by the Nephrologist The patient underwent haemodialysis on daily basis from 26th March 2021 to 1st April 2021 supported with medications for symptomatic management. The schedule of haemodialysis was now changed to thrice a week for one month. Further he was suggested for renal transplant. The patient now consulted Dr Pankaj Chayyani and the Ayurvedic diagnosis made was Vrikka dosa [2]. As the tridosa are involved in the pathogenesis, the treatment was planned to address this along with Rasayana cikitsa, and Vasti karma. Specific allopathic medications were continued during Ayurvedic treatment. Haemodialysis was done when the clinical features of uraemia appeared, or the serum creatinine level increased to 12. With Ayurvedic treatments, haemodialysis could be stopped completely, and serum creatinine was normal and stable. His symptoms of bilateral pedal oedema, breathlessness, blurred vision, generalised weakness, and wet cough were completely relieved.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 38-year-old male patient complained of bilateral pedal oedema, moderate breathlessness, and blurred vision along with severe generalized weakness and wet cough. The Biomedical diagnosis was made based on the USG as bilateral medical-renal disease[1] along with bilateral moderate to gross pleural effusion. His serum creatinine level was recorded as 21.5mg/dl. Patient was then referred to higher centre for haemodialysis by the Nephrologist The patient underwent haemodialysis on daily basis from 26th March 2021 to 1st April 2021 supported with medications for symptomatic management. The schedule of haemodialysis was now changed to thrice a week for one month. Further he was suggested for renal transplant. The patient now consulted Dr Pankaj Chayyani and the Ayurvedic diagnosis made was Vrikka dosa [2]. As the tridosa are involved in the pathogenesis, the treatment was planned to address this along with Rasayana cikitsa, and Vasti karma. Specific allopathic medications were continued during Ayurvedic treatment. Haemodialysis was done when the clinical features of uraemia appeared, or the serum creatinine level increased to 12. With Ayurvedic treatments, haemodialysis could be stopped completely, and serum creatinine was normal and stable. His symptoms of bilateral pedal oedema, breathlessness, blurred vision, generalised weakness, and wet cough were completely relieved.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Integrative management of chronic renal failure - A case report
Dr Pankaj Chayyani
ABSTRACT
A 38-year-old male patient complained of bilateral pedal oedema, moderate breathlessness, and blurred vision along with severe generalized weakness and wet cough. The Biomedical diagnosis was made based on the USG as bilateral medical-renal disease[1] along with bilateral moderate to gross pleural effusion. His serum creatinine level was recorded as 21.5mg/dl. Patient was then referred to higher centre for haemodialysis by the Nephrologist The patient underwent haemodialysis on daily basis from 26th March 2021 to 1st April 2021 supported with medications for symptomatic management. The haemodialysis schedule was changed to thrice a week for one month. Further he was suggested for renal transplant. The patient now consulted Dr Pankaj Chayyani and the Ayurvedic diagnosis made was Vrikka dosa [2]. As the tridosa are involved in the pathogenesis, the treatment was planned to address this along with Rasayana cikitsa, and Vasti karma. Specific allopathic medications were continued during Ayurvedic treatment. Haemodialysis was done when the clinical features of uraemia appeared, or the serum creatinine level was greater than 12. With Ayurvedic treatments, haemodialysis could be stopped completely, and serum creatinine was normal and stable. His symptoms of bilateral pedal oedema, breathlessness, blurred vision, generalised weakness, and wet cough were completely relieved.
KEYWORDS
Renal, kidney, renal failure, case report, integrative, vrikka dosa
INTRODUCTION
Chronic kidney disease (CKD) arises from many heterogeneous disease pathways that alter the function and structure of the kidney irreversibly, over months or years. Diabetes and hypertension are the main causes of CKD. Many people are asymptomatic, and present after chance findings from screening tests—for example, through a routine medical examination or check-up—or not until they become unwell with advanced CKD. However, depending on the cause of CKD, the symptoms may present directly because of impaired kidney function.
Diagnostic Criteria- Renal ultrasound is generally considered the preferred first-line imaging technique for the assessment of people with previously undiagnosed kidney dysfunction. Diagnostic criteria include 1 or more of the following: (1) GFR less than 60 mL/min/1.73 m2; (2) albuminuria (ie, urine albumin ≥30 mg per 24 hours or urine albumin-to-creatinine ratio [ACR] ≥30 mg/g); (3) abnormalities in urine sediment, histology, or imaging suggestive of kidney damage; (4) renal tubular disorders; or (5) history of kidney transplantation. Based on previous treatment records and the clinical examination, the clinician diagnosed this patient as Chronic Renal Failure.
PATIENT INFORMATION
A 38-year-old male patient complained of bilateral pedal oedema, moderate breathlessness, blurred vision, severe generalized weakness, and wet cough for 2 months.
Medical History: The patient was healthy until 26th March 2021. Two days before, he complained of bilateral pedal oedema, moderate breathlessness, blurred vision, and severe generalized weakness and wet cough. The patient was diagnosed with bilateral medical-renal disease along with bilateral moderate to gross pleural effusion. Serum creatinine level 21.5mg/dl. Patient was then referred to a higher centre for haemodialysis by the nephrologist The patient was treated with hemodialysis on daily basis from 26th March 2021 to 1st April 2021 along with other symptomatic allopathic treatment. After 1st April, the haemodialysis was done thrice a week for one month. The symptoms persisted in spite of treatments. Hence he was suggested renal transplant.
CLINICAL FINDINGS
Pedal edema+, pallor of tongue and sclera
TIMELINE
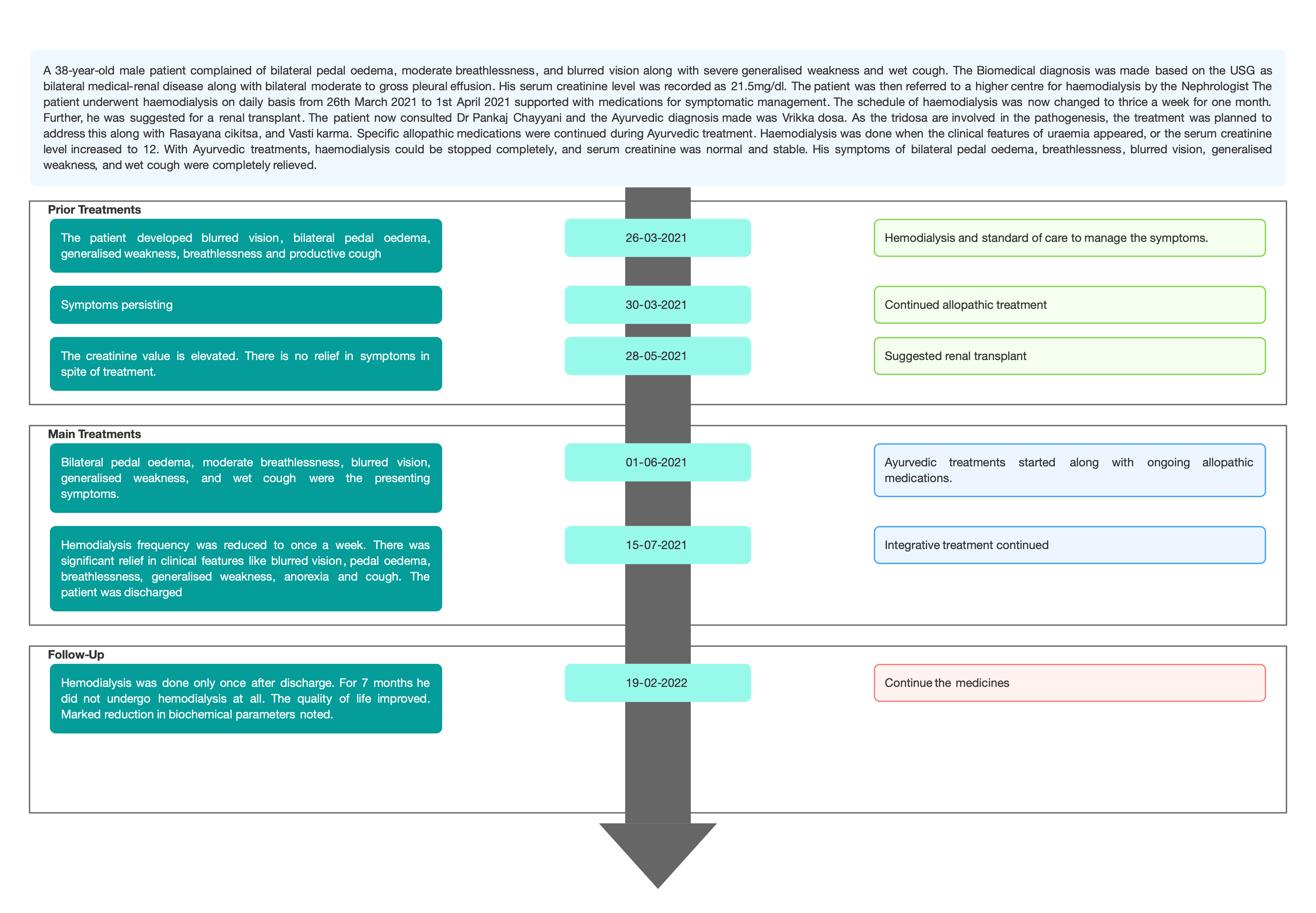
Image 1. Timeline of events added
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: USG abdomen confirmed the diagnosis as medical renal disease.
Image 2. USG abdomen is attached below
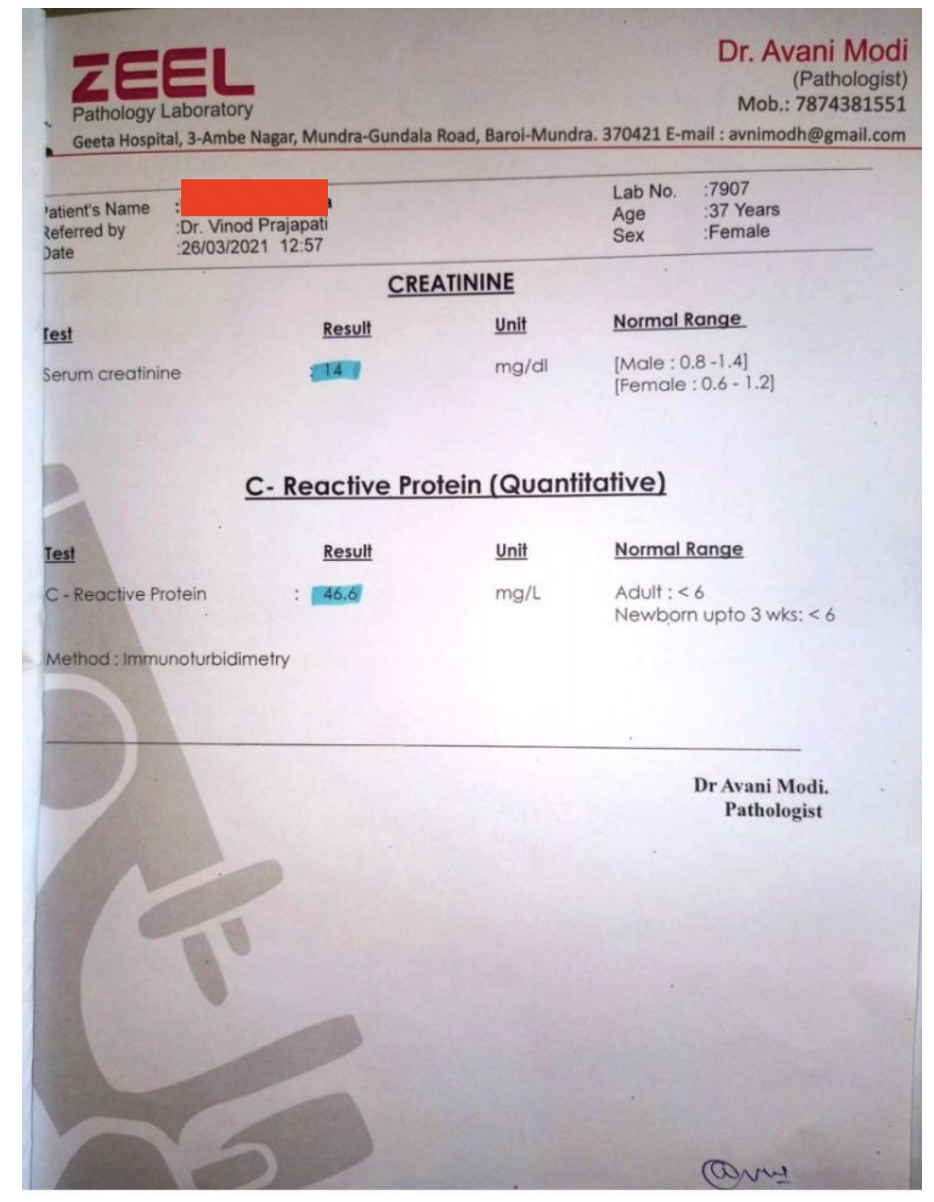
Image 3. Creatinine and CRP values recorded at baseline added below
Ayurvedic Assessment was done based on the clinical evaluation by the ayurvedic physician. The biomedical diagnosis was Chronic renal failure.
Differential Diagnosis- This does not apply as the patient came in with a definite diagnosis.
Prognosis- Chronic renal failure or ESRD (End stage renal disease) is a progressive, irreversible deterioration in renal function in which the body’s ability to maintain metabolic and fluid and electrolyte balance fails resulting in uremia or azotemia. With Ayurvedic treatment, hemodialysis could be stopped with a marked reduction in biochemical parameters.
THERAPEUTIC INTERVENTION
See the tab ‘Treatment details’
FOLLOW-UP AND OUTCOMES
Clinician-based assessment; The frequency of haemodialysis was reduced. For 7 months, the patient did not undergo haemodialysis. The serum creatinine level became normal and stable. The other parameters like Hb, urea, potassium, sodium, and phosphate also reduced significantly. The patient also got significant relief in clinical features like blurred vision, pedal oedema, breathlessness, generalised weakness, anorexia and cough
Patient assessed: Not relevant.
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported.
DISCUSSION ;
All three doṣas are involved in patients of chronic renal failure. Treatment is to be planned according to involved doṣas, rasayana cikitsa along with pancakarma mainly basti karma. Varunadi kvatha is helpful in kidney problems and it alleviates kapha and medas. Goksura is also effective and an established herb to manage kidney problems. Goksura is also balya aushadhi. Svadamstra rasayana is goksura bhavita goksura.Goksuradi gugglu is indicated in the treatment of mutraghata, mutrakricchra, prameha and disorders of vata. (Sharngadhara madhyama khanda adhyaya-7) Punarnva and iksumula have mutrala (diauresis) action and it is always beneficial to use herbs instead of modern loop diuretics as they can cause nephrotoxicity. Yavaksara also has mutrala effect and also helpful in gastric problems. Nagarjunabhra rasa and Javaharamohararasa are good for heart so both are given to improve cardiac function. The excretion of mutra and purisa is one function of apana. Both basti and nadi svedan improve apana function. Sharapunkha and bhumyamalaki have role in rakta dhatu formation by acting on liver. Basti through their effect on the seat of vata promote excretory function. Integrated effects of all therapies, medicaments, and wholesome food and behaviour may counteract the disease process and, to some extent, can also revert the process.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
The patient was suggested renal transplant owing to the non-satisfactory response to conventional medications. With ayurvedic treatment, the patient did not require haemodialysis for seven months. There was a marked reduction in his biochemical parameters. This case report demonstrated the successful integrative management of chronic renal failure. .
INFORMED CONSENT
Written consent obtained from patient’s parents.
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
1. Osborne CA, Low DG, Johnson KH. Renal disease. Vet Clin North Am. 1971 May;1(2):323-53.
2. Dr. Sharda Tak and Prof. Mahesh Chandra Sharma. Clinical study of “gokshuradi yoga” for the management of chronic renal failure. WJPR. Vol 6, Issue 16, 2017.
Image 1. Timeline
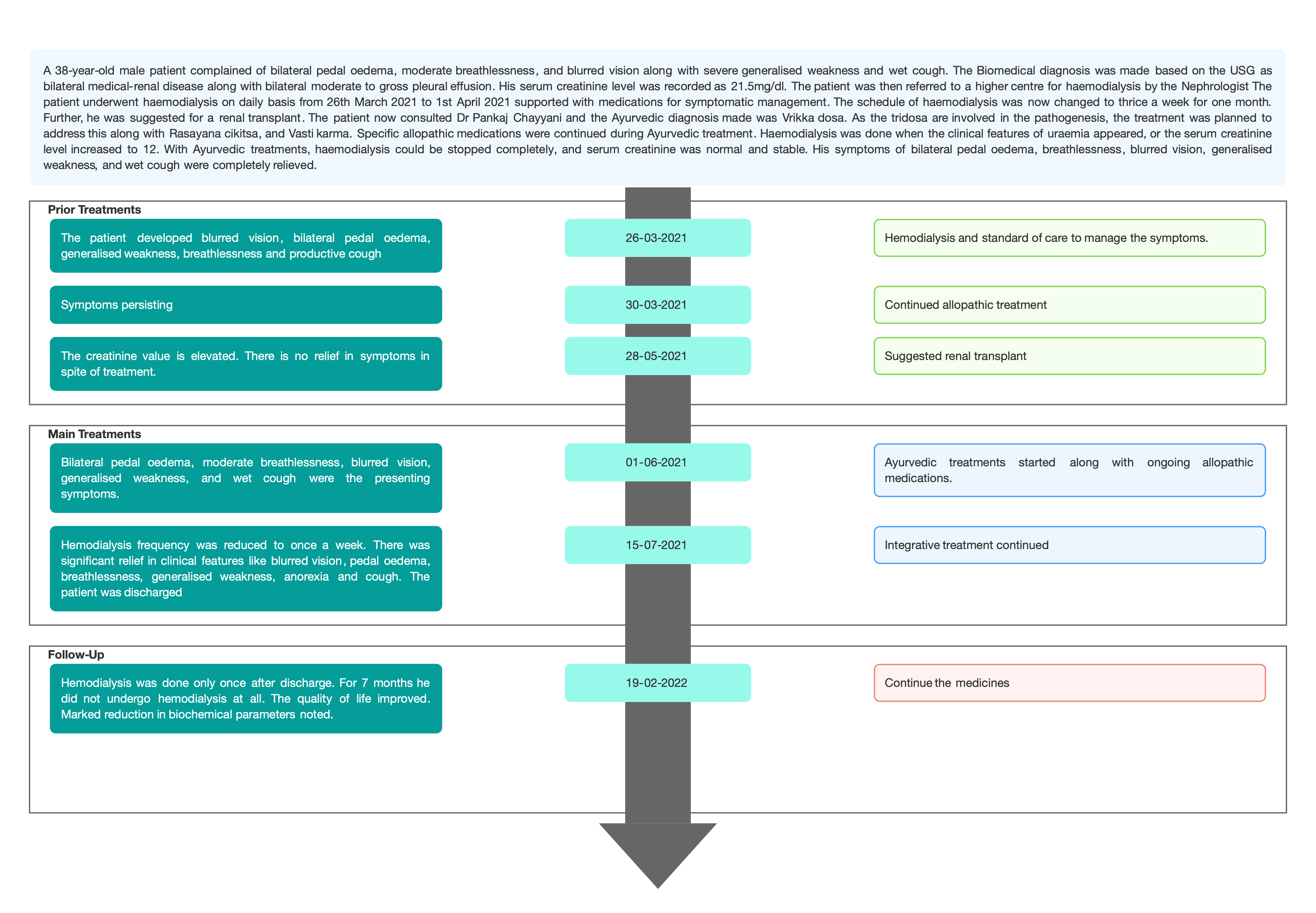
Image 2. USG abdomen dated 26.03.2021
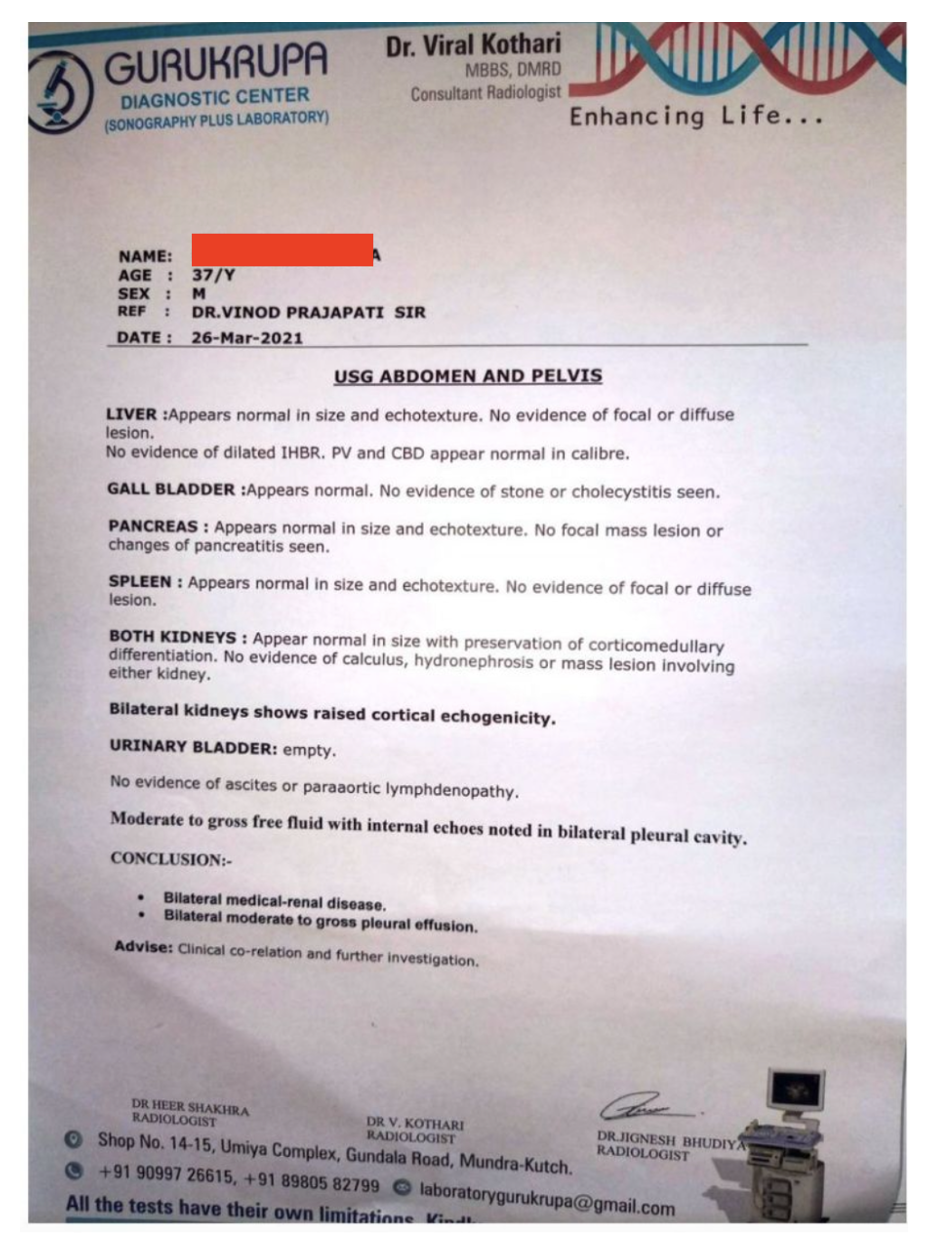
Image 3. Creatinine and CRP values recorded at baseline
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Chronic kidney disease
About the disease: Chronic kidney disease (CKD) arises from many heterogeneous disease pathways that alter the function and structure of the kidney irreversibly, over months or years. Diabetes and hypertension are the main causes of CKD. Many people are asymptomatic, and present after chance findings from screening tests—for example, through a routine medical examination or check-up—or not until they become unwell with advanced CKD. However, depending on the cause of CKD, the symptoms may present directly because of impaired kidney function.
Diagnostic criteria: Renal ultrasound is generally considered the preferred first-line imaging technique for the assessment of people with previously undiagnosed kidney dysfunction. Diagnostic criteria include 1 or more of the following: (1) GFR less than 60 mL/min/1.73 m2; (2) albuminuria (ie, urine albumin ≥30 mg per 24 hours or urine albumin-to-creatinine ratio [ACR] ≥30 mg/g); (3) abnormalities in urine sediment, histology, or imaging suggestive of kidney damage; (4) renal tubular disorders; or (5) history of kidney transplantation.
Treatment: Most people reaching ESKD are treated with either hemodialysis or peritoneal dialysis. Approximately 56% of people with ESKD on dialysis are actively waiting for a kidney transplant, but demand outstrips availability, so only 25% receive a kidney whereas 6% die while waiting for a transplant each year.
Diagnosis of the case: The patient was pre-diagnosed with bilateral medical-renal disease with elevated serum creatinine level. Based on previous treatment records and the clinical examination, the clinician diagnosed the case as Chronic Renal Failure.
Prognosis: CKD has varying levels of presentation. It usually gets worse over time though treatment has been shown to slow the progression. If left untreated, CKD can progress to kidney failure and early cardiovascular disease. In this case, with add-on Ayurvedic treatments, the frequency of undergoing hemodialysis was reduced to once a week. In further follow-ups, the condition improved, and the patient could stop the dialysis for seven months with a marked reduction in biochemical parameters.
Image 1. Diagnosis proof document- USG abdomen report dated 26.3.2021 added below
-
Ayurveda Diagnosis
AYURVEDIC DIAGNOSIS: Vrikka dosha
ABOUT THE DISEASE: An exact explanation for Chronic kidney disease (CKD) cannot be obtained in the classical ayurvedic textbooks, but dispersed fragments of the disease can be traced in various chapters.
In Sushruta samhita, Sharira Sthana kidney has been mentioned as a Matruja Avayava which is made up of Rakta and Medo Dhatus.
Acharya Caraka and Sushruta, have considered Vrikka as the source of origin of medovaha srotas.
मेदोवहानाम् स्रोतसां वृक्कौ मूलं वपावहनं च ॥८॥ (Ca. Vi.5)
The dosha prakopaka hetu like nidanarthakara, santarpanajanya, apatarpanjanya and ajeerna avastha leads to agni dushti and therefore vitiation of samana vayu, pachaka pitta and ranjaka pitta occurs with the aggravation of kledaka kapha. The sthansamshraya of the prakupita dosha happens in vrikka and mutrashaya through vyana vayu leading to the srotodushti of dhatus, mala and oja which results in apana vayu vitiation. Thus the vrikka roga manifests.
Management:
According to Acarya Sushruta, vrikka is formed from Rakta and Medodhatu. Ahaara is converted to Rasa Dhatu and further converted to Raktadi remaining Dhatus. So, the line of treatment should focus on Jatharagni correction, which gives strength to Dhatwagnis, leading to the formation of fine quality Rasadi Dhatus. Shamana dravyas prescribed should focus on Rakta and Medodhatu, leading to the formation of Saara Bhaaga of both the Dhatus leading to proper nourishment of Vrikka. After Shamana Cikitsa, shodhana chikitsa is recommended.
The 38 year old male patient presented with blurred vision, bilateral pedal oedema, generalised weakness, breathlessness and productive cough. The patient was pre-diagnosed with bilateral medical-renal disease along with bilateral moderate to gross pleural effusion on (26/03/2021) with a serum creatinine level of 14mg/dl and is under haemodialysis. He was recommended a renal transplant.
Based on the investigations, and clinical examination, the Ayurvedic diagnosis was given as Vrikka dosha. The physician planned the treatment according to the involved dosha. Varunadi kvatha is helpful in kidney problems, and it alleviates kapha and medas. Goksura is also an effective and established herb for kidney problems. Goksura is balya aushadhi. Svadamstra rasayana is goksura bhavita goksura.Goksuradi Guggulu is indicated in the treatment of mutraghata, mutrakricchra, prameha and disorders of vata. (Sharangadhara madhyama khanḍa adhyaya-7) Punarnava and iksumula have mutrala (diuresis) action, It is always beneficial to use herbs instead of modern loop diuretics as they can cause nephrotoxicity. Yavaksara also has a mutrala effect and is indicated in gastric problems. Nagarjunabhra rasa and Javaharamohararasa are good for the heart, so both are given to improve cardiac function. The excretion of mutra and purisha is one function of apana. Both basti and nadi svedana improve apana function. Sharapunkha and bhumyamalaki have role in rakta dhatu formation by acting on liver. Basti, promotes the excretory function. The integrated effect of all therapies, medicaments and wholesome food and behaviour may counteract the disease process and, to some extent, helps revert the process.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Varunadi kvatha Kashayam 40 ml twice a day Oral 2021-06-01 - 2021-07-15 Ch.Chi.26 Ikshumula Kvatha Kashayam 40 ml- twice a day Oral 2021-06-02 - 2021-07-15 Anubhuta Dravya Prayoga Goksuradi guggulu Tablet 3 tablets thrice a day Oral with water 2021-06-01 - 2021-07-15 Ch.Chi.26 Swadamshtra Rasayana Tablet 2 tablets twice a day Oral with water 2021-06-01 - 2021-07-15 AH. UTh.4 Rasayana curna + Sharapunkha curna Churna 2 gram- twice a day Oral with water 2021-06-01 - 2021-07-15 Ch. Chi. 1, Bhai. Ratnavali, Mutrakricchra Cikitsa Punarnava curna Churna 5 gram twice a day Oral with water 2021-06-02 - 2021-07-15 Anubhuta Dravya Prayoga Yavakshara Churna Twice a day Oral with water 2021-07-02 - 2021-07-15 Ch.Su.14 Nagarjunabhra rasa Tablet twice a day Oral with water 2021-06-09 - 2021-07-15 Ayurveda Sara sangraha, rasa rasayana Prakaran Javaharamohararasa Tablet twice a day Oral with water 2021-06-12 - 2021-07-15 Rasendra Sara Sangraha, Rasayoga) Uricare Tablet 2 tablet twice a day Oral with water 2021-06-01 - 2021-07-15 Ayurvedic proprietary Medicine) Tab. Regeno Tablet 2 tablet twice a day Oral with water 2021-06-01 - 2021-07-15 Ayurvedic proprietary Medicine Nadi svedana on lumbar region Swedana As desired by the physician External application 2021-06-01 - 2021-07-05 Punarnavadi Niruha Basti Basti 320ml External 2021-06-01 - 2021-07-15 Anubhuta yogam Brahmi ghrta Nasya 8 drops in each nostril Intranasal 2021-06-11 - 2021-07-15 Sahasrayogam. Ghrita prakaranam -
Outcome Measures
OUTCOME MEASURES
A 38-year-old male patient presented with blurred vision, bilateral pedal edema, generalized weakness, breathlessness, and productive cough for 2 months. The patient was pre-diagnosed with bilateral medical-renal disease along with bilateral moderate to gross pleural effusion before 2 months and is undergoing hemodialysis, thrice a week. Due to unsatisfactory response to allopathic treatments, elevated serum creatinine and deranged biochemical parameters, the patient was recommended renal transplant. During the treatment, serum creatinine, urine output, and other biochemistry reports were assessed.
Table 1. Symptoms tabulated before and after treatment
CHIEF COMPLAINTS ( BEFORE
TREATMENT) – 01/06/2020
AFTER TREATMENT (On 22/01/2022)
Blurred vision
Moderate improvement
Bilateral pedal oedema
No edema
Breathlessness on mild exertion
No breathlessness at all
Generalized weakness
No weakness at all
Anorexia
No anorexia
Wet coughing
No coughing
Table 2. Frequency of Hemodialysis tabulated
Before admission
During Ayurveda
treatment
After Discharge
Every day from 26/03/2021 to 01/04/2021- total 7 times
Thrice a week from 03/04/2021 to
27/05/2021- total 10 times
Weekly once
· 07/06/2021
· 15/06/2021
· 26/06/2021
· 03/07/2021
Done only one time
· 02/08/2021
After that till today no dialysis
Table 3. Serum Creatinine level (mg/dl) (From the treating physician s notes)
Before admission
During admission
After discharge
26/03/2021- 21.5
01/06/2021- 7.7
02/08/2021- 2.81
27/03/2021- 16.77
07/06/2021- 13.6
16/08/2021- 6.2
28/03/2021- 19.68
14/06/2021- 12.7
14/09/2021- 5.6
29/03/2021- 19.93
24/06/2021- 11.9
16/11/2021- 4.5
30/03/2021- 20.91
03/07/2021- 12.9
10/12/2021- 5.1
31/03/2021- 12.37
14/07/2021- 9.0
03/01/2022- 4.6
01/04/2021- 15.36
22/01/2022- 4.0
27/05/2021- 7.56
12/02/2022- 3.31
28/05/2021- 7.55
31/05/2021- 9.48
Table 4. Biochemistry reports (Values documented in the treating physician s notes)
DATE
Hb (g/dL)
B. Urea (mg/dL)
S . K +
(mmol/ L)
S. Na
S . C l -
(mmol/ L)
S.Ca++
( m g / dL)
S.Phospha te (mg/dL)
26/03/2021
10
213.5
122
90.1
9.57
7.36
27/03/2021
3.88
124.4
90.6
28/03/2021
9.1
4.37
126.7
91.0
01/06/2021
10.8
37
4.3
130
102
8.9
3/6/2021
52
09/06/2021
10.9
55
4.3
140
98
9.0
14/06/2021
74
16/06/2021
10.5
44
4.1
141
101
9.0
24/06/2021
10.3
83
5.0
133
99
9.0
01/07/2021
8.7
79
5.0
135
102
8.4
07/07/2021
9.2
44
5.1
138
93
8.3
14/07/2021
9.0
71
5.4
136
96
8.6
19/02/2022
12.5
73
4.0
142
98.0
8.9
3.8
Table 5. Urine output during the hospitalisation period (ML/24 HOURS). From the treating physician s notes
· 01/06/2021- 300
· 02/06/2021- 200
· 03/06/2021- 330
· 04/06/2021- 300
· 05/06/2021- 460
· 06/06/2021- 360
· 07/06/2021- 350
· 08/06/2021- 300
· 09/06/2021- 300
· 10/06/2021- 330
· 11/06/2021- 430
· 12/06/2021- 420
· 13/06/2021- 430
· 14/06/2021- 450
· 15/06/2021- 450
· 16/06/2021- 450
· 17/06/2021- 360
· 18/06/2021- 360
· 19/06/2021- 300
· 20/06/2021- 410
· 21/06/2021- 710
· 22/06/2021- 450
· 23/06/2021- 510
· 24/06/2021- 600
· 25/06/2021- 710
· 26/06/2021- 750
· 27/06/2021- 700
· 28/06/2021- 630
· 29/06/2021- - (didn’t measure because of Fistuloplasty)
· 30/06/2021- -
· 31/06/2021- -
· 01/07/2021- 600
· 02/07/2021- 250
· 03/07/2021- 390
· 04/07/2021- 760
· 05/07/2021- 710
· 06/07/2021- 780
· 07/07/2021- 660
· 08/07/2021- 1050
· 09/07/2021- 890
· 10/07/2021- 880
· 11/07/2021- 1080
· 12/07/2021- 1500
· 13/07/2021- 1050
· 14/07/2021- 1100
· 15/07/2021- 1500
According to the patient urine output remained- 1500-1900ml/24 hours at home
-