Featured Case
-
Abstract
A 57-year-old female patient complained of reddish discolouration of bilateral lower limb along with severe pain associated with fever and chills on and off for 3 months. The complaints started with moderate pain and reddish discolouration associated with intermittent fever. At the onset of symptoms, she immediately consulted an Allopathic doctor and took medicines, but did not get relief. The symptoms worsened after treatment. She was stressed due to the pain and lack of sleep. Patient had a history of recurrent Urinary tract infection (UTI) and history travelling abroad (USA). The patient now approached Dr Rajeshwari for better care. Based on clinical examination and urine culture and sensitivity test, the Biomedical diagnosis was made as Klebsiella induced urinary tract infection [1] associated with cellulitis [2] and the Ayurvedic diagnosis was made as Pittaja mutrarkricchra [3] and ushnavata associated with Vrana shopha. The line of treatment followed was jvara and ama cikitsa. With ayurvedic treatments, patient got significant reduction in symptoms and routine laboratory investigation were within normal limits. Lower limb cellulitis was completely resolved with no bacteriuria on culture and sensitivity test. The follow up period was uneventful, and patient achieved complete relief without sequelae.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 57-year-old female patient complained of reddish discolouration of bilateral lower limb along with severe pain associated with fever and chills on and off for 3 months. The complaints started with moderate pain and reddish discolouration associated with intermittent fever. At the onset of symptoms, she immediately consulted an Allopathic doctor and took medicines, but did not get relief. The symptoms worsened after treatment. She was stressed due to the pain and lack of sleep. Patient had a history of recurrent Urinary tract infection (UTI) and history travelling abroad (USA). The patient now approached Dr Rajeshwari for better care. Based on clinical examination and urine culture and sensitivity test, the Biomedical diagnosis was made as Klebsiella induced urinary tract infection [1] associated with cellulitis [2] and the Ayurvedic diagnosis was made as Pittaja mutrarkricchra [3] and ushnavata associated with Vrana shopha. The line of treatment followed was jvara and ama cikitsa. With ayurvedic treatments, patient got significant reduction in symptoms and routine laboratory investigation were within normal limits. Lower limb cellulitis was completely resolved with no bacteriuria on culture and sensitivity test. The follow up period was uneventful, and patient achieved complete relief without sequelae.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Standalone Ayurvedic management of Klebsiella induced Urinary tract infection associated with Cellulitis- A Case report.
Dr Rajeshwari
ABSTRACT
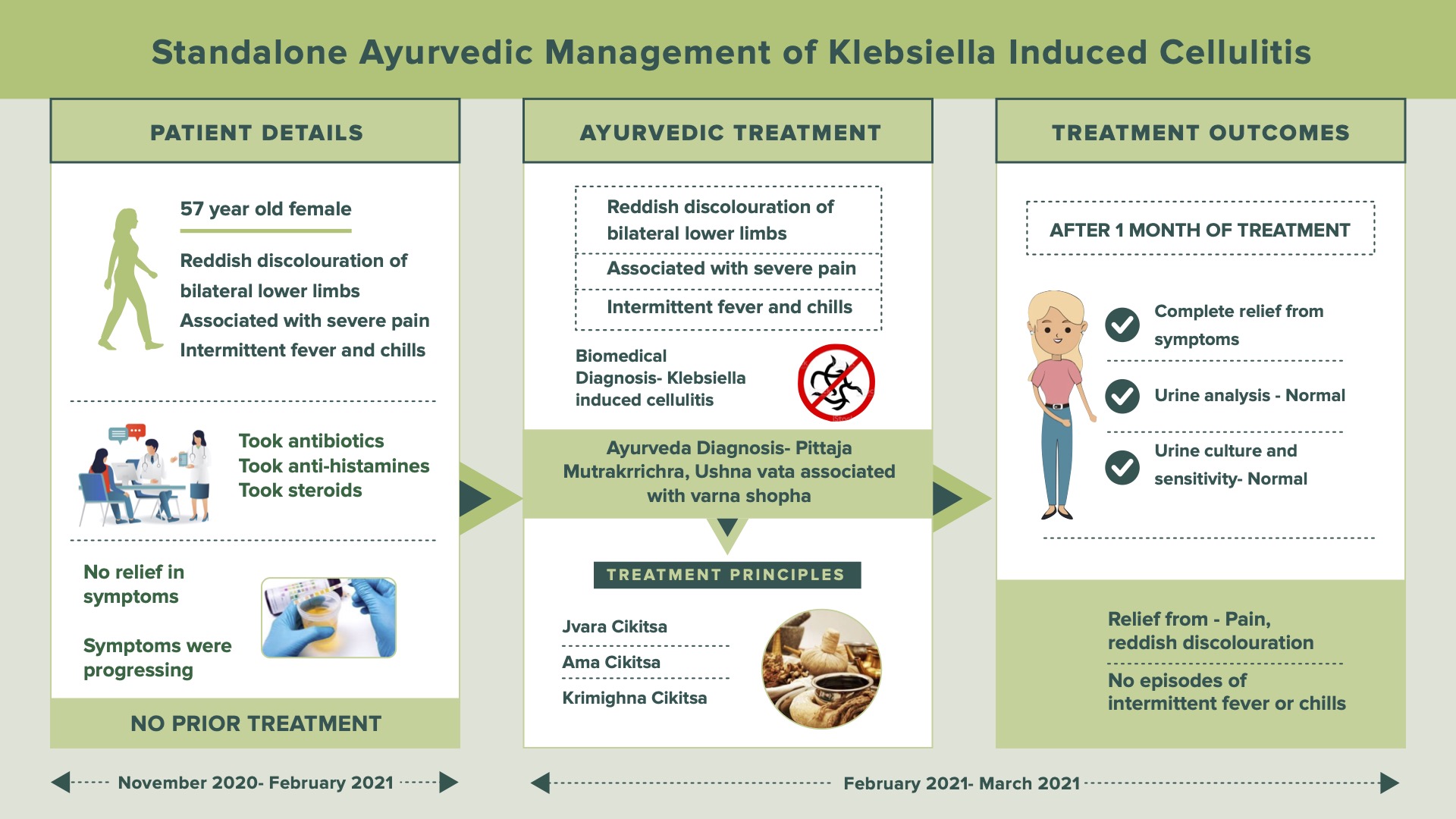
A 57-year-old female patient complained of reddish discolouration of bilateral lower limb along with severe pain associated with fever and chills on and off for 3 months. The complaints started with moderate pain and reddish discolouration associated with intermittent fever. At the onset of symptoms, she immediately consulted an Allopathic doctor and took medicines, but did not get relief. The symptoms worsened after treatment. She was stressed due to the pain and lack of sleep. Patient had a history of recurrent Urinary tract infection (UTI) and history travelling abroad (USA). The patient now approached Dr Rajeshwari for better care. Based on clinical examination and urine culture and sensitivity test, the Biomedical diagnosis was made as Klebsiella-induced urinary tract infection [1] associated with cellulitis [2] and the Ayurvedic diagnosis was made as Pittaja mutrarkricchra [3] and ushnavata associated with Vrana shopha. The line of treatment followed was jvara and ama cikitsa. With ayurvedic treatments, patient got significant reduction in symptoms and routine laboratory investigation were within normal limits. Lower limb cellulitis was completely resolved with no bacteriuria on culture and sensitivity test. The follow-up period was uneventful, and patient achieved complete relief without sequelae.
KEYWORDS
Klebsiella, Urinary tract infection, Cellulitis, Ayurveda management, Standalone, Ushnavata, Mutrkricchra
INTRODUCTION
Klebsiella is a type of bacteria commonly found in nature. In humans, the bacteria are often present in parts of the digestive tract where they do not generally cause health issues. In the United States, Klebsiella pneumoniae and Klebsiella oxytoca are the two strains responsible for most human sicknesses. Many Klebsiella infections are acquired in the hospital setting or in long-term care facilities. In fact, Klebsiella accounts for up to 8% of all hospital-acquired infections. People with a compromised immune system and/or people who have an implanted medical device (such as a urinary catheter or airway tube) are more at risk for Klebsiella infections. Extensive use of antibiotics has resulted in the development of antibiotic-resistant strains of Klebsiella. These infections can be more aggressive and difficult to treat. Whenever klebsiella gets into other areas of the body, it can lead to a range of illnesses, including pneumonia, bloodstream infections, meningitis, and urinary tract infections.
Diagnostic criteria: Urine Culture and sensitivity test, swab test
PATIENT INFORMATION
The 57 year old female patient complained of reddish discolouration of bilateral lower limb along with severe pain associated with fever and chills on and off for 3 months. Urine culture and sensitivity test confirmed the presence of Klebsiella.
Medical History: The complaint started with moderate pain and reddish discolouration with intermittent fever which affected her day-to-day activities as disease progressed. And she took allopathic treatment from November 17th, 2020, for the same complaints, with which the patient could not get any relief. Instead, the condition got worsened with the treatment. Due to the pain, she was stressed, and her sleep was disturbed. The patient had no co-morbidities. She had a history of Recurrent UTI and history of travelling abroad (USA). The patient does not have any other comorbidities.
CLINICAL FINDINGS/PHYSICAL EXAMINATION
On examination, tenderness, afebrile with chills, reddish discolouration of lower limbs was present. Afebrile, redness, swelling, rashes, tenderness were present.
Image 1. Baseline Image added below.
Image 2. Timeline of events added below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The images at baseline and the urine culture and sensitivity tests were the diagnostic parameters used.
Image 3. Investigations at baseline added below
Ayurvedic Assessment was done based on the investigation reports and the clinical evaluation by the ayurvedic physician.
Differential Diagnosis- The diagnosis was confirmed with urine culture and sensitivity tests.
Prognosis- There was a heavy bacterial load of Klebsiella species observed in the lab report before treatment. These bacteria are multiple drugs resistant which does not respond easily to conventional medicine as seen in this patient. With the initiation of the standalone ayurvedic treatment, the patient got a significant reduction in the clinical condition and complete relief from symptoms in 3 months.
THERAPEUTIC INTERVENTION
See the tab ‘Treatment details’
FOLLOW-UP AND OUTCOMES
Clinician-based assessment; Patient got significant reduction in symptoms and routine laboratory investigation were within normal limits. Lower limb cellulitis was completely resolved with no bacteriuria in the culture and sensitivity test. Follow up period was uneventful, and patient achieved complete relief without sequelae.
Patient assessed: Not relevant.
Image 4. During treatment and investigation added below
Image 5. After treatment and investigation report added below
Image 6. Follow up image added below
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events: None reported.
DISCUSSION ;
The management of cellulitis focuses mainly on the eradication of the infection. Cellulitis is a painful bacterial infection of the deeper layers of skin. It can start suddenly and become life-threatening without prompt treatment. The patient with a weakened immune system is especially vulnerable to contract cellulitis. Here, while treating cellulitis the patient had developed symptoms of UTI, from the lab report it was confirmed as an infection caused by a load of gram negative klebsiella species of bacteria namely; klebsiella pneumoniae & klebsiella oxytoca, through proper care patient got complete relief from all the symptoms. The main Ayurvedic principles like jvara cikitsa and ama cikitsa were followed strictly. And proper diet & healthy lifestyle was advised to the patient. Here, the conservative management were done focusing the pathogenic organism as mentioned by Caraka in krimighna cikitsa, Vimana sthana-Vyadhitharoopiyam adhyayam. Vardhamana pippali enhances the immune system. Dhatri mix and Chandraprabha Vati acts as a diuretic. Agnitundi Vati acts as amahara which corrects the agni. Krimisodhini vati, vidangarishtam and vilwadi gulika acts as krimihara. Mahasudarshan vati acts as jvarahara. Rasna manjistadi lepam for external application acts as daha hara. Dashamoola kashaya dhara for bahya shodhana. Snehapana & Virecana acts as abhyantara shodhana.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
The case report illustrates the utility of ayurveda concepts and efficacy of ayurvedic medicines in treating cellulitis caused by klebsiella infection which is having multiple drug resistance to commonly used antibiotics. In such scenario, ayurvedic intervention can be considered as an option to successfully manage multiple clinical conditions caused by drug resistant pathogens. It also raises the relevance in personal health care among the travellers.
INFORMED CONSENT
Written consent was obtained from the patient to publish the case report.
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
- Atay N, Uslu Gökceoğlu A. Evaluation of urinalysis and urine culture in children with first-time urinary tract infection. Turk J Urol. 2021 May;47(3):242-247.
- Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul 19;316(3):325-37.
- Namde MJ, Pathrikar AA, Kamat NM, Paradkar HS. Management of Pittaja Mutrakricchra by Ayurveda: A Case Study. A Case Study. Int. J. AYUSH CaRe. 2021; 5(1) Special issue:7-12
Image 1. Baseline image

Image 2. Timeline of events
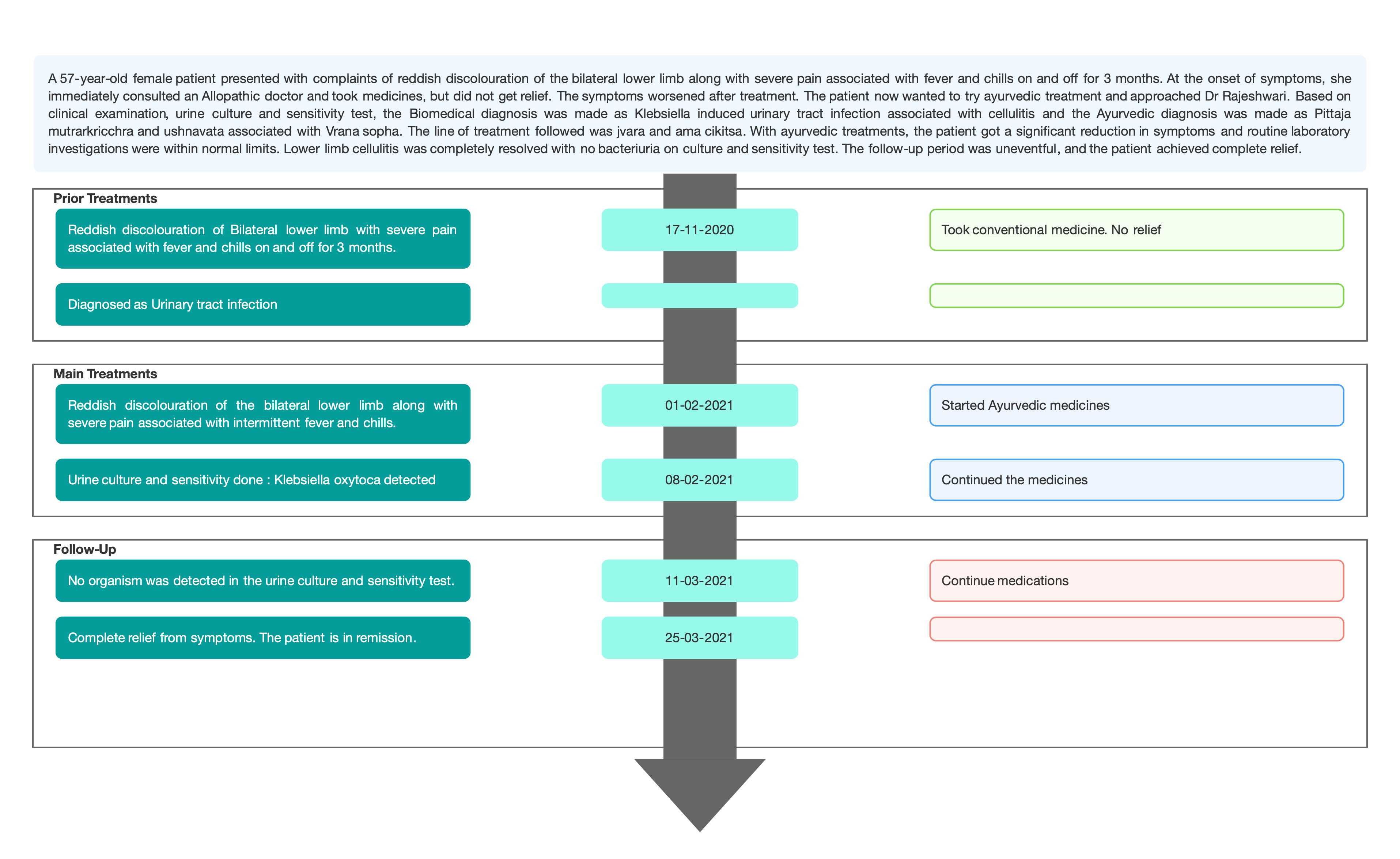
Image 3. Culture & Sensitivity report before treatment
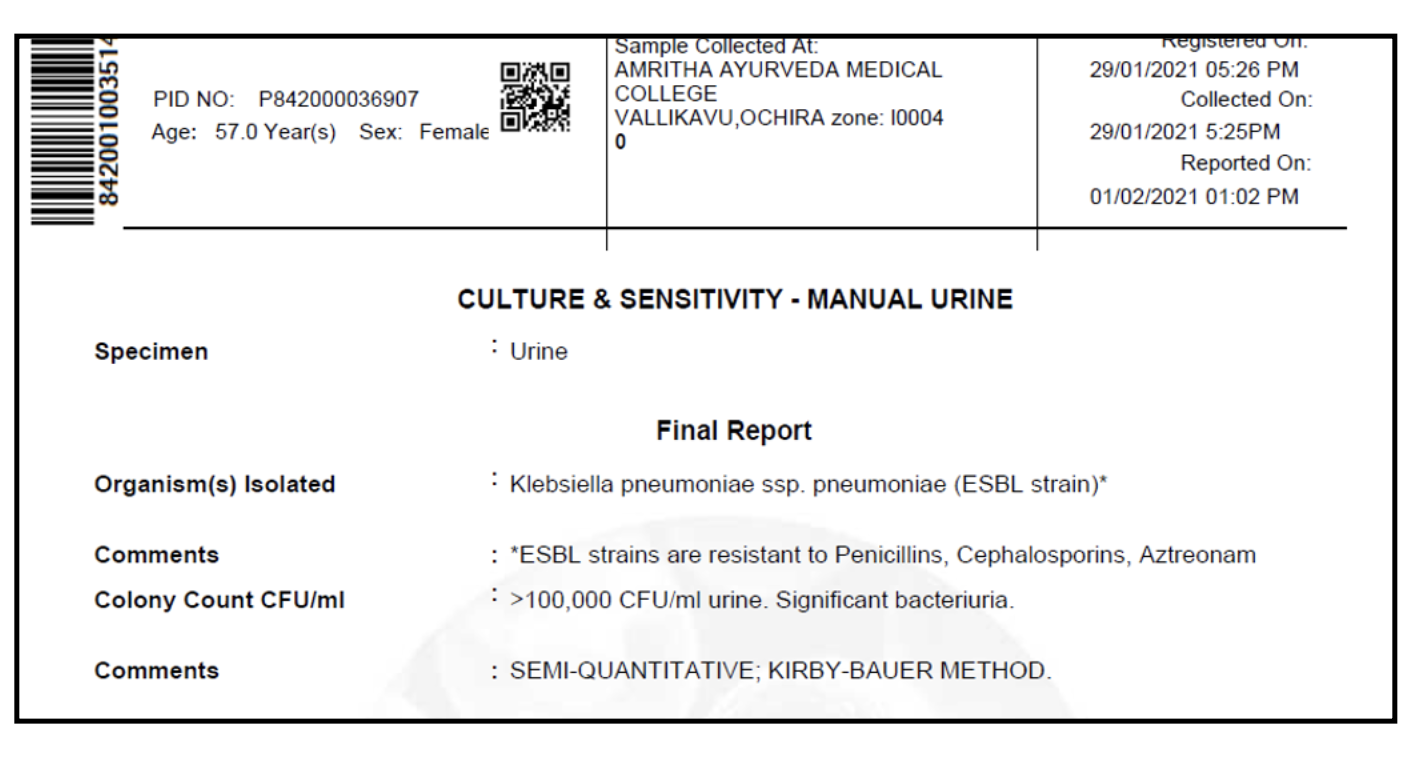
Image 4. Image taken during treatment and the culture & sensitivity report
 Image 5. Image taken after treatment and culture & sensitivity test report
Image 5. Image taken after treatment and culture & sensitivity test report 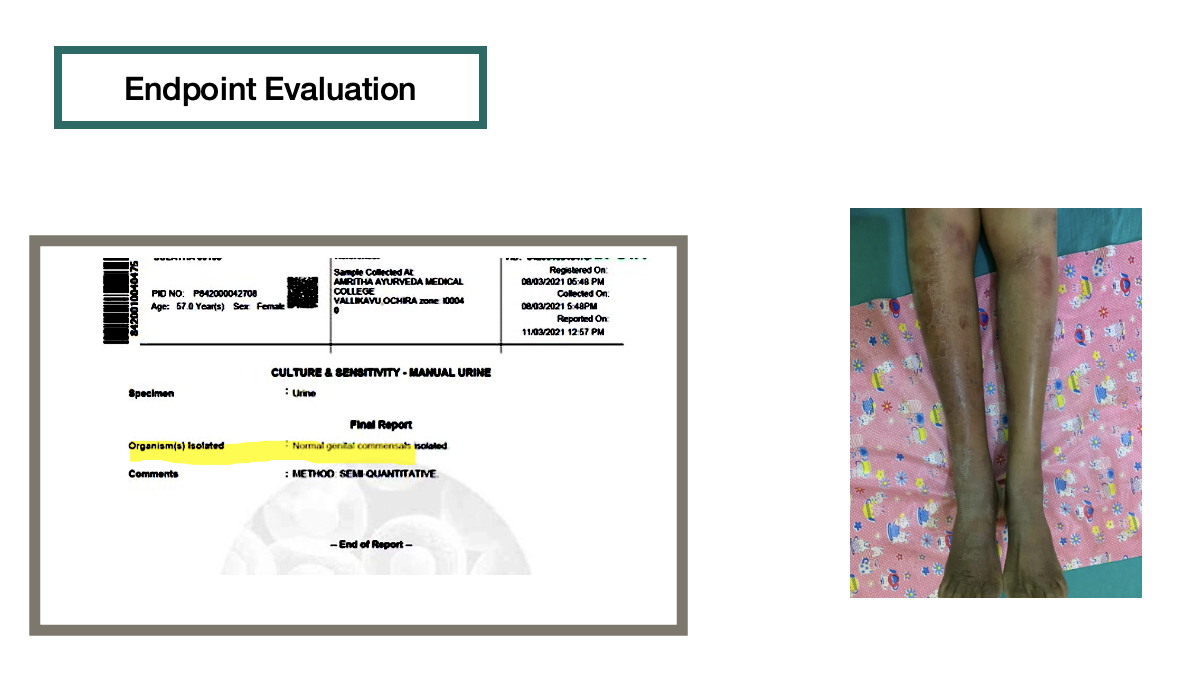
Image 6. Follow up image

-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Klebsiella induced Urinary tract Infection associated with cellulitis
ABOUT THE DISEASE:
Klebsiella is a type of bacteria commonly found in nature. In humans, the bacteria are often present in parts of the digestive tract where they do not generally cause health issues. In the United States, Klebsiella pneumoniae and Klebsiella oxytoca are the two strains responsible for most of the human sickness. Many Klebsiella infections are acquired in the hospital setting or in long-term care facilities. In fact, Klebsiella accounts for up to 8% of all hospital-acquired infections. People with a compromised immune system and/or people who have an implanted medical device (such as a urinary catheter or airway tube) are more at risk for Klebsiella infections. Extensive use of antibiotics has resulted in the development of antibiotic-resistant strains of Klebsiella. These infections can be more aggressive and difficult to treat. Whenever klebsiella gets into other areas of the body, it can lead to a range of illnesses, including pneumonia, bloodstream infections, meningitis, and urinary tract infections.
Prognosis: Klebsiella species bacteria are antibiotic resistant. Hence, the disease is difficult to cure when it affects different organ systems at a particular time. The prognosis of Klebsiella pneumonia is poor, especially in patients who are alcoholic, diabetic, have nosocomial infection or have septicemia.
The 57 years old female patient complained of reddish discolouration of the bilateral lower limb along with severe pain associated with fever and chills on and off for 3 months. Urine culture and sensitivity test confirmed the presence of Klebsiella. Hypothetically, in this patient, the pathogen first affected the urinary tract causing infection and later on spread to the skin causing cellulitis.
Diagnostic Criteria: Urine Culture and sensitivity test, swab test
Treatment: Given the low occurrence of K. pneumoniae in the community, the treatment should follow standard guidelines for antibiotic therapy. Once infection with K. pneumoniae is either suspected or confirmed, antibiotic treatment should be tailored to local antibiotic sensitivities. Current regimens for community-acquired K. pneumoniae include a 14-day treatment with either a third or fourth-generation cephalosporin as monotherapy or a respiratory quinolone as monotherapy or either of the previous regimes in conjunction with an aminoglycoside. If the patient is penicillin-allergic, then a course of aztreonam or a respiratory quinolone should be undertaken. For nosocomial infections, a carbapenem can be used as monotherapy until sensitivities are reported.
Image 1. Culture and sensitivity test before treatment added below
Image 2. Image taken at baseline added below
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Pittaja mutrarkrchra & ushnavata associated with Vrana Shopha.
ABOUT THE DISEASE:
Pittaja mutrakrchra: UTI is a common, distressing, and rarely life-threatening condition. UTI is more common in females than males. The infection is usually caused by E. coli derived from bowel flora [2]. Less frequently, other organisms like Klebsiella, Enterobacter and Streptococci have been implicated as causative organisms [1] The symptoms of Urinary tract infection are similar to Mutrakricchra as described in Ayurveda. It is regarded as ‘dukhena or kricchrena mutrapravrutti’ i.e. painful micturition or emission of urine with difficulty or dysuria.The symptoms of Mutrakricchra are increased frequency, urgency, hesitancy, burning micturition, painful micturition and discolouration of urine. According to Acarya Caraka, there are 8 types of Mutrakricchra. In this patient, the mutrakricchra has been identified with that of pitta aggravation
Ushnavata: Susruta mentions ushnavata as a type of mutraghata (urinary obstruction). Heavy exercise, and long walk under extreme sunlight cause the aggravation of pitta and vata dosha. The aggravated doshas are lodged in the urinary pathway. There, it causes inflammation in the nearby areas - bladder, urethra, rectum etc. This leads to yellowish urine or blood-mixed urine. In this condition, the individual passes urine with difficulty (dysuria) and frequently. There is also associated severe pain.
Vrana shopha: The Vrana shopha is described as an earlier phase of Vrana. Sushruta explains in detail about Vrana shopha. There are 3 stages of progression in vrana shopha. The stages are Amavastha (early stage of the inflammatory process), Pachyamanavastha (true inflammatory stage) and Pakvavastha (suppurative stage) respectively. Based on the vitiation of dosha, Sushruta has described Vrana shopha into 6 types: Vatika, Paittika, Kaphaja, Shonita, Sannipattaja and Agantuja. Diagnosis made according to the three progressive stages helps manage the condition easily. According to Sushruta, if the doshas are eliminated in the stage of accumulation, they will not progress to the further stages of pathogenesis, otherwise, in the later stages, they would become more severe.
This patient, with a history of travelling abroad, accompanied by poor hygiene, led to infection with klebsiella-induced UTI further affecting the skin and causing cellulitis.
Treatment: Here, a combination of formulations and therapies was planned as the clinical diagnosis is a combination of mutrakricchra, and ushnavata with vrana shopha.
Reference
- Namde MJ, Pathrikar AA, Kamat NM, Paradkar HS. Management of Pittaja Mutrakricchra by Ayurveda: A Case Study. A Case Study. Int. J. AYUSH CaRe. 2021; 5(1) Special issue:7-12.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Dhatri mix Churnam 2 tsp BD Oral, hot water After food 2021-02-01 - 2021-02-06 Anubhuta yogam Chandraprabha vati Tablet 2 tablets BD Oral, before food 2021-02-01 - 2021-02-06 Ayurveda Sara Sangraha, 17th edition, page on.- 421 – 423 Vilwadi gulika Tablet 1 tablet OD Oral, before food 2021-02-01 - 2021-02-06 Ashtanga Hridaya, Utt. 36. 84 – 85 Mahasudarshanam tablet Tablet 1 tablet Stat Oral, After food 2021-02-01 - 2021-02-06 Siddha medicine Agnitundi vati Tablet 1 tablet BD Oral, After food 2021-02-01 - 2021-02-06 Bhaishajya ratnavali, Agnimandya Rogadhikara Vardhamana pippali rasayana Churnam 12 gm Oral, with 1 glass lukewarm milk early morning on empty stomach 2021-03-19 - 2021-03-19 Caraka. Ci.1.3. Verse 36-40 Vardhamana pippali rasayana Churnam 9 gm Oral, with 1 glass lukewarm milk early morning on empty stomach 2021-03-20 - 2021-03-20 Vardhamana pippali rasayana Churnam 6 gm Oral, with 1 glass lukewarm milk early morning on empty stomach 2021-03-21 - 2021-03-21 Vardhamana pippali rasayana Churnam 3 gm Oral, with 1 glass lukewarm milk early morning on empty stomach 2021-03-22 - 2021-03-22 Vardhamana pippali rasayana Churnam 3 gm Oral, with 1 glass lukewarm milk early morning on empty stomach 2021-03-23 - 2021-03-23 Vardhamana pippali rasayana Churnam 6 gm Oral, with 1 glass lukewarm milk early morning on empty stomach 2021-03-24 - 2021-03-24 Vardhamana pippali rasayana Churnam 9 gm Oral, with 1 glass lukewarm milk early morning on empty stomach 2021-03-25 - 2021-03-25 Vardhamana pippali rasayana Churnam 12 gm Oral, with 1 glass lukewarm milk early morning on empty stomach 2021-03-02 - 2021-03-02 Vidangaristam Aristam 20 ml, BD Oral, After food 2021-03-27 - 2021-04-04 AFI Krimishodhini vati Tablet 2 tablets BD Oral, Before food 2021-03-27 - 2021-04-04 Ayurvedic Proprietary medicine Dasamoola kashaya dhara Kasayam 5 litres Kasaya dhara - 45 mins for 7 days 2021-02-08 - 2021-02-14 Sahasrayogam, Kashaya Prakaranam Rasnamanjistadi lepam Lepam 10 gm 3 hrs Morning & Evening for 7 days 2021-02-08 - 2021-02-14 Anubhuta Dravya Prayoga Indukantha Gritham Snehapana 30 ml For 5 days 2021-03-12 - 2021-03-16 Sahasrayogam. Gritha Prakarana Avipathi Curnam Curnam 30 gm with hot water Sadyovirecana- Evening 7 pm, before food 2021-03-18 - 2021-03-18 Sahasrayogam, Curna Prakaranam Indukantham kashayam Kashayam 10 ml kashayam + 20 ml lukewarm water BD Oral, ,Before food 2021-03-25 - 2021-04-08 Sahasrayogam, Gritha Prakaranam (yoga made into kasaya) Krimishodhini vati tablet 2 BD with Kashaya Oral, Before food 2021-03-25 - 2021-04-08 Patent & Proprietary Medicine Agnitundi vati Tablet 2 BD Oral, Before food 2021-03-25 - 2021-04-08 Sahasrayogam, Gutika Prakaranam Vidangaristam Aristam 20 ml BD Oral, After food 2021-03-05 - 2021-04-08 -
Outcome Measures
Clinical Outcome
A 57-year-old female patient complained of reddish discolouration of the bilateral lower limb along with severe pain associated with fever and chills on and off for 3 months. The complaint started with moderate pain and reddish discolouration with intermittent fever which affected her day-to-day activities as the disease progressed. Though she tried allopathic medicines, she did not get relief. The symptoms were worsening, and she was getting stressed.
With the ayurveda treatment, she got a significant reduction in symptoms and routine laboratory investigations were within normal limits. Lower limb cellulitis was completely resolved with no bacteriuria on culture and sensitivity test, the follow-up period was uneventful, and the patient achieved complete relief from symptoms.
Disease modifying effect- The patient is in remission.
Image 1. Image taken during treatment added below
Image 2. Follow up image added below
-



 Image 5. Image taken after treatment and culture & sensitivity test report
Image 5. Image taken after treatment and culture & sensitivity test report