Featured Case
-
Abstract
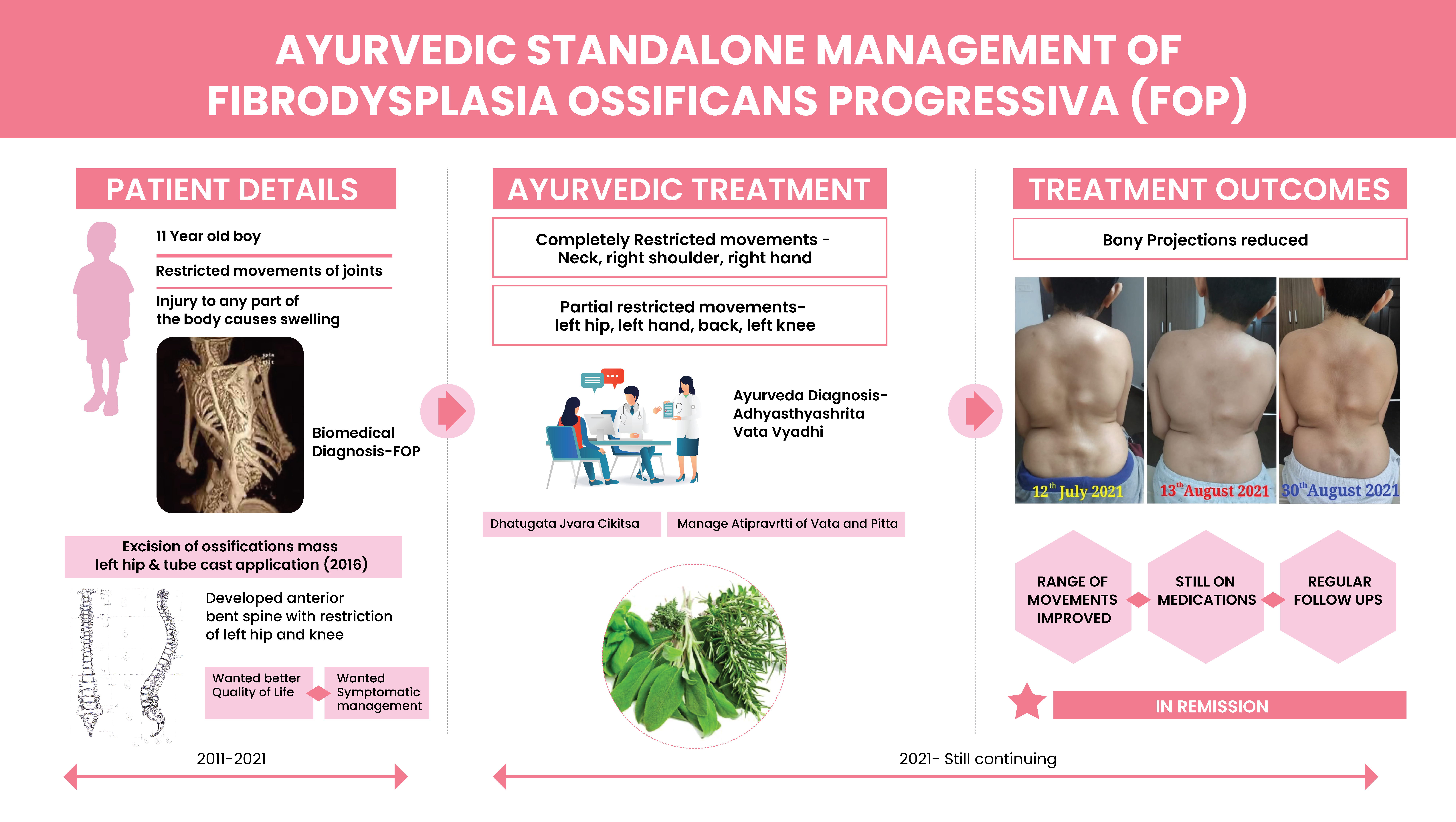
A 11-year-old boy was diagnosed with Fibrodysplasia Ossificans Progressiva. The biomedical diagnosis was confirmed with the gene test. The genomic DNA sample was analysed for mutations in the gene known to cause fibrodysplasia ossificans progressiva. At the age of 5, the kid had undergone open surgical correction by excision of ossifications mass on the left hip with tube cast application. Later, he developed bending of anterior spine with restriction of left hip and knee joint. Symptomatic management was done with standard of care. The parents wanted to try Ayurveda to improve the quality of life and so approached Dr KG Raveendran. The symptoms at the time of consultation were difficulty in lying down over the back, complete restricted movements of the neck, right shoulder and right hand. The patient also complained partial restriction of various other body parts due to deformity. There was also swelling in the joints. The Ayurvedic diagnosis was Adhyasthyashrita Vata Vyadhi and treatment was administered on the lines of Dhatugata Jvara Cikitsa. The patient underwent one and a half months of In-Patient Ayurvedic treatment. After Ayurvedic treatments, there were improvements in the range of movements in the lumbar, shoulder, cervical joints and right leg. The prominent bony projections in the back appeared to have reduced in size. There was a significant improvement in the Quality of Life. This case demonstrates the role of Ayurvedic intervention in improving quality of life in a progressive congenital disorder which has no effective treatment.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 11-year-old boy was diagnosed with Fibrodysplasia Ossificans Progressiva. The biomedical diagnosis was confirmed with the gene test. The genomic DNA sample was analysed for mutations in the gene known to cause fibrodysplasia ossificans progressiva. At the age of 5, the kid had undergone open surgical correction by excision of ossifications mass on the left hip with tube cast application. Later, he developed bending of anterior spine with restriction of left hip and knee joint. Symptomatic management was done with standard of care. The parents wanted to try Ayurveda to improve the quality of life and so approached Dr KG Raveendran. The symptoms at the time of consultation were difficulty in lying down over the back, complete restricted movements of the neck, right shoulder and right hand. The patient also complained partial restriction of various other body parts due to deformity. There was also swelling in the joints. The Ayurvedic diagnosis was Adhyasthyashrita Vata Vyadhi and treatment was administered on the lines of Dhatugata Jvara Cikitsa. The patient underwent one and a half months of In-Patient Ayurvedic treatment. After Ayurvedic treatments, there were improvements in the range of movements in the lumbar, shoulder, cervical joints and right leg. The prominent bony projections in the back appeared to have reduced in size. There was a significant improvement in the Quality of Life. This case demonstrates the role of Ayurvedic intervention in improving quality of life in a progressive congenital disorder which has no effective treatment.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Role of Ayurvedic intervention in improving the Quality of Life in a patient with Fibrodysplasia Ossificans progressiva - A Case report
Dr KG Raveendran
ABSTRACT
A 11-year-old boy was diagnosed with Fibrodysplasia Ossificans Progressiva1. The biomedical diagnosis was confirmed with the gene test. The genomic DNA sample was analysed for mutations in the ACVRI (NM_001105) gene known to cause fibrodysplasia ossificans progressiva. At the age of 5, the kid had undergone open surgical correction like excision of ossifications mass left hip and tube cast application and after which he had anterior bent spine with restriction of left hip and knee joint. Always, the symptomatic management was done with standard of care. The parents wanted to try Ayurveda to improve the quality of life and so approached Dr KG Raveendran. The symptoms were difficulty in lying down over the back, complete restricted movements of the neck, right shoulder and right hand and partial restriction of various other body parts due to deformity, thus causing swelling. The Ayurvedic diagnosis was Adhyasthyashrita Vata Vyadhi and treatment was on the line of Dhatugata Jvara Cikitsa. The patient underwent one and a half months of In-Patient Ayurvedic treatment. Post Ayurvedic treatments, there were improvements in the range of movements in the lumbar, shoulder, cervical joints and right leg. The prominent bony projections in the back appeared to have reduced in size. There was a significant improvement in the Quality of Life. As this is a congenital disorder, with no known cure and is a progressive condition, regular Ayurvedic management is advised to maintain the quality of life.
KEYWORDS
Fibrodysplasia ossificans progressiva, Ayurveda, Adhyasthyashrita Vatavyadhi, Ossification, Gene Mutation Test
INTRODUCTION
Fibrodysplasia ossificans progressiva (FOP) is a clinical condition where, the muscle tissue and connective tissue (such as tendons and ligaments) are gradually replaced by bone, thus causing restricted movement. This can be seen in early childhood itself, where the neck and shoulders are initially affected followed by the other parts of the body and the limbs. They also develop breathing difficulties, eating difficulties etc....that disrupts their normal life.
Diagnostic criteria: The correct diagnosis of FOP can be made clinically even before radiographic evidence of heterotopic ossification is seen, if soft tissues lesions are associated with symmetrical malformations of the great toes. Definitive genetic testing of FOP is now available and can confirm a diagnosis of FOP prior to the appearance of heterotopic ossification. Clinical suspicion of FOP early in life on the basis of malformed great toes can lead to early clinical diagnosis, confirmatory diagnostic genetic testing (if appropriate), and the avoidance of harmful diagnostic and treatment procedures. Clinicians should be aware of the early diagnostic signs of FOP, which are congenital malformation of the great toes and episodic soft tissue swelling even before the appearance of heterotopic ossification. This awareness should prompt genetic consultation and appropriate testing3.
PATIENT INFORMATION
A 11-year-old presented with difficulty in lying down over the back. Complete restricted movements of neck, right shoulder and right hand and partial restriction of left hand, back region, left hip, and left knee. Difficult for him to remove his shirt or writing etc… Injury to any part of the body causes swelling which gradually transforms to a bone tissue. He was diagnosed with a rare genetic disorder Fibrodysplasia ossificans progressiva
Medical History: 11-year-old child born of a non-consanguineous marriage, Full Term Normal Vaginal Delivery cried immediately after birth with history of delayed milestones (neck holding at 6 months, roll over at 8 months, walking at 1 ½ years) was admitted here. He was a diagnosed case of Fibrodysplasia ossificans progressiva. As reported by father, the child was born with flat foot and malformed big toes bilaterally. After a month of his first birthday, his parents noticed a small mass over the lower part of head, which was hard on palpation. Consultant suggested the oedema, would subside on its own. But the mass gradually increased in size which sized down to neck with tenderness. Now they consulted an Orthopaedic surgeon and underwent Biopsy, which showed no deformity. Gradually parents noticed small hard bony projection over the back region and the Rheumatologist they consulted suggested of genetic disorder related to uncontrolled bone ossification. When, he was a baby, whenever he fell and had injury, the small swelling gradually would transform to a hard bony projection. This condition was diagnosed as fibrodysplasia ossificans progressiva (An autosomal dominant syndrome that usually arises by a new mutation, i.e.: the parents are normal). At the age of 5 years (2016), his left hip joint got locked completely and found extreme pain with no movements and found to have extra bony ossification over the left Hip joint. Underwent open surgical correction like excision of ossifications mass left hip & tube cast application and after which he had anterior bent spine with restriction of left hip & knee joint. At the age of 5 years (2016), his left hip joint got locked completely and found extreme pain with no movements and found to have extra bony ossification over the left Hip joint. Underwent open surgical correction like excision of ossifications mass left hip & tube cast application and after which he had anterior bent spine with restriction of left hip & knee joint.
Family History: None significant. Parents or close relatives do not have this condition.
PHYSICAL EXAMINATION/CLINICAL FINDINGS
General - Malformed bony projections over back, B/L shoulder joint, left knee and left hip joint. Anteverted bent spine with limping gait. General examination- Normal: Respiratory system- B/L Lung fields are clear: Cardiovascular system- S1, S2 Heard: Gastrointestinal system- No gas bloatedness: No Tenderness/ Organomegaly.
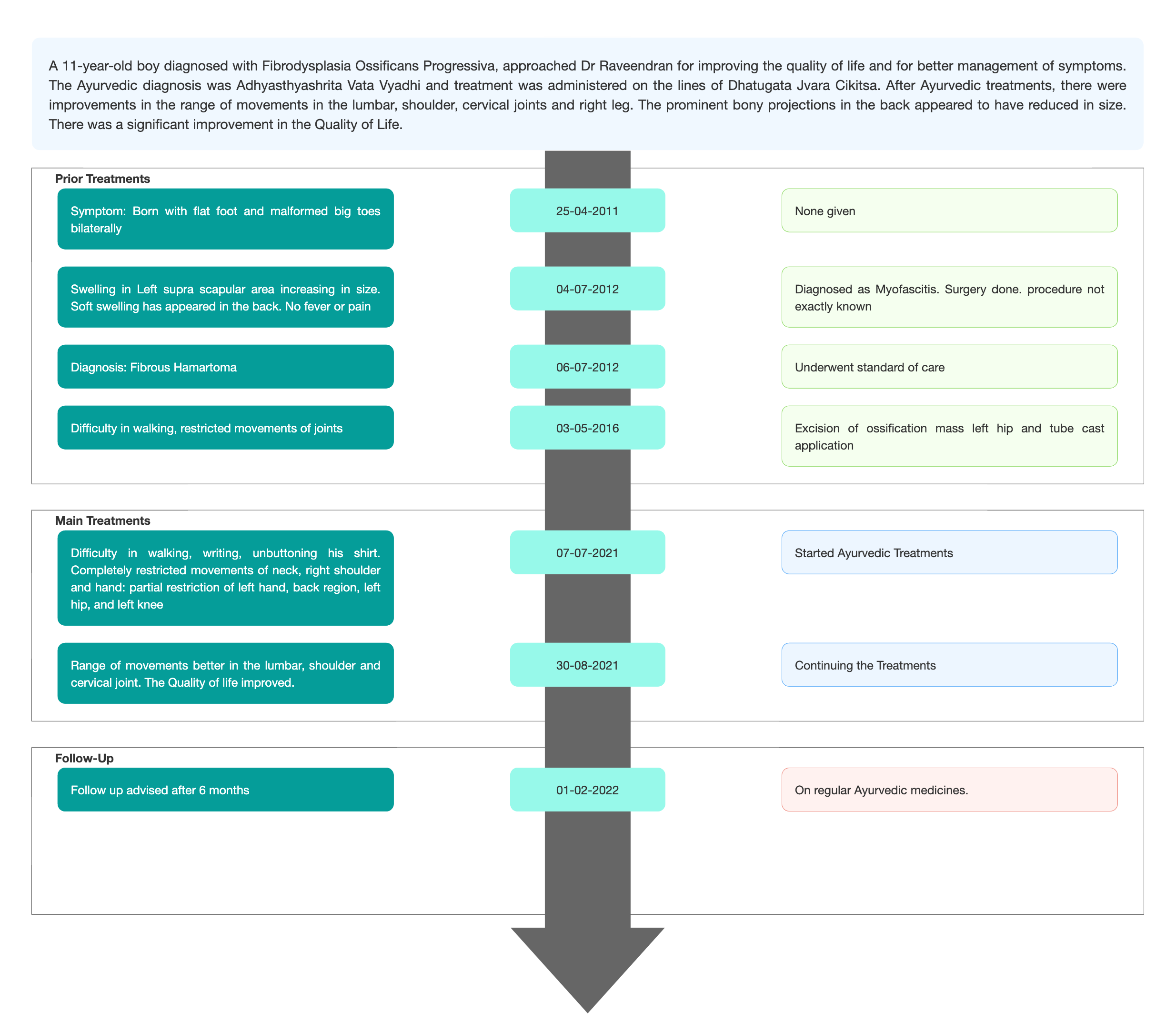
TIMELINE
Image 1. Timeline of events attached below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: AVCRI Gene test, Lab Investigations, Special Investigations were the basis for the Diagnostic criteria.
Image 2. Paediatric Surgery reports dated 2011
Image 3. Bone marrow image attached below
Image 4. Brain MRI attached below
Image 5. AVCRI Gene Test attached below
Image 6. Ultrasound scan Abdomen attached below
Image 7. Discharge Summary 2016 - Diagnosis Proof documents
Ayurvedic Assessment was done based on the clinical evaluation by the ayurvedic physician, and the confirmed diagnosis from the modern hospital.
Differential Diagnosis- This does not apply as the patient came in with a definite diagnosis.
Prognosis- Fibrodysplasia ossificans progressiva (FOP), a rare and disabling genetic condition characterized by congenital malformations of the great toes and progressive heterotopic endochondral ossification (HEO) which is the most catastrophic of HEO disorders in humans. Flare-ups of FOP are episodic; immobility is cumulative. This is a progressive disorder and can only be managed during the episodes. In this patient also, the kid had already undergone hip replacement surgery at the age of 6, and In patient admissions for fibrous hamartoma and Myofascitis.
THERAPEUTIC INTERVENTION
See the tab 'Treatment Details'
FOLLOW-UP AND OUTCOMES
The patient is advised to come for regular follow ups once every year and continue the Ayurvedic medicines to maintain the quality of life.
Clinician-based assessment: ROM better in Shoulder joint, SLR improved in the right side, Cervical Joint Right Rotation improved, Anteverted bent spine- slightly improved.
Subjective parameters: Range of movements in major affected joints was assessed at baseline and at the endpoint to measure the outcome.
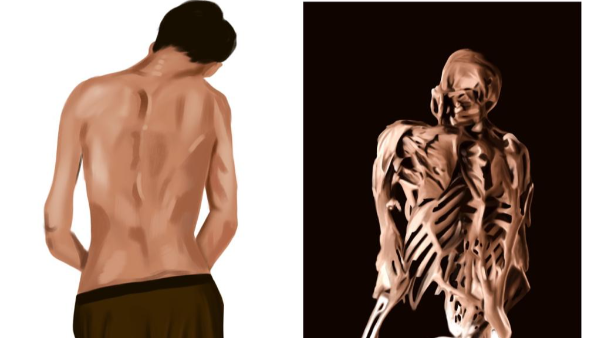
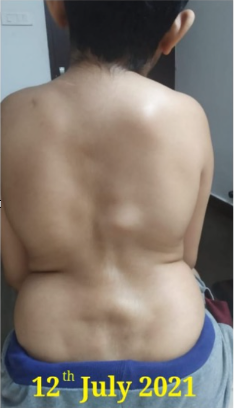
Image 8. Patient image at baseline and endpoint attached below
Patient-assessed: Not relevant
Follow up test results: No investigations or blood tests were done, as it was not deemed necessary.
Intervention adherence and tolerability: The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events: None reported
DISCUSSION:
This disease cannot be directly correlated to any disease mentioned in the classical text in Ayurveda. The treating physician has diagnosed the condition, based on the clinical presentation. The line of treatment was Dhatugata jvara cikitsa. This is basically a dhatvashrita vyadhi. Here the due to the increased formation of asthidhatvagni, dhatu transformation is not taking place properly, by that atipravritti of asthi dhatu is happening and again it is transformed as asthi dhatu only. So, the target was to reduce the atipravritti of both vata and pitta.
Overall Dhatugata jvara cikitsa, vatapittahara cikitsa, and asthi dhatu parinama hara cikitsa were followed for better management of the symptoms.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
FOP is a rare genetic disorder that is progressive with no known cure. This patient had tried managing the symptoms with conventional medicines, but the disease was rapidly progressing. So, they decided to try Ayurveda for better management and to improve the quality of life. With Inpatient treatments, there was an improvement in the range of movements, and a significant reduction in the bony projections. The patient is advised to regularly come for follow ups and continue the medications. Ayurvedic treatments can be recommended as an alternative treatment, for improving the quality of life in patients suffering from conditions like FOP with no known cure.
INFORMED CONSENT
Written consent obtained from patient.
ACKNOWLEDGEMENTS
None
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
1. Kaplan FS, Al Mukaddam M, Stanley A, Towler OW, Shore EM. Fibrodysplasia ossificans progressiva (FOP): A disorder of osteochondrogenesis. Bone. 2020 Nov;140:115539. doi: 10.1016/j.bone.2020.115539. Epub 2020 Jul 27. PMID: 32730934; PMCID: PMC7502483.
2. TUTTLE A. Myofascitis-a common cause of back pain. Hahnemannian. 1954 Jan-Mar;89(1):196-9. PMID: 13128531.
3. Fibrodysplasia Ossificans Progressiva: Diagnosis, Management, and Therapeutic Horizons . Pignolo et al. Pediatr Endocrinol Rev. 2013 June ; 10(0 2): 437–448)
Image 1. Timeline of events attached below
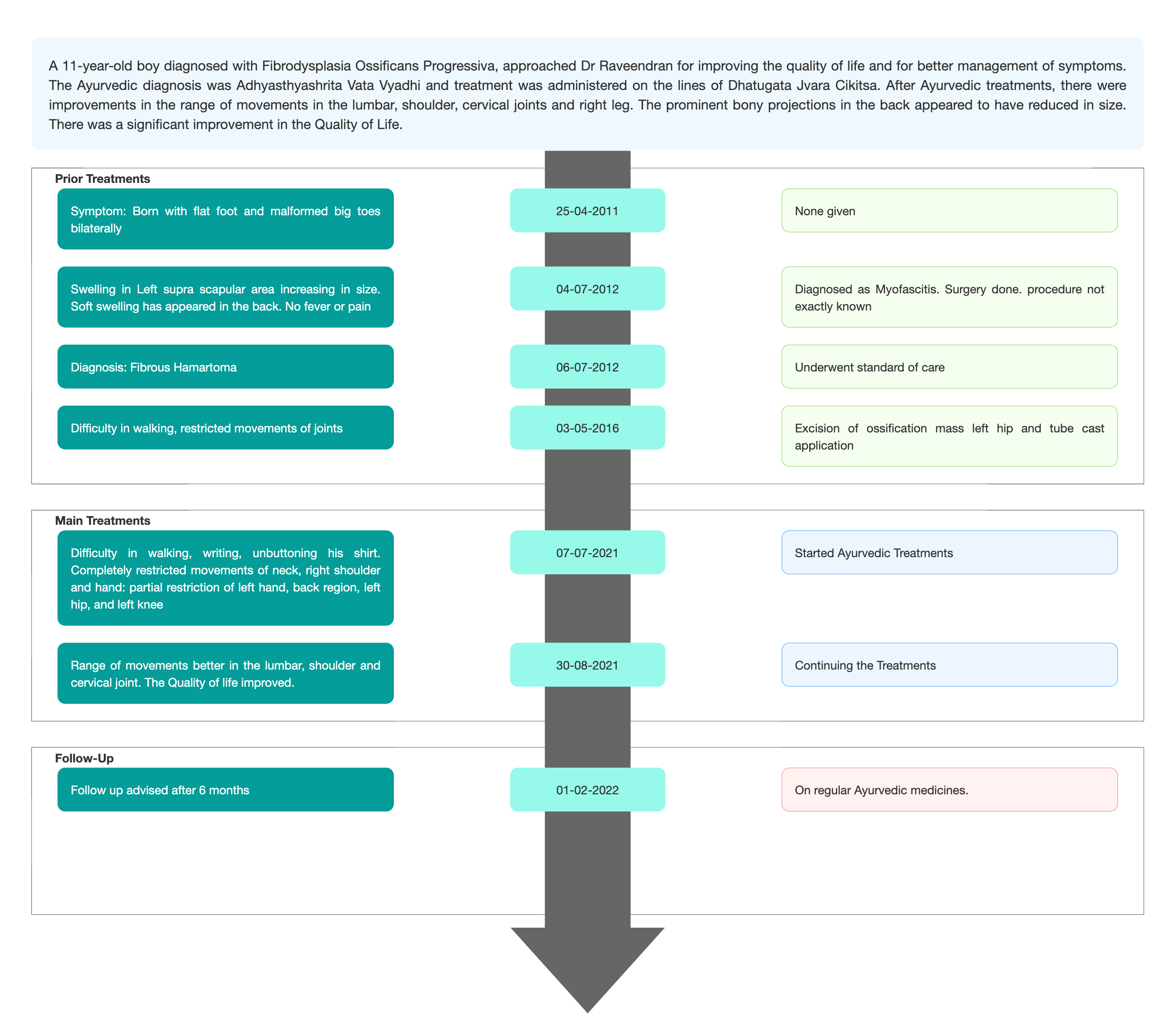
Image 2. Paediatric Surgery reports dated 2011
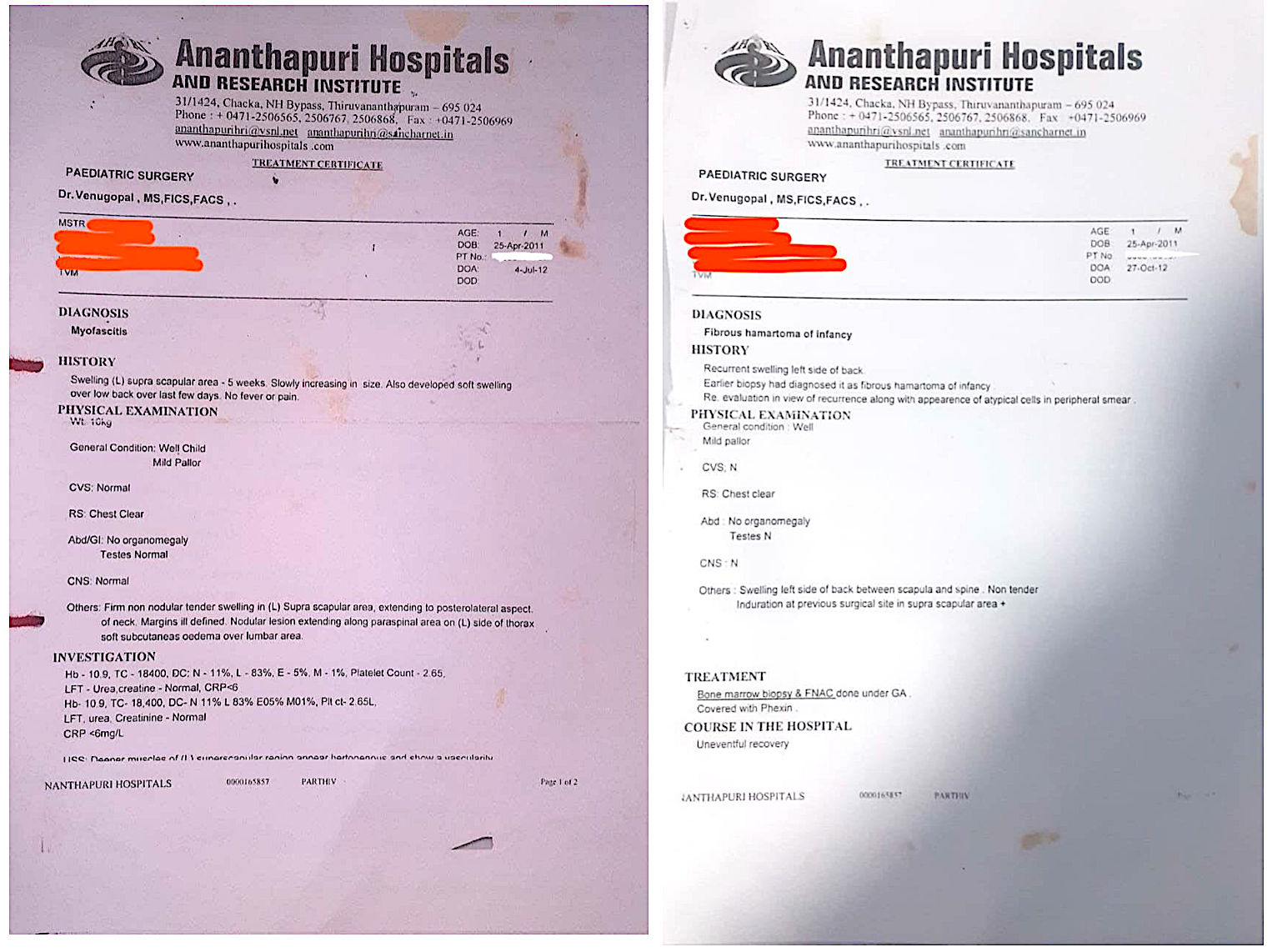
Image 3. Bone marrow image dated 2012
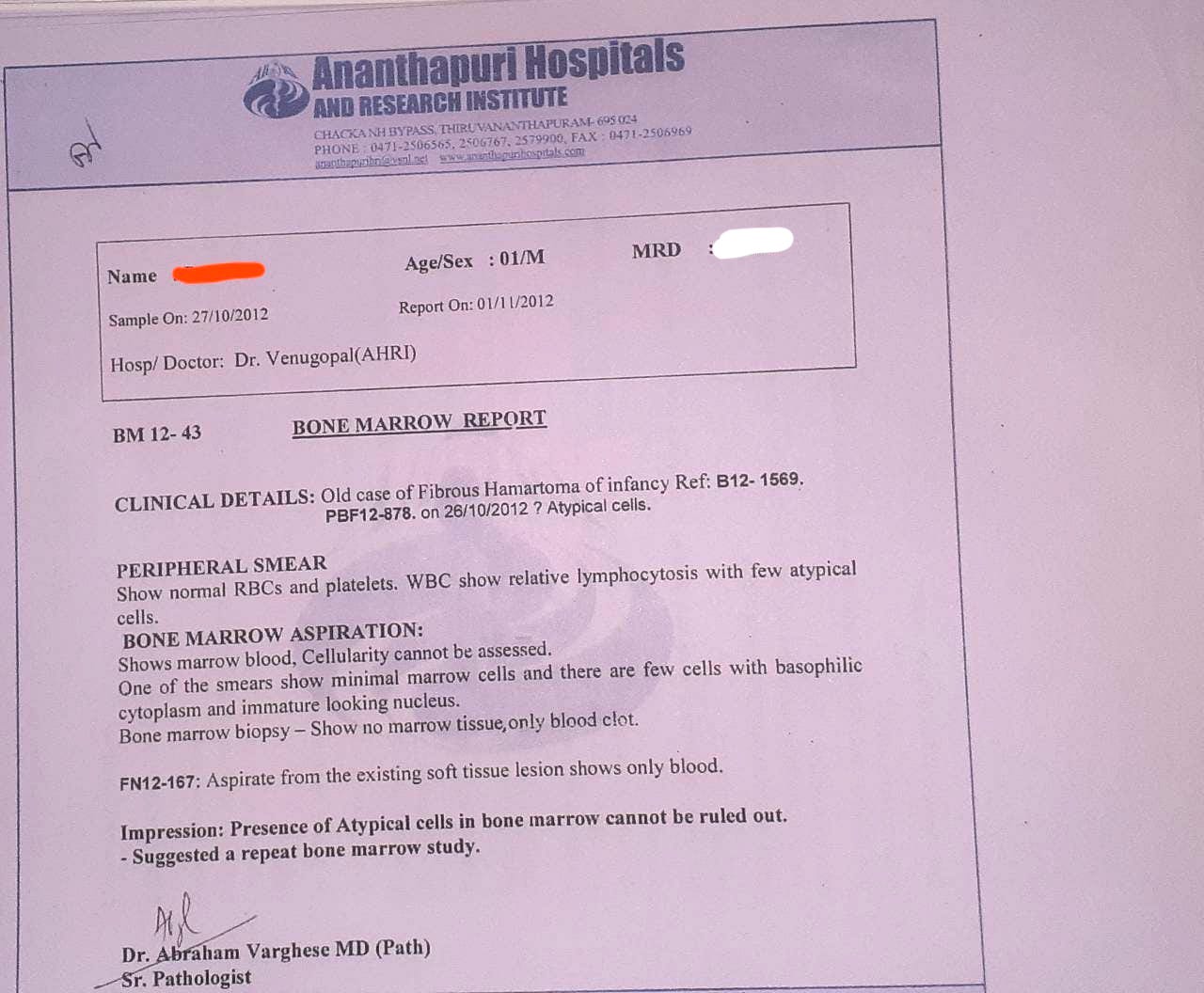
Image 4. Brain MRI dated 2014
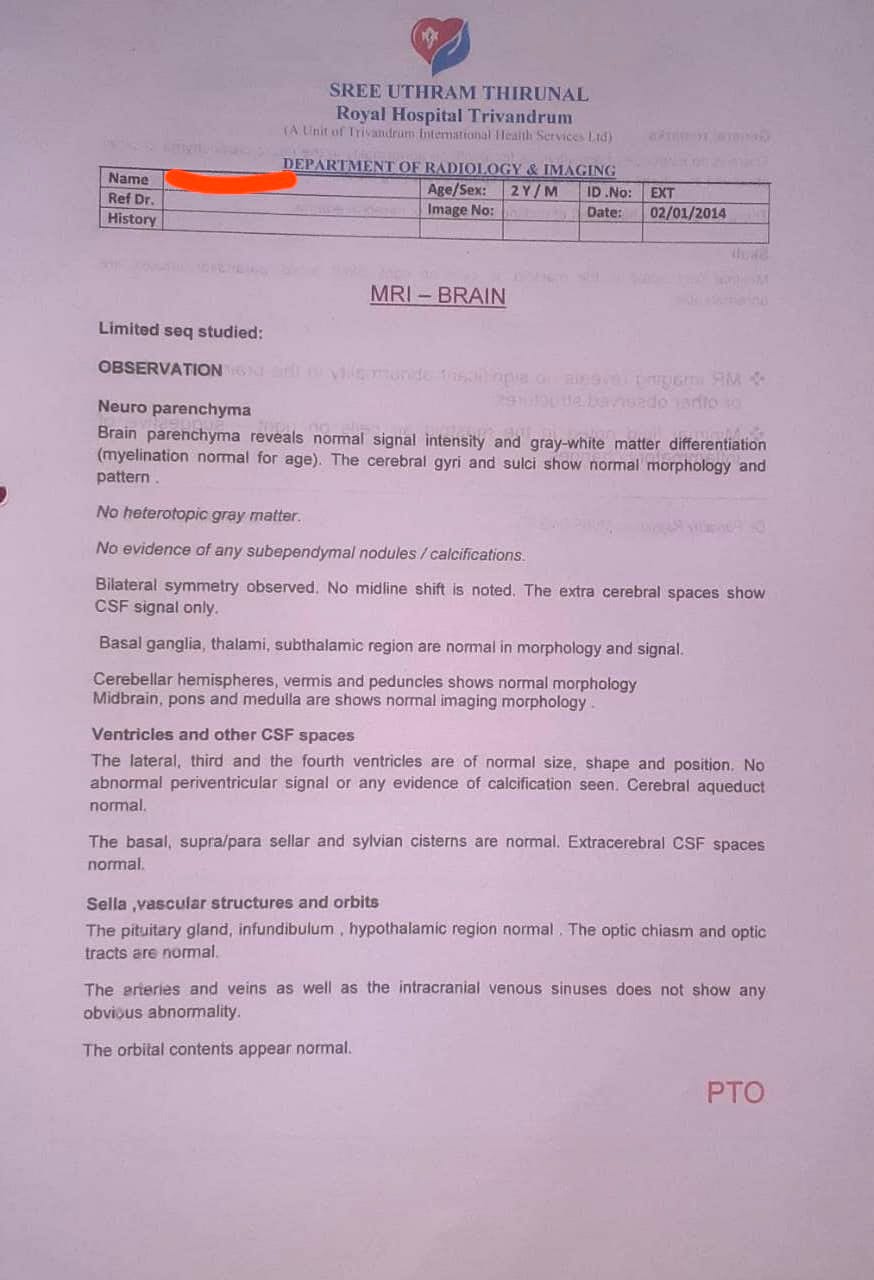
Image 5. AVCRI Gene Test dated 2015
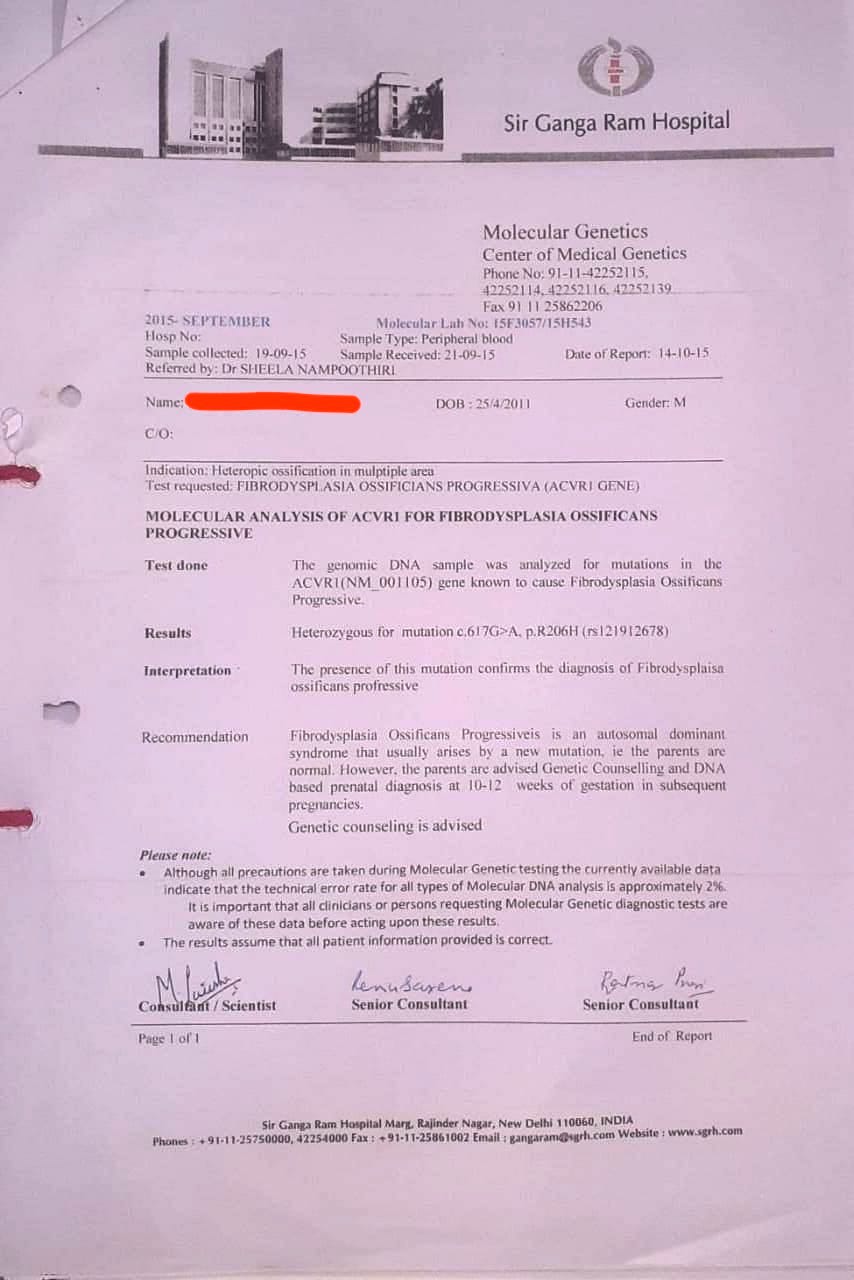
Image 6. dated 2015
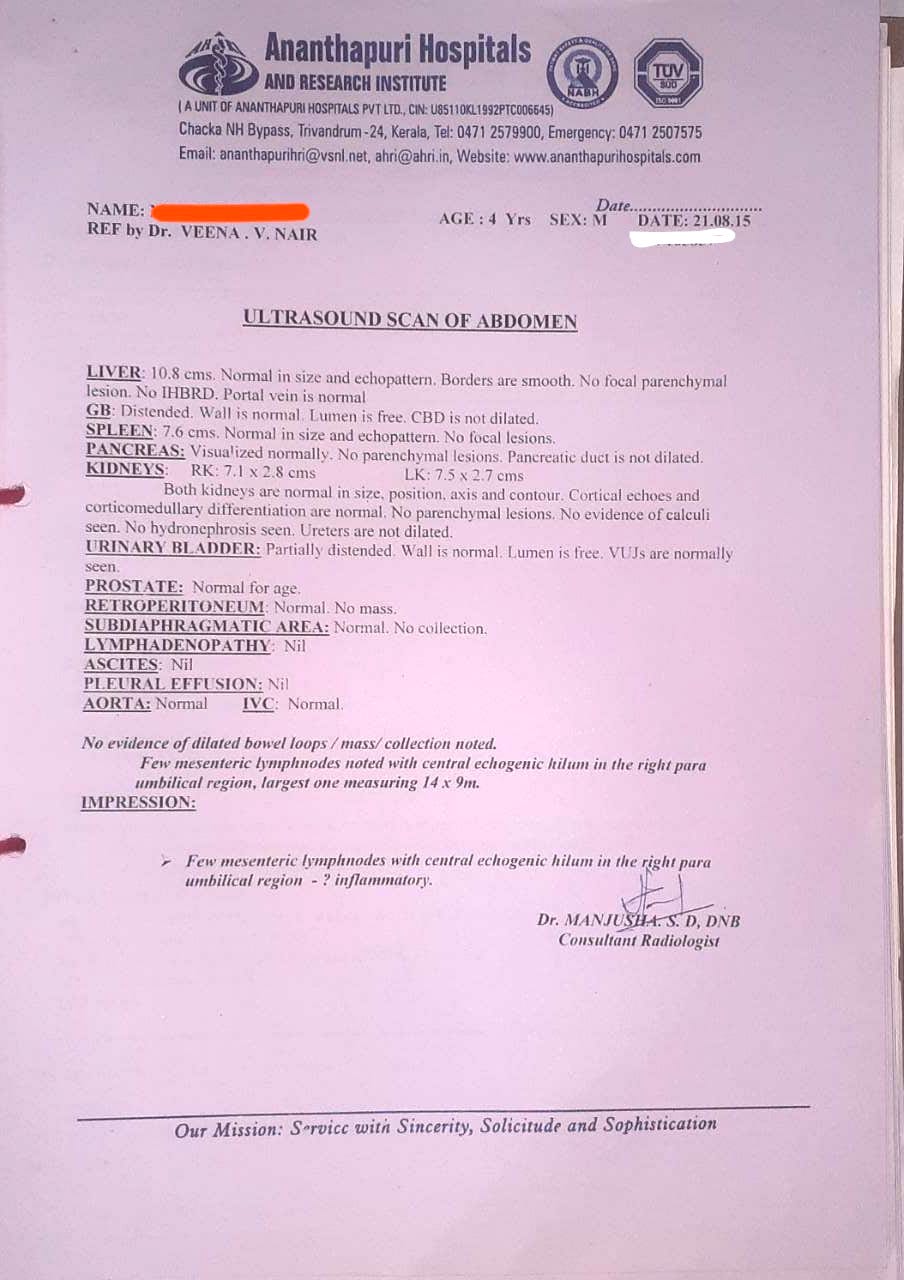
Image 7. Discharge Summary 2016 - Diagnosis Proof documents
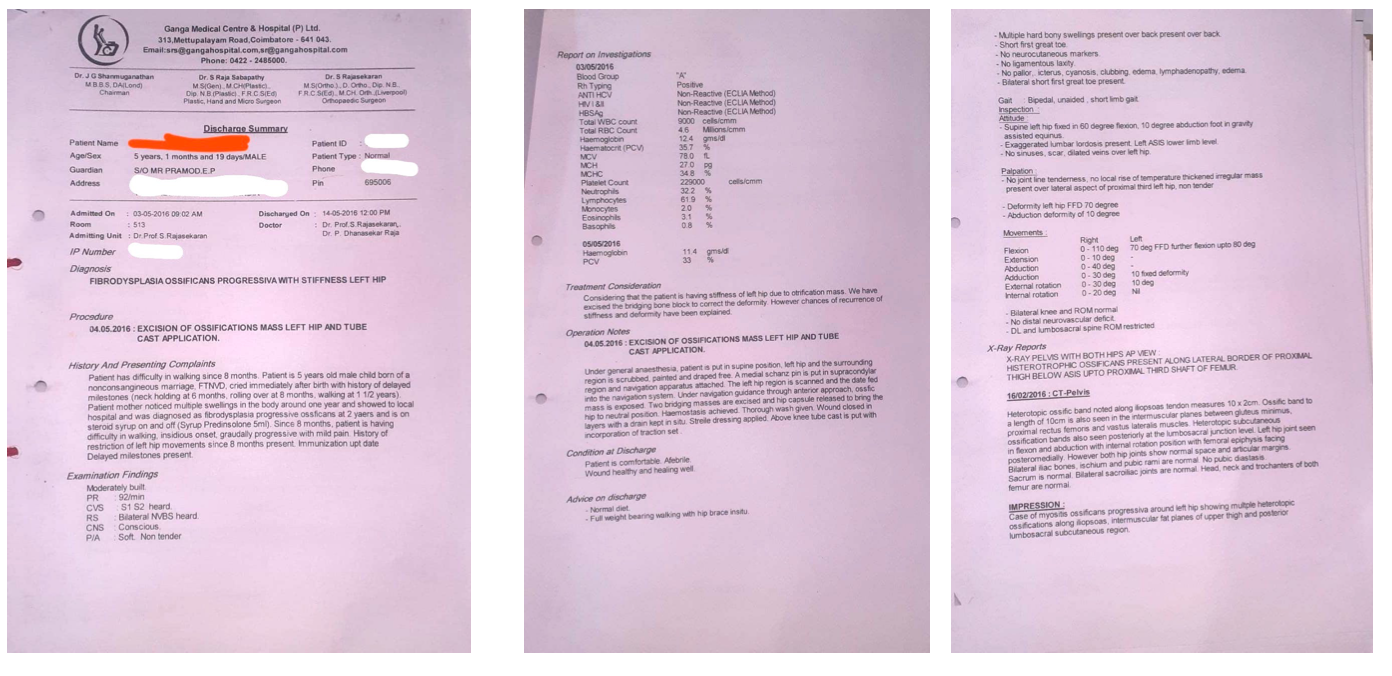 Image 8. Patient image at baseline and endpoint
Image 8. Patient image at baseline and endpoint 
-
Immersive Learning
-
Modern Diagnosis
MODERN DISEASE; Fibrodysplasia Ossificans Progressiva (FOP)
ABOUT THE DISEASE;
Fibrodysplasia ossificans progressiva (FOP) is a clinical condition where, the muscle tissue and connective tissue (such as tendons and ligaments) are gradually replaced by bone, thus causing restricted movement. This can be seen in early childhood itself, where the neck and shoulders are initially affected followed by the other parts of the body and the limbs. They also develop breathing difficulties, eating difficulties etc....that disrupts their normal life.
In this case report, a 11 year old boy, a confirmed case of FOP who has already undergone hip replacement surgery (excision of ossifications) at the age of 5, came seeking Ayurvedic treatment for his condition. His symptoms were managed regularly with conventional medicines. No significant changes were happening.
Diagnostic criteria; The correct diagnosis of FOP can be made clinically even before radiographic evidence of heterotopic ossification is seen, if soft tissues lesions are associated with symmetrical malformations of the great toes. Definitive genetic testing of FOP is now available and can confirm a diagnosis of FOP prior to the appearance of heterotopic ossification. Clinical suspicion of FOP early in life on the basis of malformed great toes can lead to early clinical diagnosis, confirmatory diagnostic genetic testing (if appropriate), and the avoidance of harmful diagnostic and treatment procedures. Clinicians should be aware of the early diagnostic signs of FOP, which are congenital malformation of the great toes and episodic soft tissue swelling even before the appearance of heterotopic ossification. This awareness should prompt genetic consultation and testing (if appropriate) and the institution of assiduous precautions to preventinjuryandiatrogenicharm. Atthepresenttime,genetictestingisavailableona clinical and research basis at several laboratories (Fibrodysplasia Ossificans Progressiva: Diagnosis, Management, and Therapeutic Horizons . Pignolo et al. Pediatr Endocrinol Rev. 2013 June ; 10(0 2): 437–448)
In this patient, gene testing was done to confirm the diagnosis. Medical history was taken in detail with all the documents about the past treatments and test reports.
Image 1. AVCRI Gene Test 2011 attached below
Image 2. Hospital Records collected from the patient revealing the Medical History attached below
Objective parameters; Range of movements for the musculoskeletal joints (Cervical, lumbar, elbow, wrist, shoulder, neck, left hip and left knee) at baseline was recorded.
Image 3. Patient image at baseline attached below
Prognosis: Fibrodysplasia ossificans progressiva (FOP), a rare and disabling genetic condition characterized by congenital malformations of the great toes and progressive heterotopic endochondral ossification (HEO) which is the most catastrophic of HEO disorders in humans. Flare-ups of FOP are episodic; immobility is cumulative. This is a progressive disorder and can only be managed during the episodes. In this patient also, the kid had already undergone hip replacement surgery at the age of 6, and IP admissions for fibrous hamartoma and Myofascitis.
Treatment options; Clinical management of FOP remains symptomatic. The rarity, variable severity and episodic clinical course of FOP pose substantial uncertainties when evaluating experimental therapies . Accordingly, medical intervention is currently supported. To date, there is no proven efficacy of any therapy in altering the natural history of the disease. (Fibrodysplasia Ossificans Progressiva: Diagnosis, Management, and Therapeutic Horizons . Pignolo et al. Pediatr Endocrinol Rev. 2013 June ; 10(0 2): 437–448)
Image 1. AVCRI Gene Test 2011
Image 2. Hospital Records collected from the patient revealing the Medical History
Bone Marrow Test 2012
Paediatric Surgery July and October 2012
Abdomen Ultrasound Scan 2015
Discharge Summary 2016
Patient image at Baseline July 2021
-
Ayurveda Diagnosis
AYURVEDIC DIAGNOSIS: ADHYASTHYASRITA VATA VYADHI
ABOUT THE DISEASE:
The clinical condition called Fibrodysplasia Ossificans Progressiva cannot be directly correlated to a specific disease condition mentioned in the classical textbooks of Ayurveda.
The treating physician has named the disease based on his yukti as Adhyasthyashrita Vatavyadhi. Basically considered as a Vatavyadhi because the disease primarily affects the asthi dhatu that is a vata predominant dha?tu. The symptoms presented by the patient are difficulty in lying down over the back. Patient has complete restricted movements in the neck, right shoulder and right hand and partial restriction of the left hand, back region, left hip and left knee. He also has difficult in removing his shirt or writing etc..., Injury to any part of the body causes swelling which gradually transforms into bone tissue. When he came to consult Dr Raveendran KG, he was 11 years old and had already undergone 2 surgeries and multiple In Patient treatments.
Rationale of treatment: Mainly the line of treatment is that of Dhatugata jvara chikitsa
This is basically a dhatuasrita vyadhi. Here due to the increased formation of asthidhatwagni, dhatu transformation is not taking place properly, by that atipravritti of asthi dhatu is happening and again it is transformed as asthi dhatu only. So the target was to reduce the atipravritti of both Vata and pitta.
Over all Dhatugata jwara chikitsa, vata pitta hara chikitsa, and also asthi dhatu parinama hara chikitsa were the protocols targeted to give relief from the symptoms.
Prognosis; Asadhya sahaja vyadhi.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Gugguluthiktakam Kashayam + Varanadi Kashayam+ Spl Nagaradi Kashayam + Bharangyadi Kashayam + Dhanwantaram (101) + Guduci avarti Kasayam 5ml of Kasayam + 20 ml of warm water+ Dhanwantaram 101 ( 3 drops) + Guduci Avarti (5 drops) Oral, On empty stomach Morning and evening 2021-07-07 - 2021-08-30 Gugguluthiktakam Ks- AH.Ci.21.57-60; Spl Nagaradi- Anubhuta Yoga; Bharngyadi- Sahasra Yogam. Kashaya Prakaranam; Dhanvantaram (101)- Proprietary Medicine; Guduci Avarti- Proprietary Medicine Rasnasapthakam Kashayam + Varanadi Kashayam+ Spl. Nagaradi Kashayam + Shaddharanam gulika + Shanka bhasmam Kasayam 2.5 ml of Kasayam + 10 ml of warm water+ 1/2 Gulika (powdered) + Sankha Bhasmam (50 mg) Oral, At 10 am and 3pm 2021-07-13 - 2021-08-30 Rasnasaptakam- Cakradatta; Varanadi- AH.Su.15.21-22; Shaddharanam gulika- Proprietary Medicine; Shankha Bhasma- Rasatarangini 12.17-18; Rajanyadi churnam + Ashta churnam (1 tsp) Curnam 1 tsp each of the Curnam + 3ml of Honey Oral, Before Lunch and Dinner 2021-07-07 - 2021-08-30 Rajanyadi- AH.Utt.2.38-40; Ashtacurnam- AH.Ci.14.35 Dhanwantararishtam + Nimbamruthasavam Aristam/Asavam 10 ml each Oral, after lunch and dinner 2021-07-07 - 2021-08-30 Dhanvantararishtam- AH; Nimbamrtasavam- AH.Ci. Vatavyadhi.57-61. Shaddharanam gulika Gulika 1/2 Powdered with warm water at bedtime 2021-07-07 - 2021-07-12 Nimabmrutadi castor oil Panam Oil (1/2 teaspoon) + warm milk (25 ml) Oral at bedtime 2021-07-13 - 2021-08-30 AH.Ci.21.58-61 Thamboolarasayanam+ Dasamoolarasayanam+ Mridweekadi Lehyam Lehyam Mixed together, 1 pinch Taken now and then 2021-07-07 - 2021-08-30 Tamboola Rasayanam- Sahasrayogam; Dasamoola Rasayanam- Sahasrayogam; Mridweekadi Lehyam- AH.Ci.3.30 Gugguluthiktakam Kashayam + Dhanvantaram Kashayam+ Spl Nagaradi Kashayam + Bharangyadi Kashayam + Dhanwantaram (101) + Guduci avarti Kasayam 5ml of Ka??yam + 20 ml of warm water+ Dhanwantaram 101 ( 3 drops) + Guduci Avarti (5 drops) Oral, on empty stomach morning and evening 2021-08-31 - 2021-10-30 Rasnasapthakam Kashayam + Varanadi Kashayam+ Spl. Nagaradi Kashayam + Shaddharanam Gulika + Shanka bhasmam Kasayam 5 ml of Kasayam + 10 ml of warm water+ 1/2 Gulika (powdered) + Sankha Bhasmam (50 mg) Oral, On empty stomach, Evening 2021-08-31 - 2021-10-30 Rajanyadi churnam + Ashta churnam (1 tsp) Curnam 1 tsp each of the Curnam + 3 ml of Honey Oral, 2021-08-31 - 2021-10-30 Nimabmrutadi Castor Oil Panam 1/2 tsp of Castor oil + 25 ml of warm milk Oral at bedtime 2021-08-31 - 2021-10-30 Thamboola rasayanam+ Dasamoola rasayanam+ Mridweekadil ehyam Rasayanam Mixed together, 1 pinch Oral, now and then 2021-08-31 - 2021-10-30 Durvadi Tailam + Eladi Co. Oil Tailam Required quantity Abhyangam on head, in the morning 2021-07-07 - 2021-07-12 Durvadi Tailam- Sahasra Yogam. Taila Prakaranam; Eladi Co Oil- Sahasra Yogam. Taila Prakaranam Prabhanjana vimardanamthailam + Narayana Tailam + Pinda Tailam + Chinchadi Tailam Tailam Required quantity Abhyangam on body in the moprning 2021-07-07 - 2021-07-12 Prabhanjanavimardana Tailam- Sahasra yogam. Taila Prakaranam; Narayana Tailam- Bhaishajya Ratnavali. Vatavyadhi. Kadi Dhara Drava Required quantity Dhara on the whole body 2021-07-13 - 2021-08-02 Anubhuta Yogam Indukantha Ghrtam Ghrtam 1 tsp Oral, after dinner 2021-07-26 - 2021-08-02 Sahasra yogam. Ghrta Prakaranam Erandamuladi Kasaya Vasti Vasti Dravya 900 ml Rectal, on empty stomach 2021-08-03 - 2021-08-07 Ca.Si.3 Special Kizhi Kizhi 2- 4 Kizhi External application on the bony projections, shoulder, knee and hip joint. 2021-08-08 - 2021-08-30 Anubhuta Yogam Gajalekshmi Lepanam Lepa Required quantity External application on the bony projections, shoulder, knee and hip joint. 2021-07-08 - 2021-08-29 Anubhuta Yogam -
Outcome Measures
OUTCOME MEASURES;
11-year-old child, born of a non-consanguineous marriage, Full Term Normal Vaginal Delivery cried immediately after birth with a history of delayed milestones (neck holding at 6 months, rollover at 8 months, walking at 1 1/2 year) , a confirmed case of Fibrodysplasia ossificans progressive, sought treatment from Dr K G Raveendran. He had already undergone hip replacement surgery to remove the ossification mass at the age of 5. His presenting complaints were difficulty in lying down over the back. Complete restricted movements of the neck, right shoulder and right hand and partial restriction of the left hand, back region, left hip and left knee. Difficult for him to remove his shirt or writing etc..., Injury to any part of the body causes swelling which gradually transforms to bone tissue. After intense Ayurvedic IP treatments for 1 and half months, there were improvements in the range of movements in the lumbar, shoulder, cervical joints and right leg. The prominent bony projections in the back appeared to have reduced in size.
As this is a congenital disorder, with no known cure and is a progressive condition, regular Ayurvedic management is advised to maintain the quality of life.Only subjective assessments were done, as in FOP objective parameters are not significant.
Subjective parameters; Range of movements in major affected joints was assessed at baseline and at the endpoint to measure the outcome. They were tabulated as follows:
MUSCULO SKELETAL SYSTEM
During admission
During discharge
Anteverted bent spine
Anteverted bent spine – Slightly improved
Gait – Limping
Gait – Limping
Multiple hard bony projection all over the back, shoulders, left hip and left knee
Multiple hard bony projection all over the back, shoulders, left hip and left knee – size reduced comparatively
Length variation of B/L leg
Length variation of B/L leg
CERVICAL JOINT
During admission
During discharge
Multiple bone projection
Multiple bone projection reduction in size
Tenderness – Absent
Tenderness – Absent
ROM
ROM
Flexion - <=5 degree
Flexion - <=5 degree
Extension - <=5 degree
Extension - <=5 degree
Right rotation - <=5 degree
Right rotation - <=10 degree
Left rotation - <=5 degree
Left rotation - <=5 degree
Right lateral bending - <=5 degree
Right lateral bending - <=5 degree
Left lateral bending - <=5 degree
Left lateral bending - <=5 degree
LUMBAR JOINT
During admission
During discharge
Multiple bone projection
Multiple bone projection reduction in size
Tenderness – Absent
Tenderness – Absent
ROM
ROM
SLR –
Movements are better in right leg than left leg.SLR –
Movements are better in right leg than left leg.Right leg - > 45 degree
Right leg - >50 degree
Left leg - < 25 degree
Left leg - < 25 degree
LEFT HIP JOINT
During admission
During discharge
Tenderness- Absent
Tenderness- Absent
Movements - Restricted
Movements - Restricted
Swelling- Absent
Swelling- Absent
LEFT KNEE JOINT
During admission
During discharge
Tenderness- Absent
Tenderness- Absent
Crepitus- Absent
Crepitus- Absent
Swelling- Absent
Swelling- Absent
Movements - Restricted
Movements - Restricted
SHOULDER JOINT
During admission
During discharge
Right shoulder joint
Right shoulder joint
Tenderness – Absent
Tenderness – Absent
ROM
ROM
Abduction - <=5 degree
Abduction - <=10 degree
Adduction - <=5 degree
Adduction - <=10 degree
Flexion - <=5 degree
Flexion - <=10 degree
Extension - <=5 degree
Extension - <=10 degree
Left shoulder joint
Left shoulder joint
Tenderness – Absent
Tenderness – Absent
ROM
ROM
Abduction 30 degree
Abduction 30 degree
Flexion 70 degree
Flexion 70 degree
Extension - <= 10 degree
Extension - <= 10 degree
ELBOW JOINT
During admission
During discharge
No Tenderness
No Tenderness
Flexion and extension almost full
Flexion and extension almost full
WRIST JOINT
During admission
During discharge
ROM – All movements are full without restriction
ROM – All movements are full without restriction
Image 1. Images were taken at baseline, midpoint and endpoint, attached below
DISEASE MODIFYING EFFECT; He got improvements in the Range of movements in some joints, along with a reduction in bony projections after a 1 month IP treatment. He is advised to continue the medicines along with diet and lifestyle management, and come for regular follow ups.
Image 1. Patient images taken before, during and after Ayurvedic Treatment
-