Featured Case
-
Abstract
A 47-year-old female with severe abdominal pain was diagnosed with acute calculus cholecystitis. The diagnosis was confirmed by a USG abdomen, which detected multiple gallstones of varying size, and she did not respond to standard of care with the persisting symptoms. She opted for ayurvedic treatment. The patient presented with acute abdominal pain, specifically in the right upper and middle quadrants, associated with itching all over the body for three days. Murphy’s sign was positive on clinical examination. Dr Jyoti Joshi diagnosed this condition as Pittashmari, and the treatment focused on the correction of Jataragni. After 2 days of treatment, the abdominal pain and itching subsided. In the repeat USG done after 4 months of treatment, the gall bladder appeared normal without any calculi. This case reports the outcomes and potential of Ayurveda treatment in acute calculus cholecystitis.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
Standalone Ayurvedic management of Acute calculus cholecystitis
A 47-year-old female with severe abdominal pain was diagnosed with acute calculus cholecystitis. The diagnosis was confirmed by a USG abdomen, which detected multiple gallstones of varying size, and she did not respond to standard of care with the persisting symptoms. She opted for ayurvedic treatment. The patient presented with acute abdominal pain, specifically in the right upper and middle quadrants, associated with itching all over the body for three days. Murphy’s sign was positive on clinical examination. Dr Jyoti Joshi diagnosed this condition as Pittashmari, and the treatment focused on the correction of Jataragni. After 2 days of treatment, the abdominal pain and itching subsided. In the repeat USG done after 4 months of treatment, the gall bladder appeared normal without any calculi. This case reports the outcomes and potential of Ayurveda treatment in acute calculus cholecystitis.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Standalone Ayurvedic management of Acute calculus cholecystitis- A Case report
Dr Jyoti Joshi
ABSTRACT
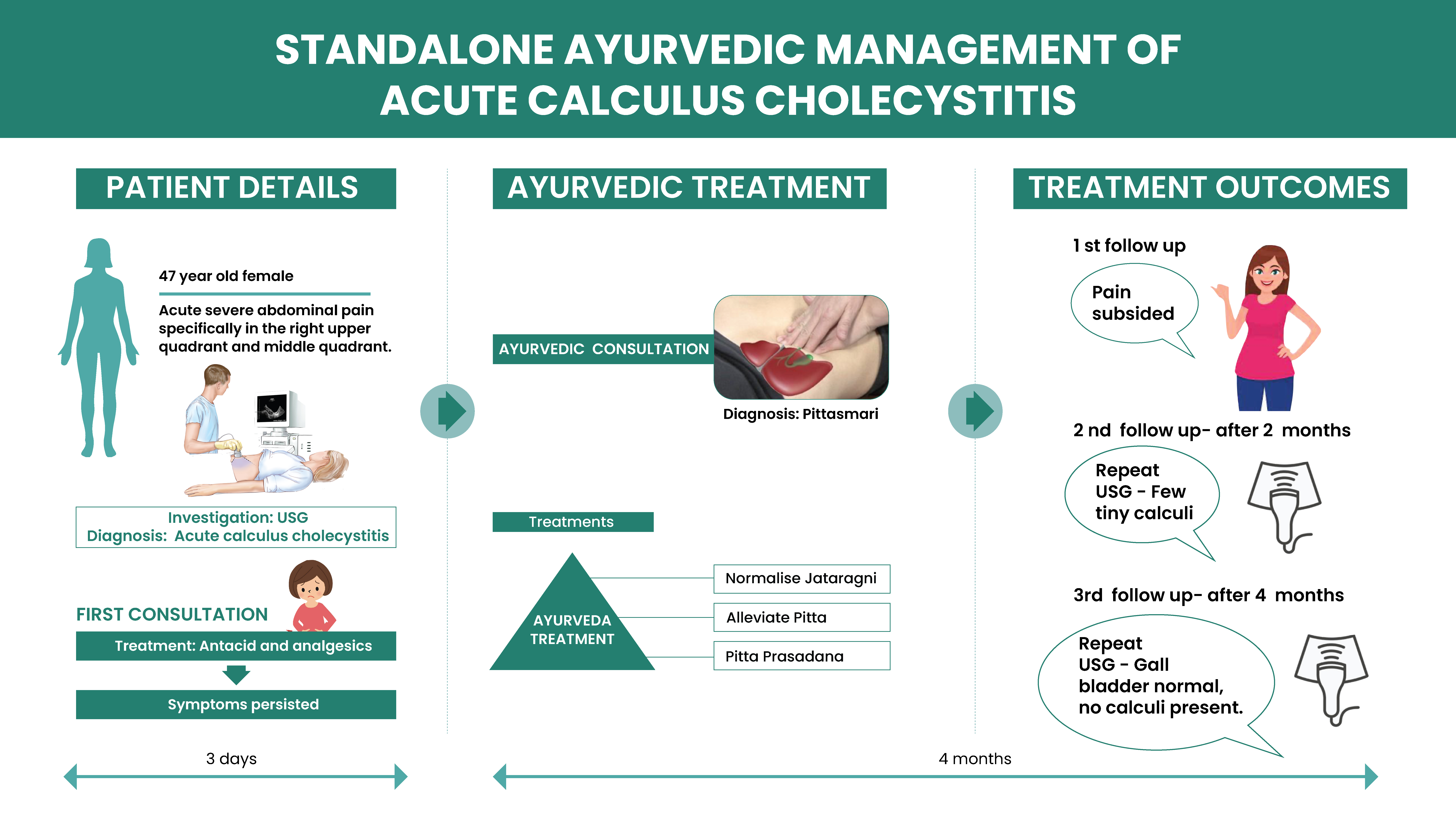
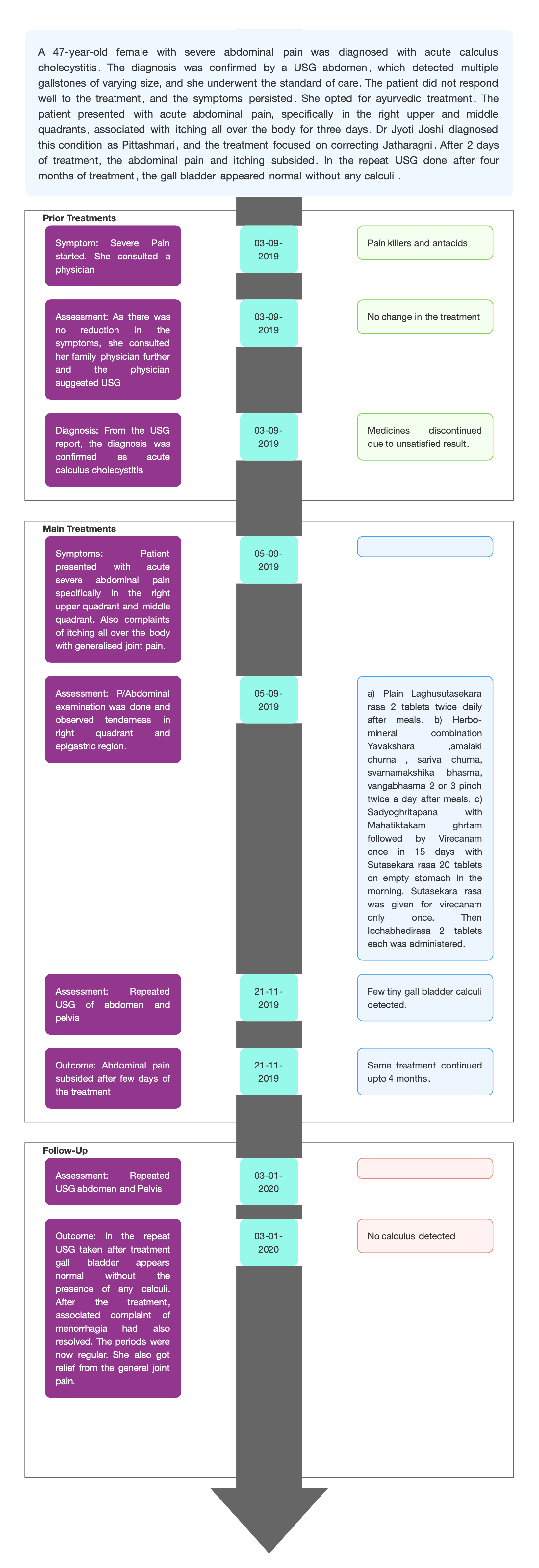
A 47-year-old female with severe abdominal pain was diagnosed with acute calculus cholecystitis. The diagnosis was confirmed by a USG abdomen, which detected multiple gallstones of varying size and she underwent the standard of care. The patient did not respond well to the treatment, and the symptoms persist. She opted for ayurvedic treatment. The patient presented with acute abdominal pain, specifically in the right upper and middle quadrants, associated with itching all over the body for three days. Murphy’s sign was positive on clinical examination. Dr Jyoti Joshi diagnosed this condition as Pittashmari and the treatment focused on the correction of Jatharagni. After 2 days of treatment, the abdominal pain and itching subsided. In the repeat USG done after four months of treatment, the gall bladder appeared normal without any calculi. Thus, Ayurveda can opt as a treatment of choice in acute calculus cholecystitis.
KEYWORDS
Acute cholecystitis, pittasmari, case report
INTRODUCTION
Acute cholecystitis—inflammation of the gall bladder— is most often caused by gallstones. Gallstones are one of the most common gastrointestinal tract disorders, affecting about 10% of people in Western society. More than 80% of people with gallstones are asymptomatic. Acute cholecystitis develops in 1-3% of patients with symptomatic gallstones [1]. Gallbladder disease occurs in men and women, with certain populations being more prone to it. The risk of gallbladder disease increases in women, obese patients, pregnant women, and patients in their 40s.
PATIENT INFORMATION
47 yr old female patient presented with acute severe abdominal pain specifically in the right upper quadrant and middle quadrant associated with itching all over the body for three days.
Medical history: Patient developed severe abdominal pain before 3 days. As the pain was unbearable, she consulted a general practitioner who prescribed painkillers and antacids. She took one course of painkillers to get relief from symptoms. Then she contacted her family physician for further opinion. On the basis of the presenting symptoms, the physician suggested USG and the diagnosis was confirmed as acute calculus cholecystitis and advised surgical management. But the patient was not willing to go for surgery, so came for Ayurvedic treatment.
CLINICAL FINDINGS
P/A examination: tenderness in the right quadrant and epigastric region.
TIMELINE
Image 1 : Attached
DIAGNOSTIC ASSESSMENT
Modern diagnosis: The patient presented with acute severe abdominal pain specifically in the right upper quadrant and middle quadrant. Based on clinical examination and USG report taken the condition was diagnosed as Acute calculus cholecystitis.
Image 2: Proof document attached
Ayurvedic diagnosis: pittasmari
Differential diagnosis: Appendicitis, Biliary colic, Cholangitis, Mesenteric ischemia, Gastritis,
Peptic ulcer disease.
Prognosis: For patients with uncomplicated acute cholecystitis, the prognosis is excellent. The mortality rates are very low. Perforation or gangrene of the gallbladder may occur in delayed cases. Patients with acalculous cholecystitis have high mortality varying from 20-50%. In this case, Patient presented with cholelithiasis, for which surgical management was suggested by the consulted doctor. But the patient was not willing to do surgery, hence she opted for Ayurvedic medicines to get cured. With Ayurvedic medicines, she got symptomatic relief and also a repeat USG did not detect any gallstones.
THERAPEUTIC INTERVENTION
See Tab Treatment details
Follow-up and outcome
1st Follow up (21/11/2019): revealed presence of few tiny gall bladder calculi.
2nd Follow up (3/1/2020): gall bladder appears normal without the presence of any calculi.
Clinician-based assessment: After few days of treatment abdominal pain subsided. USG taken during the treatment (nov 2019) revealed presence of few tiny gall bladder calculi. In the repeated USG taken after treatment gall bladder appears normal without the presence of any calculi. She also got relief from general joint pain.
Image : 3 attached
Patient assessed: Not relevant
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported
DISCUSSION
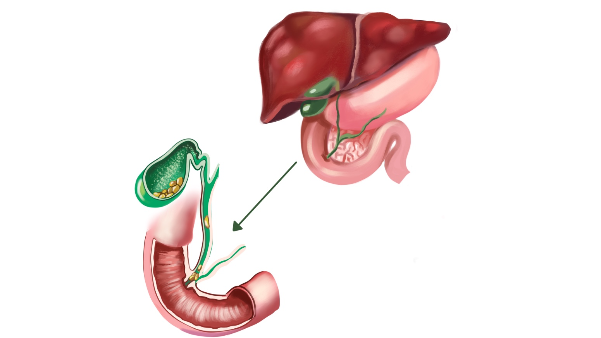
Cholelithiasis is correlated to the term Pittasmari according to the Ayurveda concept.The Pitta and Kapha produced in excess by their specific Naidanika factors combine with each other and localized in the urinary system and get precipitate specially at bladder neck and obstruct the bladder outlet. It results in obstruction of urine flow and symptoms of Pittaja Ashmari as,burning hot sensation and inflammatory changes in urinary tract. The Ashmari is reddish, yellowish, black or honey like in colour and appear like Bhallataka seed [2]
The most appropriate management of cholecystitis is laparoscopic cholecystectomy. There are low morbidity and mortality rates with quick recovery. This can also be done with an open technique in cases where the patient is not a good laparoscopic candidate. In situations in which the patient is acutely ill and considered a poor surgical candidate, he or she may be treated with temporizing percutaneous drainage of the gallbladder. Milder cases of chronic cholecystitis in patients considered poor surgical candidates might be managed with low-fat and low-spice diets. The results of this treatment vary. Medical treatment of gallstones with ursodiol also has been reported to have occasional success.
As the condition is pitt??mari, the correction of ja?har?gni is very important. K??ra and virecana was adopted for alleviating the pitta. Pitta is in pakv?vastha. With virecana karma, pittanirharana can be done. Instead of systematic Virechana, virechana was done once in 15days to avoid obstructive cholecystitis. Drugs like ?at?vari are all pittapras?danam in nature.
PATIENT’S PERSPECTIVE
Not obtained
LEARNING POINTS
The clinical condition is completely surgically curable, according to conventional medicine. A surgically curable condition was otherwise successfully managed with only oral medications that helped avoid hospitalisation, post-surgical difficulties, simultaneously giving symptomatic relief from long standing associated complaints.
INFORMED CONSENT
Written informed consent was given by the patient for publication.
CONFLICT OF INTEREST
None declared
FUNDING
None
REFERENCE:
1.Indar, A. A., & Beckingham, I. J. (2002). Acute cholecystitis. BMJ (Clinical research ed.), 325(7365), 639–643. https://doi.org/10.1136/bmj.325.7365.639
2. Acharya Priyavrat Sharma(ed), Sushruta Samhita with Dalhana virachita Nibandha Sangraha vyakhya, published by Chaukhamba samskrita Samsthana, Varanasi, 8th edition 2005, Nidana Sthana 3 /9
-
Immersive Learning
-
Modern Diagnosis
Modern Diagnosis: Acute calculus cholecystitis
About the Disease: Acute calculus cholecystitis is the inflammation of gall bladder that occurs due to occlusion of the cystic duct or impaired emptying of the gallbladder. The finding of right upper abdominal pain with deep palpation, Murphy sign, is usually classic for this disease.
About 20% of patients with acute cholecystitis need emergency surgery and the prognosis is good in uncomplicated cases. In severe cases of acute cholecystitis, the intense inflammation can make surgery difficult, resulting in injury to the bile duct, which has substantial morbidity
Diagnostic Criteria:
A. Local signs of inflammation etc.:
(1) Murphy’s sign, (2) RUQ mass/pain/tenderness
B. Systemic signs of inflammation etc.:
(1) Fever, (2) elevated CRP, (3) elevated WBC count
C. Imaging findings: imaging findings characteristic of acute cholecystitis
Definite diagnosis
(1) One item in A and one item in B are positive
(2) C confirms the diagnosis when acute cholecystitis is suspected clinically
Confirmed Diagnosis: Diagnosis was made based on medical signs and reported symptoms, along with USG done as instructed by a previously consulted physician.
Baseline evaluation: USG Abdomen & pelvis (3/9/2019) - Acute calculus cholecystitis and Bulky uterus.
Image 1: USG report done before treatment
Prognosis:
The patient presented with acute calculus cholecystitis. In patient's words, she was suggested to undergo surgical management but was unwilling to do surgery and opted for Ayurvedic treatment. After 2 days of treatment, the abdominal pain subsided. In the repeat USG done after treatment, the gall bladder appeared normal without any calculi.
Treatment:
Immediate measures should be taken to rest the gall bladder; this will subdue the inflammatory process in most patients. Patients should be fasted, rehydrated with intravenous fluids, and given oxygen therapy and adequate analgesia. Indometacin (25 mg three times daily for a week) can reverse the inflammation of the gall bladder and the contractile dysfunction seen in the early stages (first 24 hours) of cholecystitis. The prokinetic action of indometacin will also improve postprandial emptying of the gall bladder in patients with gallbladder disease. A single intramuscular dose of diclofenac (75 mg) may substantially decrease the rate of progression to acute cholecystitis in patients with symptomatic gallstones. Because of the risk of superimposed infection, intravenous antibiotics should be started empirically if the patient has systemic signs or if no improvement is seen after 12-24 hours. A second-generation or newer cephalosporin should be used (for example, cefuroxime 1.5 g every 6-8 hours) with metronidazole (500 mg every 8 hours). Non-operative management—solvent dissolution therapy or extracorporeal shockwave lithotripsy—has been used with variable results to treat chronic cholecystitis in patients unfit for surgery, but it has no place in the management of acute cholecystitis.
-
Ayurveda Diagnosis
Ayurveda diagnosis: Pittasmari
Pittashmari refers to gallstones or biliary calculi. Pitta refers to bile, tissue metabolism, and body heat in Sanskrit. Pitta is regarded as a vikriti or byproduct of rakta in Ayurvedic literature. The word "Ashmari" translates to "stone" or "calculus."
Samprapti:
While considering the pathogenesis of gallstone in Ayurvedic parlance, it can be said that the kaphaprakopaka Nidanasevan (causative factors) leads to accumulation of Kapha at first, which produces the symptoms like Alasya (lethargy), Gaurav (heaviness), Mandoshmata (decreased digestive fire). In Pittashaya (gall bladder) quantitatively accumulated Kapha mixes with the Pitta already present in it. The mixture of Kapha and Pitta in Pittashaya leads to the formation of viscous material (biliary sludge) causing obstruction in the passage of Vayu. Hence the Vayu gets vitiated by its Rukshadi gunas and converts the viscous material into a dry and solid form called Pittashmari (gallstone).
In this patient, frequent consumption of fast foods and junk foods can be considered the cause of pittasmari. On account of a long-term habit of irregular lifestyle, leading to vikriti of pitta resulting in pittasmari.
Treatment target:
As the condition is pittashmari, the correction of jataragnii is significant. Kshara and virecana were adopted for alleviating the pitta. Pitta is in pakvavastha. With virecana karma, pittanirharana can be done. Instead of systematic Virechana karma, a virechana was done once in 15 days to avoid obstructive cholecystitis. Drugs like satavari are all pittaprasadanam in nature.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Plain Laghusutasekhara rasa Tablet 1-0-1 Oral, after meals 2019-09-06 - 2020-01-03 Rasa Tarangini - Parisishta Herbo-mineral combination [Yavaksara (125mg), amalaki curna (5gm), sariva curna (5gm), svarnamaksika bhasma (1gm), vangabhasma (1gm)] Powder 2- 3 pinch twice a day After meals. 2019-09-06 - 2020-01-03 Anubuta Yoga Virechanam Virechanam Sadyoghrtap?na with Mahatiktakagh?tam (30ml) followed by Virecanam once in 15 days with S Oral 2019-09-06 - 2020-01-03 Mahatiktakaghrtam - Bhaishajyaratnavali Kushta Adhikara 118 – 124 Sutasekhara rasa - Yogaratnakara Amlapitta Chikitsa 705 Icchabhedirasa Tablet 1-0-1 After meals 2019-09-06 - 2020-01-03 Bhaishajya Ratnavali Udara Rogadhikara 13 – 105 -
Outcome Measures
OUTCOME:
A 47 year old female presented with acute severe abdominal pain, specifically in the right upper and middle quadrant, associated with itching all over the body for three days. As the previously consulted physician advised, USG was done, and the case was diagnosed as Acute Calculus Cholecystitis. The Allopathic doctor suggested surgical management, but the patient was unwilling to do surgery and adopted ayurvedic treatment to get cured. After a few days of treatment, abdominal pain subsided. USG one during the treatment revealed the presence of a few small gall bladder calculi. In the repeated USG done after treatment gall bladder appears normal without any calculi. After the treatment, the associated complaint of menorrhagia had also resolved. The periods were now regular. She also got relief from the general joint pain.
Subjective assessment: Abdominal pain subsided within 2- 3 days of treatment.
Objective assessment: USG report
Baseline evaluation (3/9/2019)
Detected multiple gall stones, largest among them measuring 3-4mm size
Midpoint evaluation (21/11/2019)
revealed presence of few tiny gall bladder calculi.
Endpoint evaluation (3/1/2020)
gall bladder appears normal without the presence of any calculi.
Image 1: Baseline evaluation 3.9.2019
Image 2: Midpoint evaluation 21.11.2019
Image 3: Endpoint evaluation 3.1.2020
-