Featured Case
-
Abstract
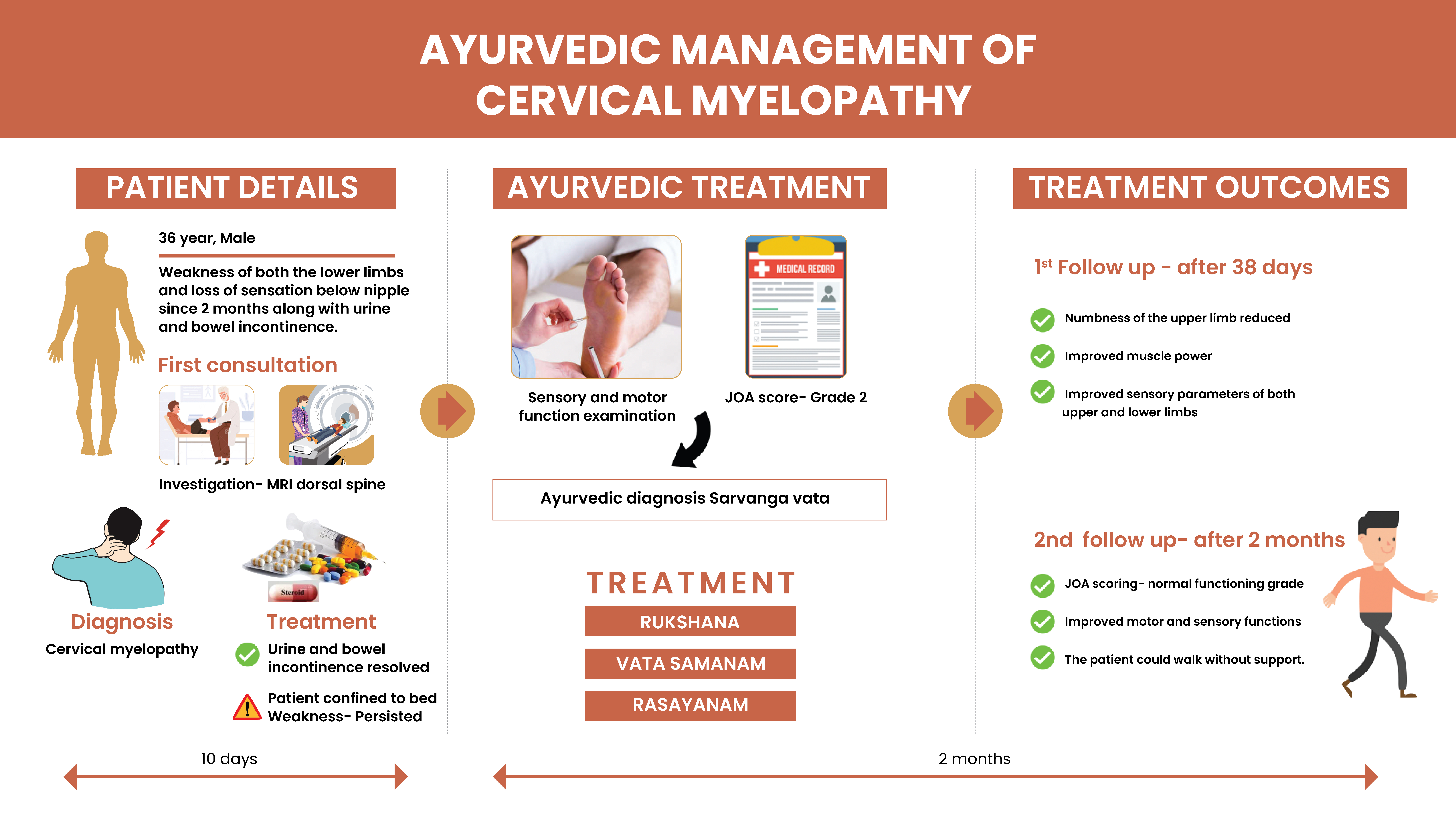
A 36-year-old diabetic male patient was diagnosed with cervical myelopathy. The diagnosis was confirmed by an MRI dorsal spine which revealed symmetric T2 hyperintensity in the long segment of the spinal cord. He was confined to bed during the course of treatment. The patient was administered steroids and other undisclosed supportive medications for 2 months. Urine and bowel incontinence was present during the initial period which resolved with the standard care treatments. The symptoms such as the weakness and loss of sensation in both lower limbs associated with weakness and occasional numbness of upper limbs persisted. The patient opted Ayurvedic treatment for further management and approached Dr Mukesh. The Japanese Orthopedic Association scoring was Grade 2, revealing reduced sensory and motor functions. The physician diagnosed this clinical condition as Sarvanga vata. Rukshana therapy was administered followed by Vata Samana and Rasayana therapy. At the time of discharge, after 38 days of treatment, numbness of the upper limb reduced with improved muscle power and other sensory parameters of both upper and lower limbs. In the follow-up, after 2 months the Japanese Orthopedic Association scoring indicated a normal functioning grade. The patient is now able to walk without any support. This case report demonstrates the scope of Ayurvedic treatment in disabling cervical myelopathy.
-
Summaries
-
Listen
-
Watch
-
View
-
Read

Ayurvedic management of cervical myelopathy- A case report
A 36-year-old diabetic male patient was diagnosed with cervical myelopathy. The diagnosis was confirmed by an MRI dorsal spine which revealed symmetric T2 hyperintensity in the long segment of the spinal cord. He was confined to bed during the course of treatment. The patient was administered steroids and other undisclosed supportive medications for 2 months. Urine and bowel incontinence was present during the initial period which resolved with the standard care treatments. The symptoms such as the weakness and loss of sensation in both lower limbs associated with weakness and occasional numbness of upper limbs persisted. The patient opted Ayurvedic treatment for further management and approached Dr Mukesh. The Japanese Orthopedic Association scoring was Grade 2, revealing reduced sensory and motor functions. The physician diagnosed this clinical condition as Sarvanga vata. Rukshana therapy was administered followed by Vata Samana and Rasayana therapy. At the time of discharge, after 38 days of treatment, numbness of the upper limb reduced with improved muscle power and other sensory parameters of both upper and lower limbs. In the follow-up, after 2 months the Japanese Orthopedic Association scoring indicated a normal functioning grade. The patient is now able to walk without any support. This case report demonstrates the scope of Ayurvedic treatment in disabling cervical myelopathy.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE:
Ayurvedic management of cervical myelopathy- A case report
Dr Mukesh. E
ABSTRACT
A 36-year-old male patient was diagnosed with cervical myelopathy. The diagnosis was confirmed by MRI dorsal spine which shows symmetric T2 hyperintensity in the long segment of the spinal cord. He was confined to bed during treatment. The patient underwent steroids and other undisclosed supportive medications for 2 months. Urine and bowel incontinence was present during the initial period and resolved with the standard care treatments. Whereas the symptoms like weakness and loss of sensation in both lower limbs associated with weakness and occasional numbness of upper limbs persisted. The patient opted for Ayurvedic treatment for further management and approached Dr Mukesh. Based on clinical examination and assessment done, the Japanese Orthopedic Association scoring was Grade 2 which revealed reduced sensory and motor functions. The physician diagnosed this clinical condition as Sarvanga vata. Rukshana therapy was administered followed by Vata Samana and Rasayana therapy. At the time of discharge, after 38 days of treatment, numbness of the upper limb reduced with improved muscle power and other sensory parameters of both upper and lower limbs. In the follow-up, after 2 months the Japanese Orthopedic Association scoring indicated a normal functioning grade. The patient is able to walk without support
KEYWORDS
Cervical myelopathy, case report, myelopathy, sarvanga vata, Ayurveda
INTRODUCTION
Cervical myelopathy refers to compression of the cervical spinal cord. Any space-occupying lesion within the cervical spine with the potential to compress the spinal cord can cause cervical myelopathy. it has an insidious onset progressing in a stepwise manner with functional decline. Cervical myelopathy is the most common type of myelopathy in adults above 55 years of age. Etiologies include degenerative changes of the spine, spinal trauma, infection, tumors, and autoimmune disorders. Treatment includes conservative management for degenerative disease or immediate surgical decompression in acute compression.
PATIENT INFORMATION
36year old diabetic male patient presented with weakness and loss of sensation of the lower limbs associated with weakness and occasional numbness of the upper limbs.
Medical history: The patient working abroad developed weakness of both the lower limbs and loss of sensation below the nipple along with urine and bowel incontinence. After returning from abroad, he consulted a neurologist. MRI dorsal spine shows symmetric T2 hyperintensity in long segments of the spinal cord.? Subacute combined degeneration in the spinal cord. He was treated with steroids and other medications. Urinary and bowel incontinence were corrected. For further management, the patient opted Ayurveda treatment.
CLINICAL FINDINGS
Nervous system :
Higher mental functions - alert, oriented, conscious
Cranial nerves- Intact
Finger-nose touch- intact
Heel shin test- impaired
Tandem walking- Not possible
Sensory system: Light touch impaired on both lower limb
Deep touch impaired on both lower limbs
Pain - impaired on both lower limbs
Temperature- hot impaired on rt lower limb
Vibration- impaired on both lower limb
Stereognosis- Intact
Reflexes:
Supinator- present B/L, Biceps- present B/L, Triceps- present B/L, Knee+, Ankle +
Motor system: UL- grade3 b/l, LL- grade1 b/l
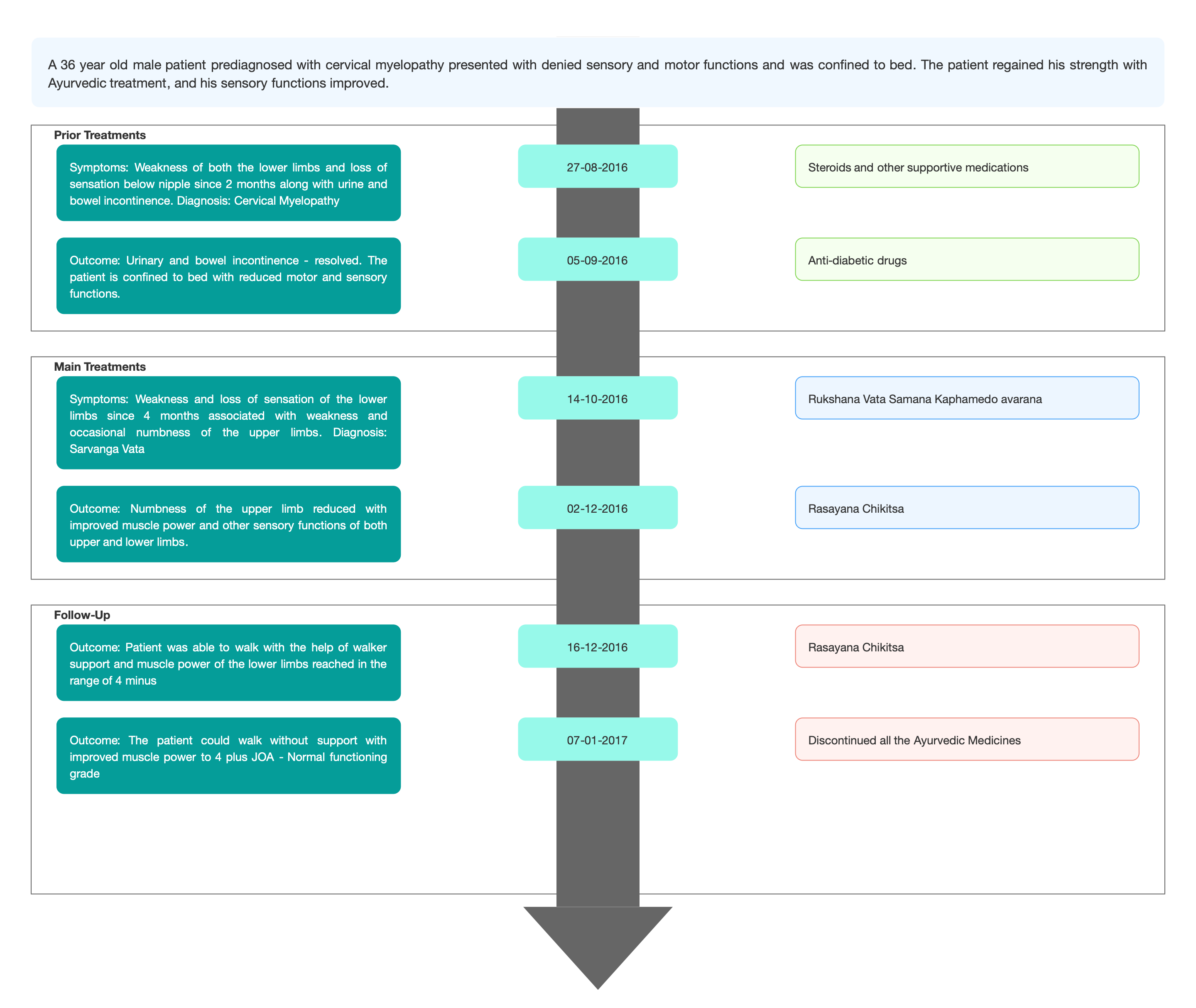
TIMELINE
Image 1. Attached below
DIAGNOSTIC ASSESSMENT
Modern Diagnosis: The condition was prediagnosed as a case of cervical myelopathy by the consulted Neurologist.
Ayurvedic Diagnosis: Based on previous treatment records and clinical examinations, the physician confirmed the diagnosis, and the case were treated as sarvanga vata.
Image 2. Diagnosis proof: Previous hospital records
Differential Diagnosis:
Central Chord syndrome
Chiari malformation
Guillain-Barre syndrome
Multiple Sclerosis Syrinx.
This was ruled out by the treating physician based on clinical examination and special investigations.
Prognosis: Without treatment, patients may progress toward significant paralysis and loss of function. MRI findings showing High-intensity changes in T2 predict a poorer recovery rate, and worse motor symptom improvements. In this, the case was pre-diagnosed as cervical myelopathy, and the MRI reports show high-intensity changes on T2. The patient was confined to bed during the initial stage of treatment with reduced motor and sensory functions. With Ayurvedic treatment, the motor and sensory functions improved, and in further follow-ups, the patient was able to walk without any support.
THERAPEUTIC INTERVENTION
See the Tab 'Treatment details'
FOLLOW-UP AND OUTCOMES
First, follow up after 2 weeks of discharge: the patient was able to walk with help of walker support—muscle power of lower limbs in the range of 4 minuses.
Second, follow up after one month after the first follow-up: the patient was able to walk without support. The muscle power of lower limbs is 4 +.
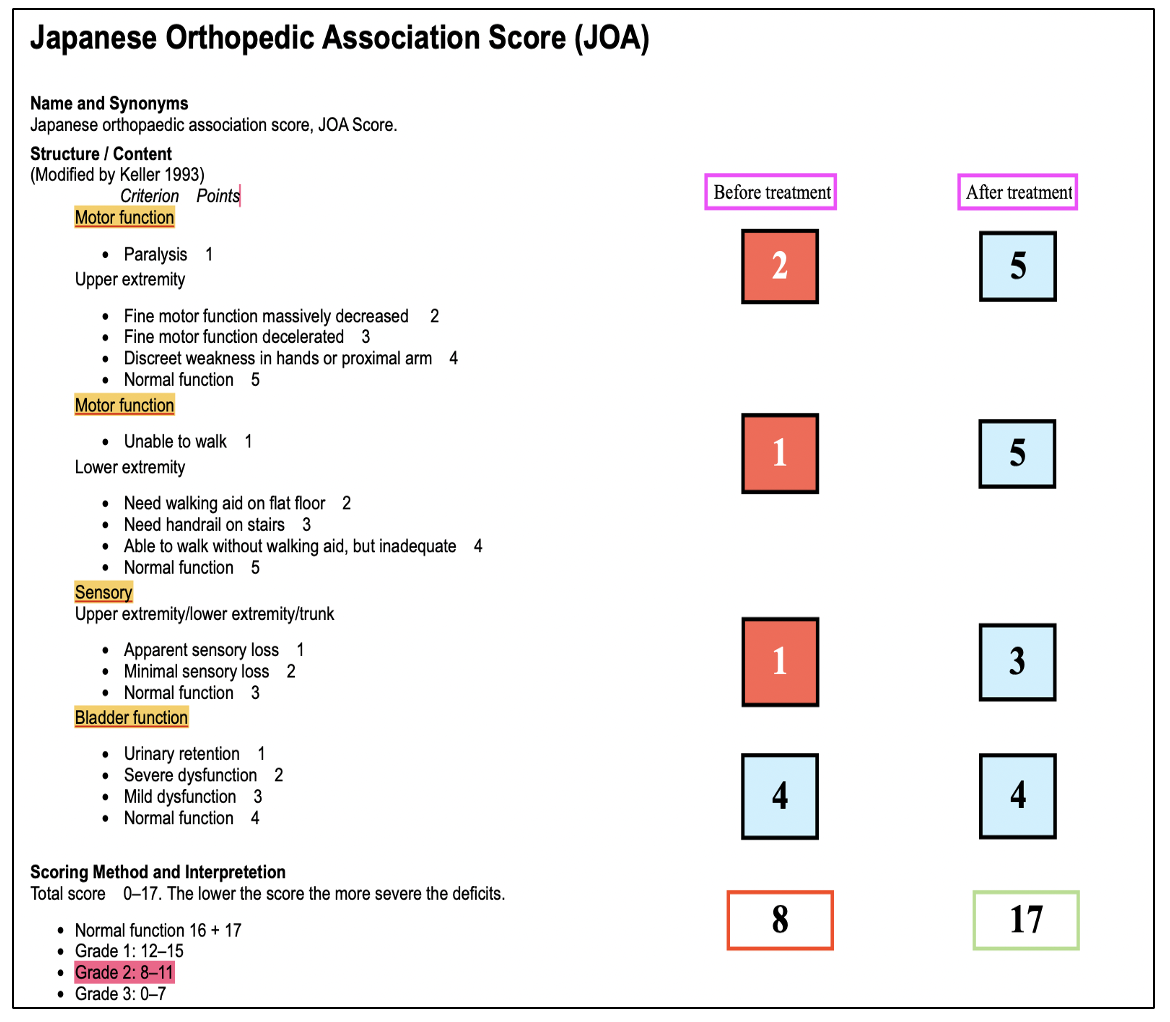
Clinician-based assessment: During the initial period of treatment, the Japanese Orthopedic Association scoring was Grade 2, which revealed reduced sensory and motor functions. In the follow-up, after 2 months, the Japanese Orthopedic Association scoring indicated a normal functioning grade. The patient can walk without support.
Image 3. Japanese Orthopedic Association scoring- before and after treatment
Patient assessment: Not relevant
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported
DISCUSSION
Due to the intake of various diets and regimens, Vata dosha gets vitiated and occupies rakta strotas in the body. Then ultimately, it causes Vata vyadhi like sarvanga vata. Ruksha guna of Vata causes rukshata and parushta in the strotas, which is the key point in the samprapti of sarvanga vata. In this patient, Santarpana janya bahudoshavastha leads to prameha. Kapahamedo avarana associated with prameha causing sarvanga vata. So Rukshana therapy was given first, and then for vata samana, vasti were administered. Signs of pitta vitiation were not present in this case. To remove the kaphamedo avarana, Lasuna rasayana was given.
PATIENT’S PERSPECTIVE:
Not available
LEARNING POINTS:
In this case, the patient pre-diagnosed with cervical myelopathy presented with denied sensory and motor functions and was confined to bed. The patient regained his strength with Ayurvedic treatment, and his sensory functions improved. In further follow-ups, the patient was able to walk. Thus, Ayurveda can be considered an option for improving the quality of life in patients with cervical myelopathy.
INFORMED CONSENT
The patient gave written informed consent for publication.
ACKNOWLEDGEMENTS
Nil
CONFLICT OF INTEREST
None declared
FUNDING
None
REFERENCE
- Donnally III CJ, Hanna A, Odom CK. Cervical Myelopathy. [Updated 2022 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482312/
- Sharma PV, editor. Charaka Samhita, Chikitsa Sthana, Vata vyadhi Chikithsa Adhyaya,28/28,2nd ed. Varanasi Chaukhamba Sanskrit sanathan;1990.
Image 1. Timeline
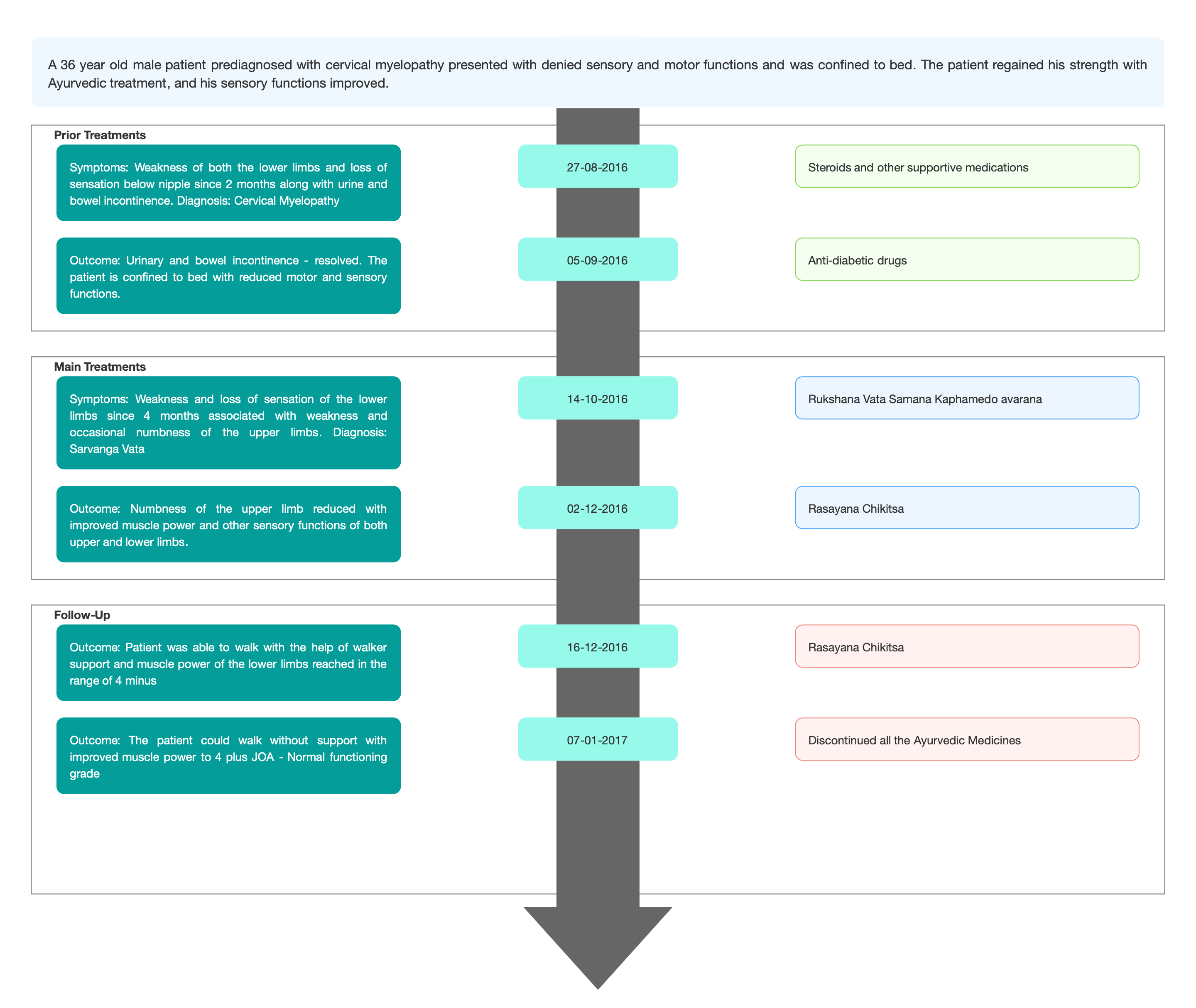
Image 2. Previous treatment records
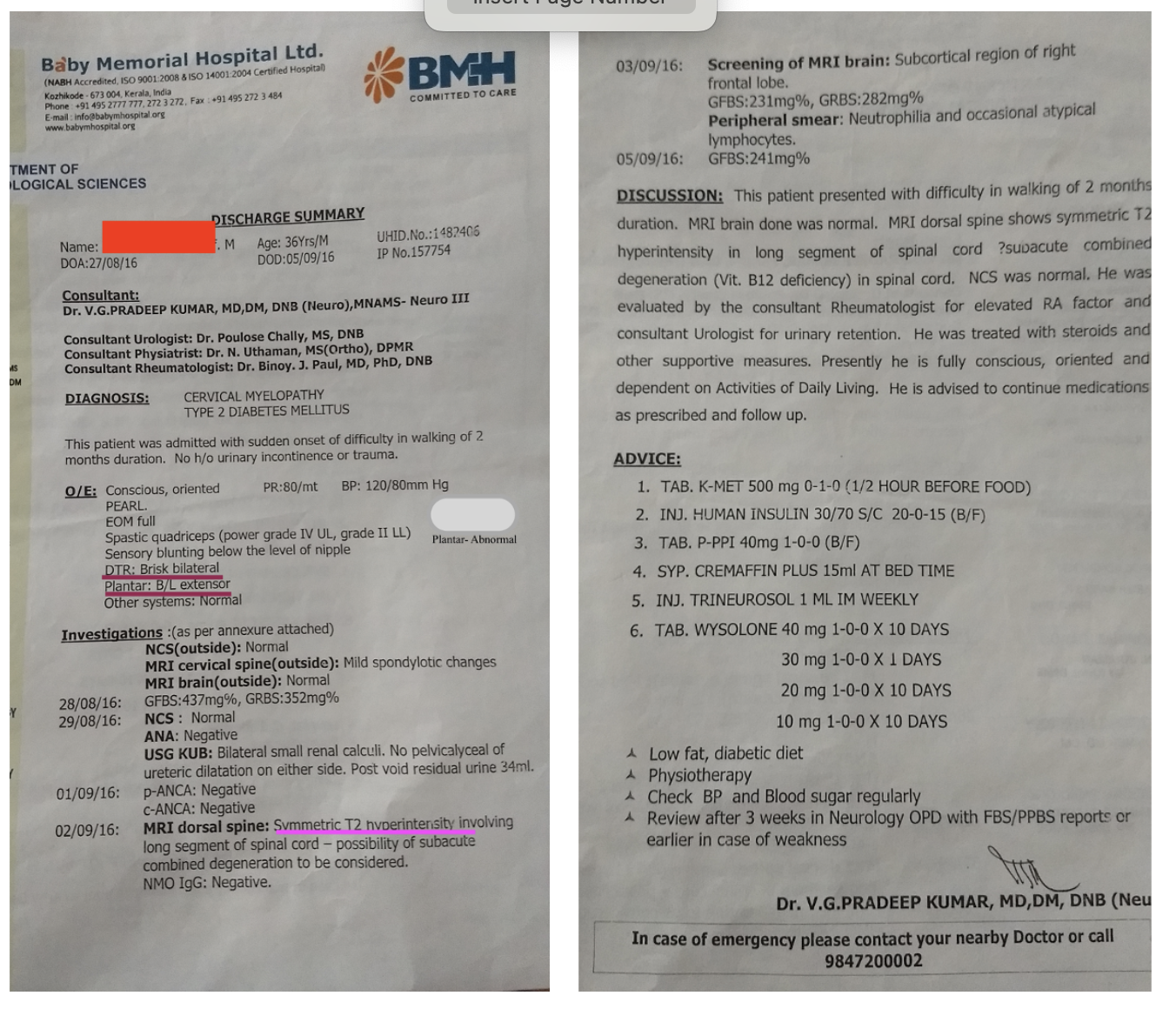
Image 3. JOA Score before and after treatment
-
Immersive Learning
-
Modern Diagnosis
Biomedical Diagnosis: Cervical myelopathy
About the disease:
Cervical myelopathy describes a spinal cord compression at the cervical level of the spinal column resulting in spasticity, hyperreflexia, pathologic reflexes, digit/hand clumsiness, and/or gait disturbance.
Diagnostic criteria: A detailed and thorough neurological examination plus MRI is the current standard to diagnose the presence of cervical myelopathy.
Treatment: Patients with cervical myelopathy treated with a conservative approach (anti-inflammatory medication and physical therapy) may have some short-term benefits in relieving painful symptoms. Patients with severe or disabling pain may also be helped with surgery. But there is always the risk of infection post-surgery.
Assessment: The JOA score may be a better method to evaluate the neurological function of patients with cervical myelopathy because it considers the pathophysiology of cervical myelopathy and provides a quantitative measure of outcomes
Biomedical Diagnosis of the case :
A 36-year-old diabetic male patient presented with weakness and loss of sensation in the lower limbs associated with weakness and occasional numbness of the upper limbs. The condition was pre-diagnosed as a case of cervical myelopathy by the Neurologist. Based on previous treatment records and clinical examinations, the physician confirmed the diagnosis and the Ayurvedic diagnosis Sarvanga vata.
Image 1. Diagnosis proof - Previous treatment records
Prognosis: Without treatment, patients may progress toward significant paralysis and loss of function. In this case, MRI findings showing High-intensity changes in T2 predict a poorer recovery rate and worse motor symptom improvements. With Ayurvedic treatment, numbness of the upper limb is reduced with improved muscle power and other sensory parameters of both upper and lower limbs. In further follow-ups, there were marked improvements in motor and sensory functions and the patient could walk without support.
Image 1.
-
Ayurveda Diagnosis
Ayurvedic Diagnosis: Sarvanga vata
About the disease
Due to the intake of various diets and regimens, Vata dosha gets vitiated and occupies rakta srotas in the body. Ruksha guna of Vata causes rukshatva and parushatva in the srotas , which is the key point in the samprapti of sarvanga vata.
According to Acharya Caraka in Vata vyadhi chikitsa
सर्वाङ्गुकुपिते वाते गात्रस्फुरणभञ्जने ||२५||
वेदनाभिः परीतश्च स्फुटन्तीवास्य सन्धयः |(Ca.Ci.28)
When vitiated Vata is located all over the body, it produces generalised fasciculation and breaking type of pain, different types of pain and generalised joint crepitus.
Prognosis:
सन्धिच्युतिर्हनुस्तम्भः कुञ्चनं कुब्जताऽर्दितः ||७२||
पक्षाघातोऽङ्गसंशोषः पङ्गुत्वं खुडवातता |
स्तम्भनं चाढ्यवातश्च रोगा मज्जास्थिगाश्च ये ||७३||एते स्थानस्य गाम्भीर्याद्यत्नात् सिध्यन्ति वा न वा |
नवान् बलवतस्त्वेतान् साधयेन्निरुपद्रवान् ||७४|| (Ca.Ci.28)These conditions can be cured when they are of recent origin in strong patients without any complications.
Treatment:
सर्वाङ्गकुपितेऽभ्यङ्गो बस्तयः सानुवासनाः ||९१||
When the vata is vitiated in the entire body, oil massage, evacuative enema, and unctuous enema should be given . This patient is 36 years old diabetic male patient who presented with weakness and loss of sensation of the lower limbs associated with weakness and occasional numbness of the upper limbs. The condition was prediagnosed as cervical myelopathy by the Neurologist, who was consulted. The patient was confined to bed with reduced motor and sensory functions. Based on the previous treatment records and clinical examination, the physician diagnosed the condition as sarvangavata.
Treatment rationale: In this patient, Santarpana janya bahudoshavastha lead to Prameha. Kaphamedo avarana associated with prameha causes the sarvanga vata. So Rukshana therapy was given first, and then for Vata samana, vasti was administered. Signs of pitta vitiation were not present in this case. To remove the kaphamedo avarana, Lasuna rasayana was given.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Gandharvahasthadi Kashayam Kashaya 60ml Oral at 6am before food 2016-10-14 - 2016-10-20 Sahasrayogam - Kashaya yoga prakarana Vaiswanara choorna Choornam 10gm Oral with kashayam - morning 2016-10-14 - 2016-10-20 Ashtanga hrudayam - Chikitsa sthanam 14/34 Amrithothara Kashaya Kashaya 60ml Oral at 6pm before food 2016-10-14 - 2016-10-20 Sahasrayogam, Kashaya yoga prakarana Udwarthanam with kolakulathadi churnam 7 days External application 2016-10-14 - 2016-10-20 Vaitarana vasti 3 days Per- rectal 2016-10-21 - 2016-10-23 Sahacharadi kashayam Kashayam 60ml Oral twice daily before food 2016-10-26 - 2016-11-06 Ashtanga hrudayam, Chikitsa sthana 21 Ekangaveera rasa Tablet 1-0-1 Oral 2016-10-26 - 2016-11-06 Bhaishajya Ratnavali, Vatavyadhi chikitsa Aswagandha choorna + Bala choorna Choornam 5gm twice daily Oral 2016-10-26 - 2016-11-06 Anubhuta yogam Dhanyamladhara 5 days External 2016-10-26 - 2016-10-30 Pizhinju thadaval with sahacharadi taila 7 days External 2016-10-31 - 2016-11-06 Erandamooladi niruha vasti 5 days – course of yogavasthi – 3 niruha and 2 matra vasti with pippalyadi anuvasana 40 ml Per- rectal 2016-11-07 - 2016-11-13 Lashuna Rasayana Rasayana 3gm Oral 2016-11-17 - 2016-11-20 Ashtanga -
Outcome Measures
OUTCOME MEASURES
A 36-year-old diabetic male patient presented with weakness and loss of sensation of the lower limbs associated with weakness and occasional numbness of the upper limbs. The condition was pre-diagnosed as a case of cervical myelopathy. The patient was confined to bed during the initial stage of treatment with reduced motor and sensory functions.
Assessment of Muscle power and other sensory and nervous functions were done throughout the treatment period. At the time of discharge, after 48 days of treatment, numbness of the upper limb reduced with improved muscle power and other sensory functions of both upper and lower limbs.
During the first follow-up after two weeks of discharge, the patient was able to walk with the help of walker support and muscle power of the lower limbs reached the range of 4 minus. In the second follow-up during the next month, the patient could walk without support with improved muscle power to 4 plus. Neurological condition assessed with JOA (Japanese Orthopedic Association) score indicates grade 2 before treatment has reached normal functioning grade after treatment.
Examination
Before treatment
After treatment
Finger nose touch
Intact
Intact
Heel shin test
Impaired
Possible
Tandem walking
Not possible
Possible
Light touch (b/l -LL)
Impaired
Intact
Deep touch (b/l -LL)
Impaired
Intact
Pain (LL)
Impaired
Intact
Temperature
Hot impaired on rt lower limb
Intact
Vibration
Impaired on both lower limb
Impaired
Stereognosis
Intact
Intact
Reflexes- Supinator
Present (b/l) +
++
- Biceps
Present (b/l) +
++
- Triceps
Present (b/l) +
++
- Knee
+
++
- Ankle
+
++
Motor system:
UL-
LL-
Grade 3 (b/l)
Grade 1 (b/l)
Grade 4+
Image1. Japanese Orthopedic Association Grading -before and after treatment
-