Featured Case
-
Abstract
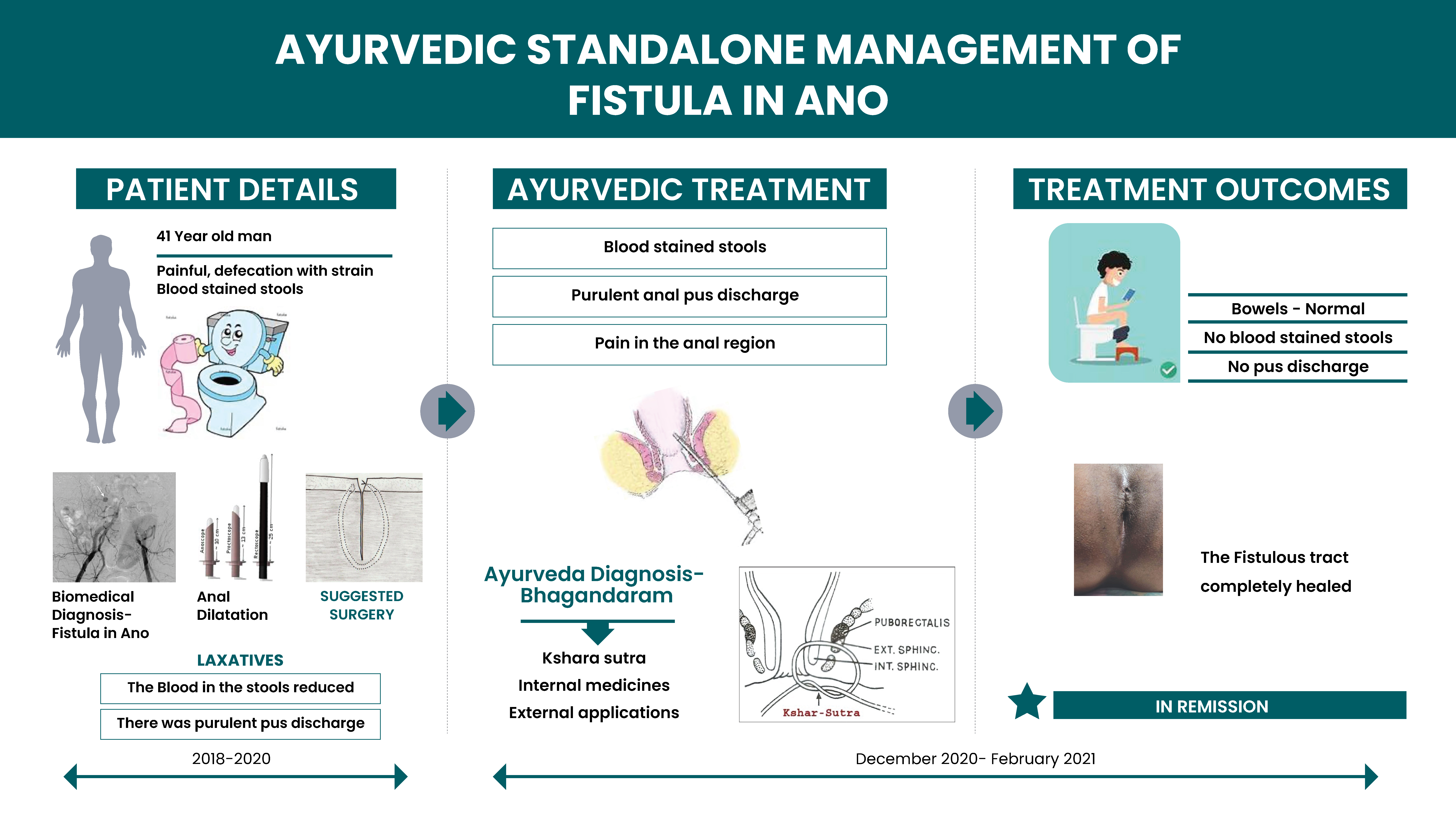
A 41-year-old male, was diagnosed with Fistula in Ano. The biomedical diagnosis was confirmed with rectal examination and MRI Fistulogram which. MRI Fistulogram revealed- well defined low anal linear simple fistulous tract 2mm in width and 2.5cms in length. Internal opening is at 6 o clock. The patient had been suffering from difficulty in passing stools and occasional blood-stained stools. He tried Anal dilatation and internal medicines, as prescribed by the General Physician, but there was no significant relief. On medication, the amount of blood discharge reduced but there was purulent pus discharge. After having tried conventional treatments for a period of over 2 years, he decided to try Ayurveda. He approached Dr Sreelekshmi who diagnosed this condition as Bhagandara. Anal fissure and skin tag were also diagnosed on rectal examination. Ksharasutra was the primary treatment scheduled to heal the fistulous tract. With 1 primary threading and 4 Kshara Sutra threading, the fistulous tract healed completely within 4 months. The last follow up was recorded after 8 months. There was no recurrence reported and on examination, the skin was perfectly healthy. The bowels are normal and satisfactory.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 41-year-old male, was diagnosed with Fistula in Ano. The biomedical diagnosis was confirmed with rectal examination and MRI Fistulogram which. MRI Fistulogram revealed- well defined low anal linear simple fistulous tract 2mm in width and 2.5cms in length. Internal opening is at 6 o clock. The patient had been suffering from difficulty in passing stools and occasional blood-stained stools. He tried Anal dilatation and internal medicines, as prescribed by the General Physician, but there was no significant relief. On medication, the amount of blood discharge reduced but there was purulent pus discharge. After having tried conventional treatments for a period of over 2 years, he decided to try Ayurveda. He approached Dr Sreelekshmi who diagnosed this condition as Bhagandara. Anal fissure and skin tag were also diagnosed on rectal examination. Ksharasutra was the primary treatment scheduled to heal the fistulous tract. With 1 primary threading and 4 Kshara Sutra threading, the fistulous tract healed completely within 4 months. The last follow up was recorded after 8 months. There was no recurrence reported and on examination, the skin was perfectly healthy. The bowels are normal and satisfactory.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Successful management of a Chronic Fistula in Ano with unsatisfactory response to conventional medicines, using Ksharasutra- an Ayurvedic Para surgical procedure. - A Case report
Dr Sreelekshmi VS
ABSTRACT
A 41-year-old male patient had been suffering from difficulty in passing stools, and blood stains in stools associated with pus discharge. He also had pain in the anus since 2 years. He consulted an allopath and was diagnosed with Anal fissure. He took conventional medicines and did anal dilatation. After a year, the blood in stools reduced but there was purulent pus discharge, and he felt worse. MRI Fistulogram (2.10.2020) revealed ‘well defined low anal linear simple fistulous (1) tract 2mm in width and 2.5cms in length.’ As he was not satisfied with the outcomes, the doctor suggested surgery but opined that it was not that successful. There was always a possibility of recurrence. So, the patient opted for Ayurveda and consulted Dr Sreelekshmi. The diagnosis was Bhagandara (2) and the line of treatment for the same was followed. With 1 Primary threading and 4 Ksarasutra the tract was completely healed. There has been no recurrence to date.
KEYWORDS
Fistula in Ano, Anal fistula, Bhagandara, Ksharasutra, Primary Threading
INTRODUCTION
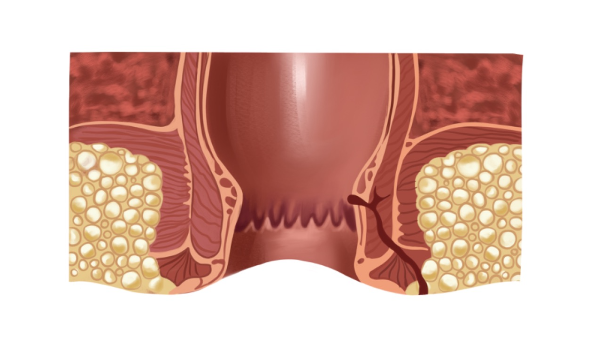
A fistula-in-ano or an Anal Fistula is an abnormal tract that is hollow, or a cavity lined with granulation tissue connecting a primary opening located inside the anal canal to another opening called a secondary opening located in the perianal skin. These secondary tracts can be multiple and may have their origin from the primary opening. This is a painful condition that can disrupt the normal activities of an individual. The symptoms are pus or blood exudation from the non-healing abscess, painful defecation, signs of infection like fever may also be present.
Diagnostic criteria: Physical examination and history taking are the primary diagnostic criteria. If the pain is too severe or it is a high-level fistula, then investigations like endoscopic ultrasound or MRI will be prescribed to identify the fistula tract. Internal fistulas may be evaluated using barium contrast X-ray, MRI or CT scan.
PATIENT INFORMATION
A 41-year-old male patient, presented with difficulty in passing stools, and bloodstains along with the stool for 2 years.
Medical History: The patient was normal 2 years back. He had difficulty passing stools. He had to strain to pass stool and gradually started seeing blood stains along with the stool. He assumed it was piles as he was mostly travelling, and diet was mainly non-veg. He consulted an allopathic doctor. On examination there was anal fissure. Anal dilatation was done to reduce the muscle spasm and internal medications were given for defecation without strain. The patient was still having difficulty passing stool and there was no significant relief. Blood stains were still present in the stools. After 1 year, the amount of blood discharge reduced but there was purulent pus discharge. He felt worse. He visited another allopathic doctor and an MRI Fistulogram (2.10.2020). Well defined low anal linear simple fistulous tract 2mm in width and 2.5cms in length. Internal opening at 6 o clock. Minimal left hydrocele was detected. The doctor suggested surgery as the best treatment option but opined that the success rate was very low, and there was a possibility of recurrence. So, the patient opted for Ayurvedic intervention. Patient also had Anal Fissure at 6 o clock position, and skin tag at 12 o clock position. He had no comorbidities. There was a history of Kidney stone 2 years back. He took conventional treatment and got relief.
Family History: Nothing significant.
Surgical History: Underwent Keyhole surgery in Knee 4 years back.
PHYSICAL EXAMINATION/CLINICAL FINDINGS
Moderate build. Vitals- BP- 120/80 mmhg. Pulse- 78/min, RR- 15/min. On Inspection- Acute anal fissure at 6 o clock position, Single external opening found at 6 o clock position. Skin tag at 12 o clock position. Palpation & Percussion were not done. On digital examination in the rectal wall- sphincter spasm present. Proctoscopy was not done due to the pain. On probing- tract is 2 cms deep to the posterior anal canal. The probe does not enter any body cavity and there is no discharge on withdrawal of the probe. Single fistulous tract with external opening at 6 o clock located. The colour of the surrounding skin is normal. There is no inflammation.
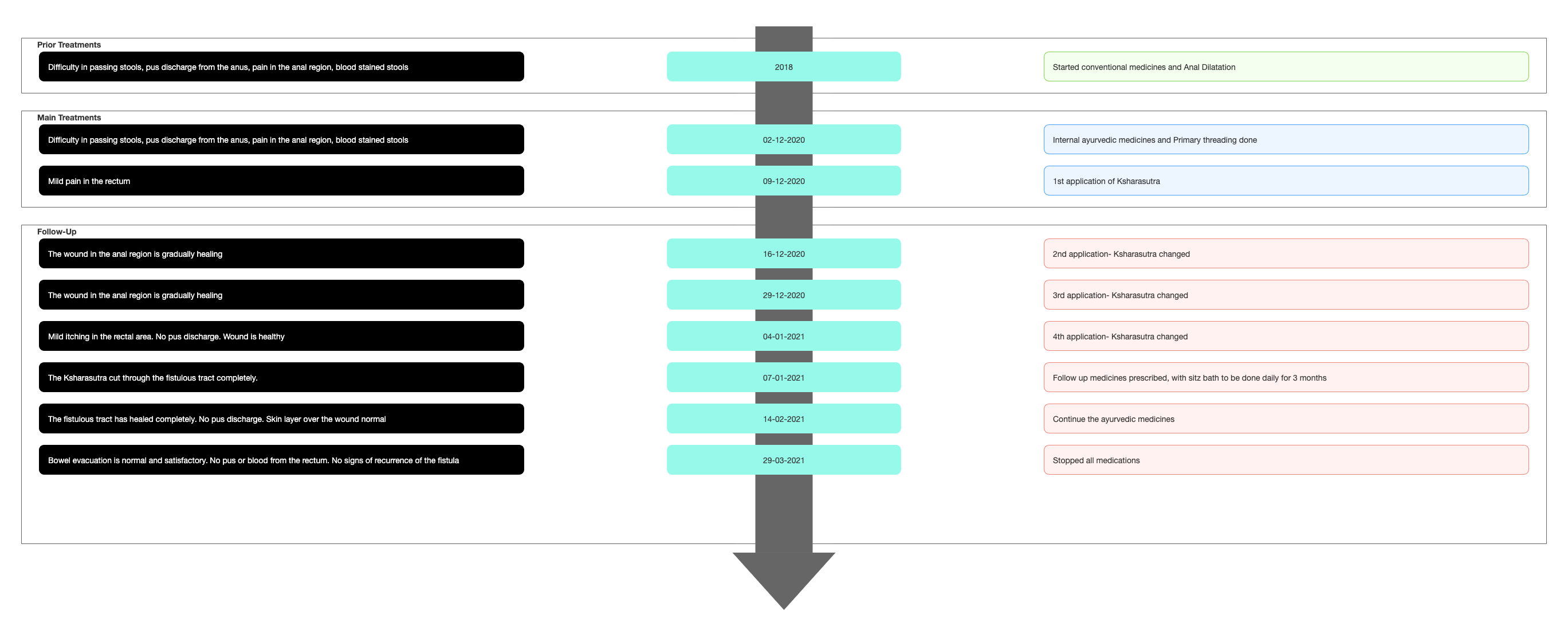
TIMELINE
Image 1. Timeline of events attached below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The diagnosis was made by clinical examination and confirmed with a Fistulogram (2.10.2020)
Image 2. MRI Fistulogram dated 2020 Attached below
Ayurvedic Assessment was done based on the clinical evaluation by the ayurvedic physician, supported by the confirmed diagnosis from the modern hospital.
Differential Diagnosis- This does not apply as the patient came in with a definite diagnosis.
Prognosis- There are surgical and non surgical options for the Treatment of Anal Fistula. Fistulectomy and Fistulotomy fibrin glue, fibrin plug, LIFT procedure and stem cell treatment are the options available. But the surgical procedures may cause complications like sphincter muscle damage leading to the incontinence of the sphincter, rectal prolapse, fecal soiling, and anal stenosis. Even after complete excision of the tract, the chances of recurrence are still present.
In this patient, surgery was suggested, but the doctor himself mentioned that surgery has a very low success rate. And recurrence was always a possibility. As the patient had tried anal dilatation and conventional medicine for more than a year, and the outcome was not satisfactory, he opted for Ayurveda.
THERAPEUTIC INTERVENTION
See the tab 'Treatment Details'
FOLLOW-UP AND OUTCOMES
4.1.21- Patient complained of itching, but there is no pus discharge, and it was a healthy wound. 7 follow ups were done in total. Minor changes were made in the prescription. In the 4th Follow up (7/1/21) the Ksara sutra cut through completely.
Clinician-based assessment; The Fistulous tract has completely healed, Bowels are normal. There is no rectal bleeding or pus discharge.
Image 3. Images were taken on 1.12.2021 (after 10 months of ayurvedic treatment): The site of the fistulous tract was healthy and there was no sign of recurrence. Attached below
Patient-assessed: Not relevant
Follow up test results: Not applicable in this patient.
Intervention adherence and tolerability– The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events: None reported
DISCUSSION:
Fistula in ano can be correlated to Bhagandaram mentioned in the Classical Ayurvedic texts based on the clinical presentation. The Ayurvedic Para surgical procedure- Kshara sutra is the best treatment option for Bhagandaram. The recurrence of a fistulous tract treated with Kshara sutra is not yet reported. Hence this treatment was chosen and was supported with internal medication and external applications to address the symptoms.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
Fistula in Ano is a surgical condition that bears side effects including anal incontinence. The chances of recurrence are also high. Kshara sutra is a very effective Para surgical procedure that helps heal the fistulous tract and recurrence is not yet reported. As there are expected side effects like Incontinence, from Fistulotomy and Fistulectomy, Kshara sutra becomes an appropriate choice for patients suffering from this condition.
INFORMED CONSENT
Written consent obtained from patient, for publishing this case report
ACKNOWLEDGEMENTS
None
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
1. Seow-Choen F, Nicholls RJ. Anal fistula. Br J Surg. 1992 Mar;79(3):197-205. doi: 10.1002/bjs.1800790304. PMID: 1555083.
2. Ahmad Mir, *Shaheen, & Kumar, P. H. (2017). Bhagandara and its management in Ayurveda: A conceptual study. International Journal of Ayurveda and Pharma Research, 5(8). Retrieved from http://ijaprs.com/index.php/ijapr/article/view/753
Image 1. Timeline of events
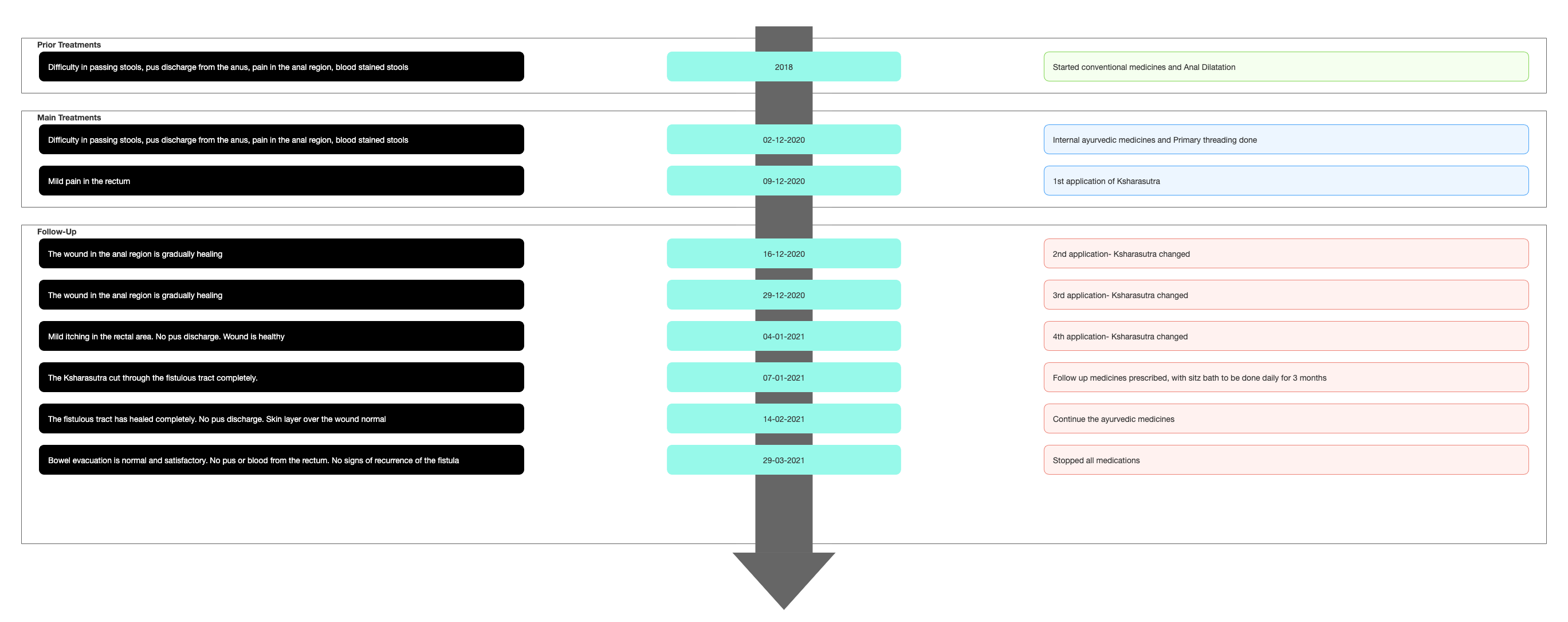
Image 2. MRI Fistulogram dated 2020 Attached below
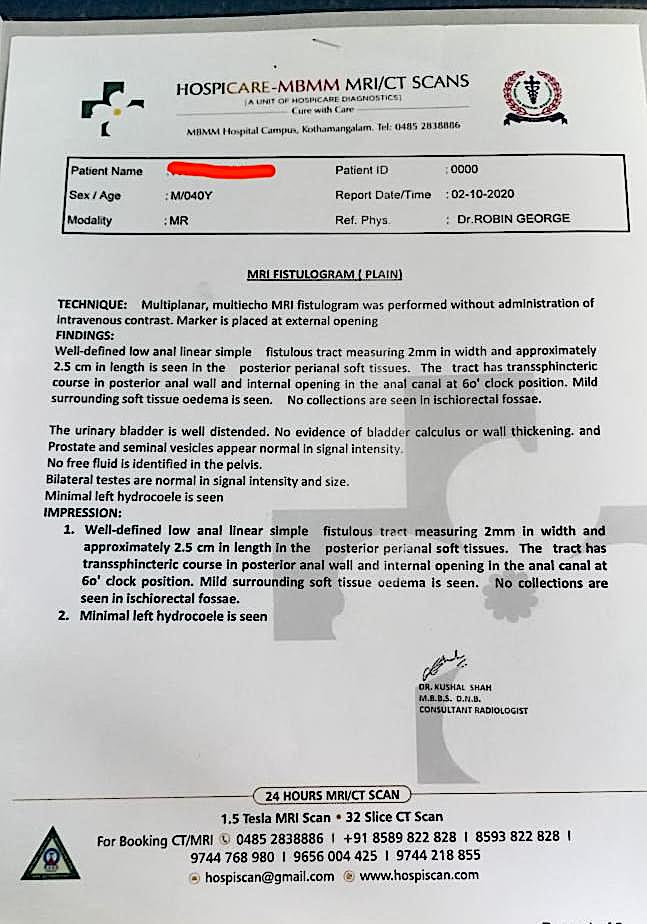
Image 3. Images were taken on 1.12.2021 (after 10 months of ayurvedic treatment):

-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Fistula in Ano
About the Disease:
A fistula-in-ano or an Anal Fistula is an abnormal tract that is hollow or a cavity lined with granulation tissue connecting a primary opening located inside the anal canal to another opening called a secondary opening located in the perianal skin. These secondary tracts can be multiple and may have their origin from the primary opening. This is a painful condition that can disrupt the normal activities of an individual. The symptoms are pus or blood exudation from the non-healing abscess, painful defecation, signs of infection like fever may also be present.
Diagnostic criteria: Physical examination and medical history are the primary diagnostic criteria. If the pain is too severe or it is a high-level fistula, then investigations like endoscopic ultrasound or MRI will be prescribed to identify the fistula tract. Internal fistulas may be evaluated using barium contrast X-ray, MRI or CT scan. The internal opening of the fistula can be identified with a Fistula probe, Anoscope, Flexible sigmoidoscopy or Colonoscopy, or an injected dye solution. In this patient, the diagnosis was confirmed with clinical examination and with a Fistulogram.
A 41 year old male patient, presented with difficulty in passing stools, and bloodstains in stools. On examination by a general physician, anal fissure was diagnosed. The symptoms persisted in spite of regular anal dilatation. Internal medications for easy defecation were prescribed. After 1 year, the the blood stains in the stools reduced but there was purulent pus discharge. MRI Fistulogram (2.10.2020) revealed well defined low anal linear simple fistulous tract 2mm in width and 2.5cms in length. Internal opening is at 6 o clock. Minimal left hydrocele is detected. The doctor suggested surgery as the best treatment option, and opined that the success rate of the surgery was very low.
Image 1. MRI Fistulogram October 2020 Attached below
Prognosis & Treatment:
There are surgical and non-surgical options of treatment. Fistulotomy, Endorectal advancement flap and Ligation of the intersphincteric fistula tract are the most commonly followed surgical procedure in the treatment of Fistula. The non-surgical procedures include seton placement, fibrin glue and collagen plug. But these procedures may cause complications like sphincter muscle damage leading to the incontinence of the sphincter, rectal prolapse, faecal soiling, and anal stenosis. Even after complete excision of the tract, the chances of recurrence are still present.
In this patient, surgery was recommended, but the doctor himself mentioned that surgery has a very low success rate. And recurrence was always a possibility. As the patient had tried anal dilatation and medications for more than a year, and the outcome was not satisfactory, he opted for Ayurveda.
Image 1. MRI Fistulogram October 2020
-
Ayurveda Diagnosis
AYURVEDIC DIAGNOSIS: Bhagandaram
About the Disease:
Taking into consideration the clinical presentation, fistula-in-ano or an Anal Fistula can be correlated to Bhagandara in the Ayurvedic texts.
Acarya Susruta, explains the presence of a deep-rooted apakva pidaka within two angular circumferences of Guda pradesha associated with pain and fever is called Bhagandara pidaka. When it suppurates and burst open, then it is called Bhagandara. This is listed as one amongst the Ashtamahagada. The word ‘Bhaga’ relates to all the structures around the guda, including the vasti and yoni. The Dharana (discontinuity) in the region of Bhaga, Guda and Vasti with surrounding skin surface is called Bhagandara. Vaghbhata mentions the formation of a Vrana to the size of a pidika, 1 or 2 angula from the anus or inside the anus (Utt.28/12-14). Rakta and mamsa are the vitiated dushyas. This results in the formation of a sinus, associated with pus discharge in the region of anus, perineum and bladder.
गुदस्य हि अग़्गुले क्षेत्रेपार्श्वतः पिडकार्तिकृत् ।
भिन्ना भगन्दरो ञेय स च पञ्चविधो मतः ॥Ma.Ni.46.1Susruta explains 5 types of Bhagandara, but Vaghbhata has mentioned 8 types of Bhagandara. Depending upon the dos?a responsible for the pathology, the respective symptoms will be produced. Here, the physician has not identified the type of Bhagandara. The colour of the skin around the anus is recorded as normal and there is no inflammation observed. The type of pain - whether toda, bheda, or sphurana are also not specified. So, the exact type of Bhagandara cannot be pointed out.
Prognosis: All the types of Bhagandara are painful and troublesome and are Krcchrasadhya. The incurable types are sannipataja, agantuja, bhagandara located in pravahini and sevani layer of the guda, and satapon?aka in the kshina.
In this patient, it was krcchrasadhya as it is a chronic condition. Though it is a low-level fistula, the patient did not respond to conventional medicines, and his symptoms still persisted. So surgery was suggested as the treatment option.
Treatment:
Gada Nigraha (Utt.7/10-14) mentions different types of treatment depending on the avastha. They are:
-
Bhagandara Pidika Cikitsa (Apakvavastha)
-
Bhagandara Cikitsa (Pakvavastha)
In Bhagandara Pidika Cikitsa, the treatment modalities specifically mentioned are Apatarpana, Alepa, Parisheka, Abhyanga, Swedana, Vimlapana, Upanaha, Pachana, Vishravana, Snehana, Vamana and Virechana (Su.Ci.8.4). Rakta Mokshana, Kshara Karma and Agni Karma are the most common parasurgical procedures done in Bhagandara. Out of these, the Kshara sutra is a very successful treatment widely practised by Ayurvedic physicians for rapid healing, with no recurrence of the fistulous tract.
In this patient, Kshara sutra was the primary treatment modality, supported by internal and external therapies. 1 primary threading and 4 Ksharasutra were applied before the patient got a complete cure for his condition.
Treatment rationale of the physician:
The Ayurvedic parasurgical procedure Kshara sutra is the best treatment option for Bhagandaram. The recurrence of a fistulous tract treated with Kshara sutra is not yet reported. Hence this treatment was chosen supported by internal medication and external applications. -
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Avipatti curnam Curnam 20 gms Oral, with warm water after food 2020-12-03 - 2020-12-29 Ashtanga Hrdayam Ka.2.21-23 Biogest Tablet Tablet 2-0-2 Oral, with warm water after food 2020-12-03 - 2020-12-08 Proprietary Medicine Abhayarishtam Arishtam 30 ml Oral, after food twice daily 2020-12-03 - 2020-12-08 Bhaisajya Ratnavali. Arshorogadhikara Aragvadhadi Kasayam Kasayam 10 ml Mix with 60 ml warm water, at bedtime 2020-12-03 - 2020-12-08 Ashtanga Hrdaya Su.15.17 Guggulupancapala Curna Curnam 10 gms Mix with required quantity of madhu and ghrta, twice daily after food 2020-12-03 - 2020-12-08 Sahasra yogam. Curna Prakarana. Ciruvilvadi Kasayam Kasayam 15 ml Mix with 40 ml warm water, twice daily before food 2020-12-03 - 2020-12-08 Sahasra yoga, Kashaya Prakarana Biogest Tablet Tablet 1-0-0 Oral, with warm water after food 2020-12-16 - 2021-01-06 Proprietary Medicine Abhayarishtam Arishtam 30 ml After food, twice daily 2020-12-16 - 2021-01-03 Guggulupancapala Curna Curnam 10 gms Mix with required quantity of madhu and ghrta, twice daily after food 2020-12-16 - 2021-01-06 Ciruvilvadi Kasayam Kasayam 15 ml Mix with 40 ml warm water, twice daily before food 2020-12-30 - 2021-01-03 Styplon Tablet Tablet 1-0-1 After food, if there is rectal bleeding 2020-12-30 - 2021-01-03 Proprietary Medicine Aragvadhadi Kasayam Kasayam 10 ml Mix with 60 ml warm water, at bedtime 2021-01-04 - 2021-01-06 Styplon Tablet Tablet 2-0-2 Oral, with warm water after food 2021-01-07 - 2021-01-22 Mustakaranjadi Kasayam Kasayam 10 ml Mix with 60 ml warm water, at bedtime 2021-01-23 - 2021-01-29 Sahasra yoga. Kasaya Prakarana Kankayana Vati Vati 1-0-1 Oral, with warm water 2021-01-23 - 2021-01-29 Bhaishajya Ratnavali. Gulmarogadhikara. Biogest Tablet Tablet 1-0-1 Oral, with warm water after food 2021-01-23 - 2021-01-29 Guggulupancapala Curna Curnam 5 gms Mix with sufficient quantity of madhu and taken at bedtime 2021-01-23 - 2021-01-29 Primary Threading- Seton thread Primary .... External application through the fistulous tract 2020-12-02 - 2020-12-02 Apamarga Ksharasutra Ksharasutra - done on 16.12/29.12/4.1 and 7.1 - 2021 Single thread External application through the fistulous tract 2020-12-09 - 2020-12-09 Anubhuta Yogam Murivenna Tailam Tailam Required quantity Rectal infiltration, whenever threading was done 2020-12-02 - 2021-01-07 Anubhuta Yogam Triphala Jalam Drava Required quantity Sitz bath for 20 minutes daily 2020-12-03 - 2021-02-28 Anubhuta Yogam WH 5 Cream Required quantity Local External application 2021-01-04 - 2021-01-29 Proprietary Medicine -
Outcome Measures
OUTCOME MEASURES
The 41 year old male patient was diagnosed with a Low-level linear fistula, confirmed with MRI Fistulogram. He had tried conventional medicines and anal dilatation for a period of more than 1 year, but the outcome was not satisfactory. The blood stains in stool reduced but there was purulent pus discharge. His doctor suggested surgery as the best treatment option, but mentioned that the success rate was very low, and there was a high recurrence rate. So the patient now opted for Ayurveda.
Both subjective and objective parameters were assessed to analyse the outcome of the ayurvedic treatments.
Subjective parameters: In total, 7 follow-ups were done. The Kshara sutra cut through the fistulous tract after 1 primary threading and 4 Kshara sutra application. But 3 more follow-ups were done to assess the condition post the ayurvedic treatments. To address the symptoms of the patient, supportive internal medicines and external applications were also given.
On 4.1.21: Patient complained of itching, but there was no pus discharge and it was a healthy wound. Minor changes were made in the prescription. In the 4th Follow up (7/1/21) the Kshara sutra cut through the fistulous tract completely.
The wound healed completely. The patient has no anal pus discharge or bloodstained stools. Bowels are normal and satisfactory.
Objective parameters:
At the baseline, photographs were not taken, as the Fistulogram confirmed the diagnosis. Photographs were taken recently to check for any recurrence. The wound site was healthy. There had been no recurrence to date.Image 1. Photos taken after 10 months of Ayurvedic treatment attached below
-