Featured Case
-
Abstract
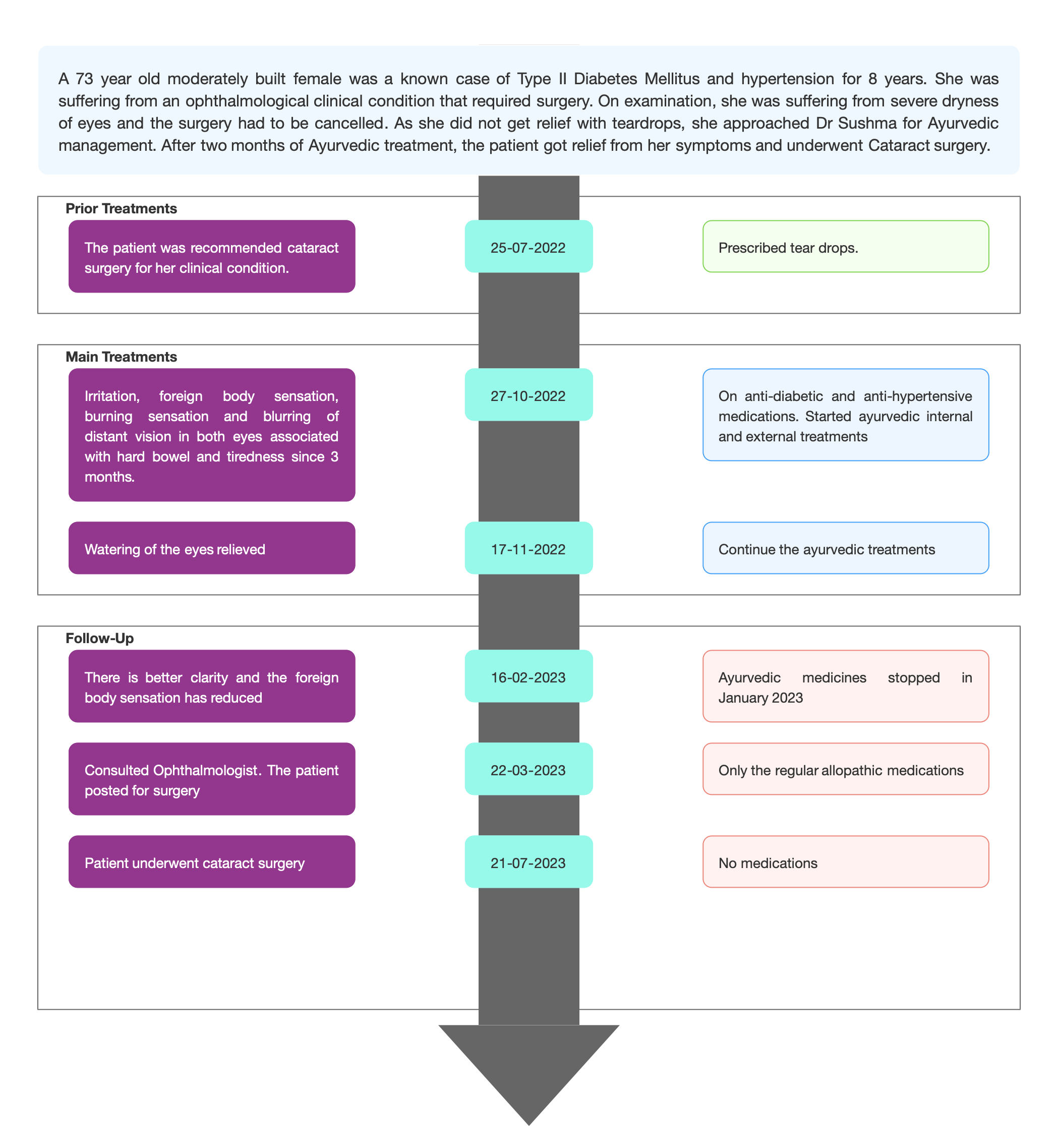
A 73 year old moderately built female, a known case of Type II Diabetes Mellitus and hypertension for 8 years, found to be suffering from BE grade 2 NS with PSC Left greater than Right. She was advised cataract surgery. During the preoperative examination, it was found that the patient was suffering from severe dry eye and the scheduled surgery was cancelled. She was prescribed teardrops and was advised to revisit for an evaluation after a month. The patient’s condition did not improve and so she approached Dr Sushma for Ayurvedic management. Based on the previous treatment records and the clinical evaluation, the Biomedical diagnosis was made as Aqueous Deficient Dry Eye and the Ayurvedic diagnosis was Shushkakshi paka- Vata pittaja. The line of treatment followed is Amapacana and vata-pitta hara. The treatment also targeted the shodhana of the vitiated vata and pitta. After two months of Ayurvedic treatments, the patient got relief from her symptoms and underwent Cataract surgery. This case report demonstrates the successful standalone ayurvedic management of ADD in a patient who could not undergo cataract surgery due to the dry eyes.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 73 year old moderately built female, a known case of Type II Diabetes Mellitus and hypertension for 8 years, found to be suffering from BE grade 2 NS with PSC Left greater than Right. She was advised cataract surgery. During the preoperative examination, it was found that the patient was suffering from severe dry eye and the scheduled surgery was cancelled. She was prescribed teardrops and was advised to revisit for an evaluation after a month. The patient’s condition did not improve and so she approached Dr Sushma for Ayurvedic management. Based on the previous treatment records and the clinical evaluation, the Biomedical diagnosis was made as Aqueous Deficient Dry Eye and the Ayurvedic diagnosis was Shushkakshi paka- Vata pittaja. The line of treatment followed is Amapacana and vata-pitta hara. The treatment also targeted the shodhana of the vitiated vata and pitta. After two months of Ayurvedic treatments, the patient got relief from her symptoms and underwent Cataract surgery. This case report demonstrates the successful standalone ayurvedic management of ADD in a patient who could not undergo cataract surgery due to the dry eyes.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Successful ayurvedic management of Aqueous deficient dry eye- a case report
Dr Sushma NS
ABSTRACT
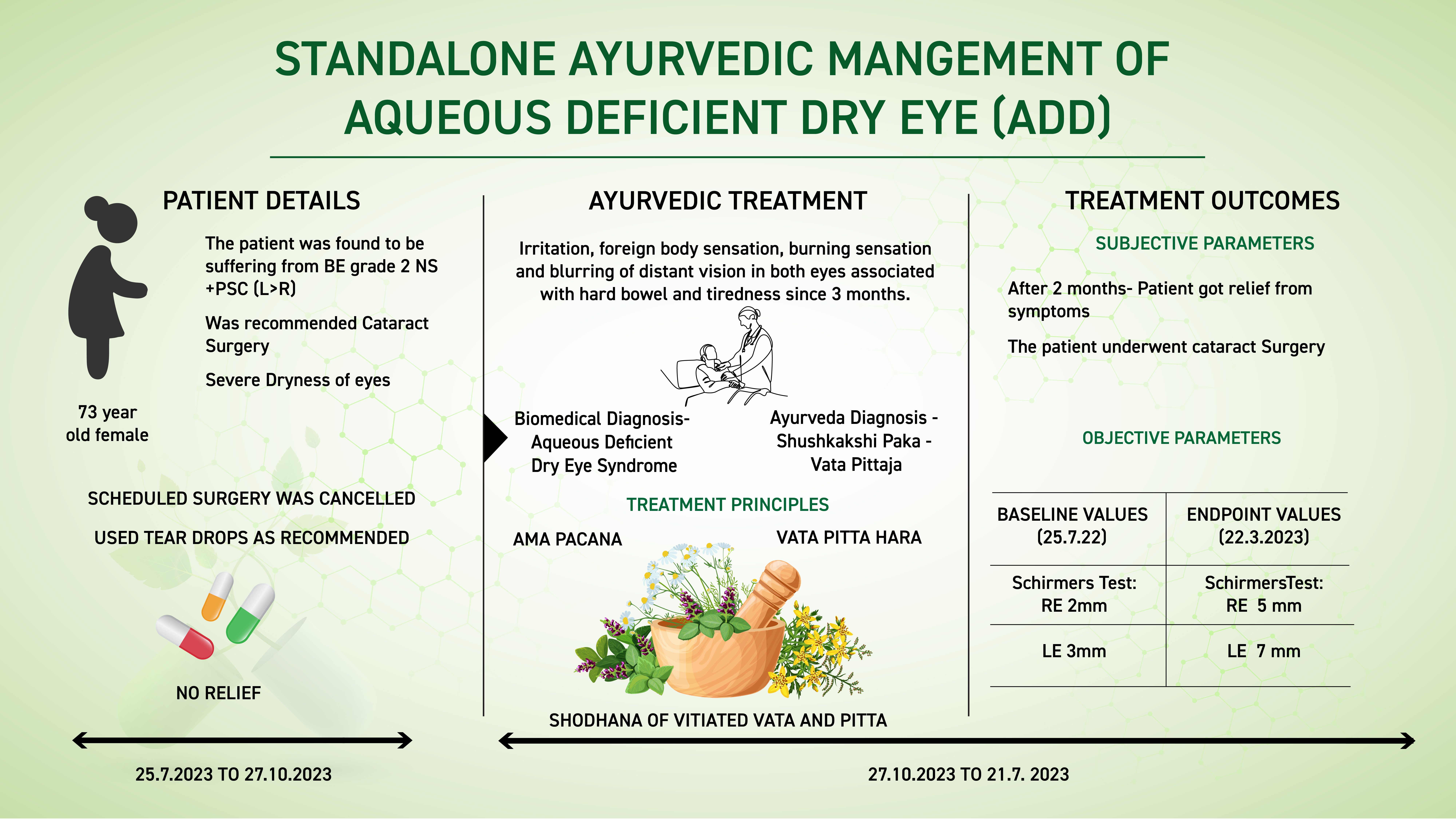
A 73-year-old moderately built female, a known case of Type II Diabetes Mellitus and hypertension for 8 years, found to be suffering from BE grade 2 NS +PSC (L>R). She was advised cataract surgery. During the pre-operative examination, it was found that the patient was suffering from severe dry eye and the scheduled surgery was cancelled. She was prescribed teardrops and was advised to re-visit for an evaluation after a month. The patient’s condition did not improve and so she approached Dr Sushma for Ayurvedic management. Based on the previous treatment records and the clinical evaluation, the Biomedical diagnosis was Aqueous Deficient Dry Eye Syndrome and the Ayurvedic diagnosis was Shushkakshi paka- Vata pittaja. The line of treatment followed is Amapacana and vata-pitta hara. The treatment also targeted the shodhana of the vitiated vata and pitta. After two months of Ayurvedic treatment, the patient got relief from her symptoms and underwent Cataract surgery. This case report demonstrates the successful standalone ayurvedic management of ADD in a patient who could not undergo cataract surgery due to the dry eyes.
KEYWORDS
Dry eye, Non-Sjögren's syndrome, aqueous deficiency, shushkakshipaka, case report, ayurveda.
INTRODUCTION
One uncommon form of dry eye is called aqueous-deficient dry eye (ADDE), also known as aqueous tear-deficient dry eye. ADDE causes your tear glands to not make enough tears to keep your eyes moist. This can result in eye irritation or damage.
Symptoms-
- pain in your eyes without a clear cause
- burning sensation, especially when you blink
- noticeable redness in your eyes
- eye itchiness
- a sensation that you have something stuck in your eye, like dirt or sand
- blurred vision, especially when reading
- eye fatigue after reading or looking at a screen for even short periods of time
- difficulty putting in contact lenses or wearing them for a long period of time
- a lack of tears when you cry
Causes: ADDE happens when your tear glands (also known as your lacrimal glands) do not make enough fluid to properly lubricate the eye. There are two main types of ADDE, depending on their cause:
Sjögren’s-related: Sjögren’s disease is an autoimmune condition that affects your body’s ability to produce fluids. This includes tears and saliva.
Non-Sjögren’s-related: This type is not related to Sjögren’s disease. Age is one of the most common factors for ADDE in people who don’t have Sjögren’s.
Some other common risk factors for the second type of ADDE can include:
- other autoimmune conditions, such as lupus or rheumatoid arthritis
- undergoing hormone replacement therapy
- conditions that affect the eye, eyelids, or eyelashes, such as blepharitis or seborrheic dermatitis
- not blinking enough during long periods of using electronic devices
- being in very dry indoor environments, especially when running HVAC systems for long periods
- not getting enough vitamin A or omega-3 fatty acids in your diet
- using antihistamines or blood pressure medications that affect eye lubrication
- complications from an eye injury, especially from chemicals or damaging substances
- receiving orbital radiotherapy for treatment of cancer in the mouth or eyes
Diagnostic criteria- Here are some of the most common methods that a doctor or eye doctor might use to diagnose ADDE:
Blink frequency: A doctor examines how often you blink in 1 minute. You may have ADDE if you blink less than once every 30 seconds.
Ocular surface staining: A doctor stains your eye’s surface with specialized sodium drops and looks at the eye through a slit lamp to see if there’s damage to any of the eye’s protective layers.
Tear film breakup time: A doctor tracks for the film of tear fluid to break up after you blink and lubricate your eye using the same specialized eye drops. You may have ADDE if the tear film breaks up in fewer than 8 to 10 seconds.
Tear lake: A doctor looks at the amount of tears along the edges of your lower eyelid as they spill out onto the eye surface. You might have ADDE if this reservoir of tears is less than 0.2 mm across.
Eyelid examination: ADDE often leads to eyelid symptoms and debris on the eyelids that can cause redness or eyelid thickening. A close examination of your eyelids can help diagnose ADDE.
Tear analysis: A doctor takes a tear sample to analyze the tear fluid for high concentrations of blood or inflammation.
Schirmer’s test: A doctor numbs your eyes with special eye drops and inserts a small strip of paper into each eye to see how much fluid fills up the paper. You might have ADDE if the paper comes out and measures less than 10 mm down a strip of paper.
Prognosis & Treatment available: Dry eye disease is often considered chronic, with periods of exacerbation due to intermittent contributing factors. More severe diseases can result in corneal complications, including infectious keratitis, ulceration, and scarring, which may cause subsequent loss of vision.In this clinical presentation, patient was suffering from BE grade 2 NS +PSC (L>R), and was advised cataract surgery. As the patient was suffering from severe dry eye the scheduled surgery was cancelled. Even though the patient was under the standard of care medications for three months, she was non-responsive to the biomedical treatment. After two months of Ayurvedic treatments, the patient could be posted for cataract surgery after confirming the ocular surface stability.
The general treatments administered are:
- using eye drops or other lubricants to keep your eyes moist
- using lid wipes to reduce bacterial buildup on your eyelids that can lead to irritation or infection
- applying prescription topical treatments like corticosteroids
- applying warm compresses to your eyes to reduce irritation and swelling
PATIENT INFORMATION
In this case report, A 73-year-old moderately built female, a known case of Type II Diabetes Mellitus and hypertension for 8 years, found to be suffering from BE grade 2 NS +PSC (L>R). She was advised cataract surgery. During the pre-operative examination, it was found that the patient was suffering from severe dry eye and the scheduled surgery was cancelled. She was prescribed teardrops and was advised to re-visit for an evaluation after a month. The patient’s condition did not improve and so she approached Dr Sushma for Ayurvedic management.
No relevant family/surgical/psychosocial/genetic history.
Addictions- Nil
CLINICAL FINDINGS
General examination: Visual Acuity. Non-Contact Tonometry:
Slit Lamp Examination:
Tear film Break Up Time
Schirmer’s Test
Lens examination
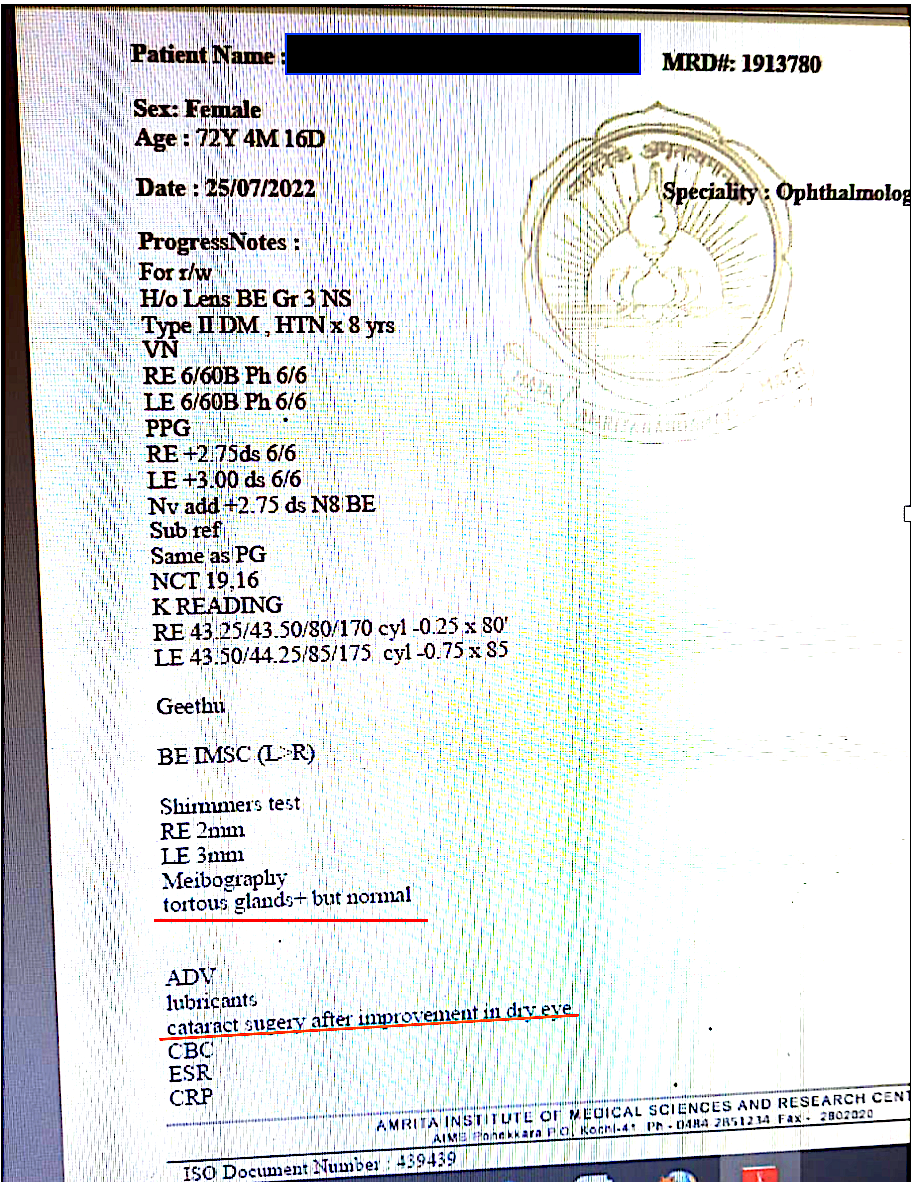
General eye examination: Visual Acuity. Non-Contact Tonometry: 19, 16
K reading RE -43.25/43.50/80/170 cyl -0.25*80
LE - 43.50/44.25/85/175 cyl -0.75*85
Slit Lamp Examination:
Tear film Break Up Time: RE 4 s; LE 6s
Corneal Staining with Fluorescein dye revealed mucus debris.
Schirmer’s Test: RE 0 mm, LE 0 mm
Lens examination: Both eye Grade 3NS
Meibography revealed a tortuous gland – but normal
TIMELINE
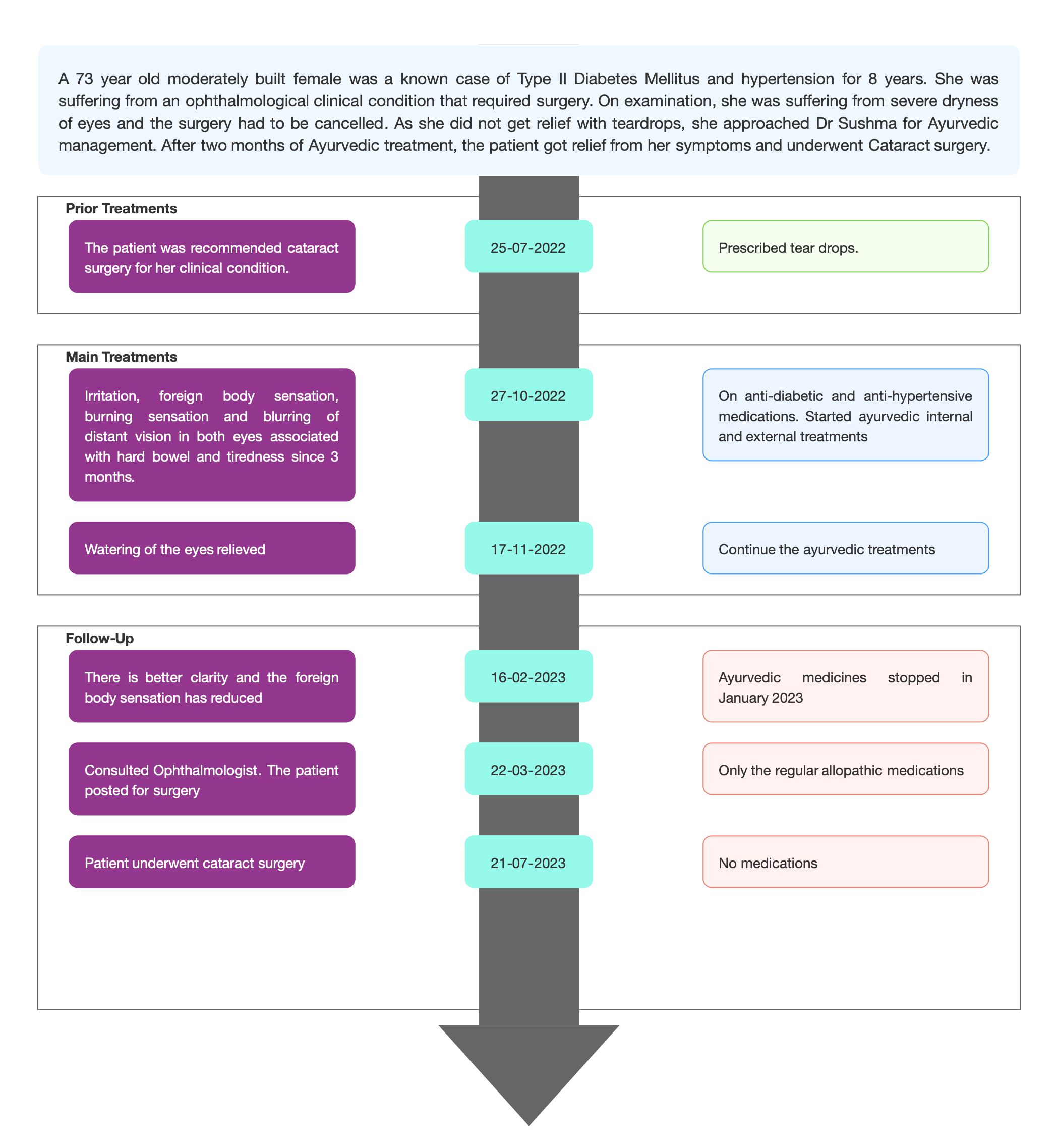
Image 1. Timeline of events added below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter; The condition was pre diagnosed as Aqueous deficient dry eye.
Image 2. Diagnosis proof document at baseline dated 25.7.2022
Ayurvedic Assessment was done based on the presenting complaints, and the clinical evaluation.
Table 1. Examination of the eye at baseline
O/E
Right Eye
Left Eye
Eyelid
WNL, Normal Meibomian gland orifice.
WNL, Normal Meibomian gland orifice.
Conjunctiva
The mild congestion in bulbar conjunctiva Concretions present In palpebral conjunctiva of the lower lid.
The mild congestion in bulbar conjunctiva Concretions present. In palpebral conjunctiva of the lower lid.
Sclera
White
White
Cornea
Senile arcus present, Lustreless
Senile arcus present, Lustreless
Pupil
Small size, sluggish reaction
Small size, sluggish reaction
Prognosis & Treatment available: Dry eye disease is often considered chronic, with periods of exacerbation due to intermittent contributing factors. More severe diseases can result in corneal complications, including infectious keratitis, ulceration, and scarring, which may cause subsequent loss of vision. In this clinical presentation, patient was suffering from BE grade 2 NS +PSC (L>R), and was advised cataract surgery. As the patient was suffering from severe dry eye the scheduled surgery was cancelled. Even though the patient was under the standard of care for three months, she was non-responsive to the treatment. But after two months of Ayurvedic treatments, the patient could be posted for cataract surgery after confirming the ocular surface stability.
THERAPEUTIC INTERVENTION
Please refer the tab ‘Treatment’ in the Portal.
FOLLOW-UP AND OUTCOMES
Both objective and subjective parameters were assessed to analyse the outcome of the ayurvedic treatment.
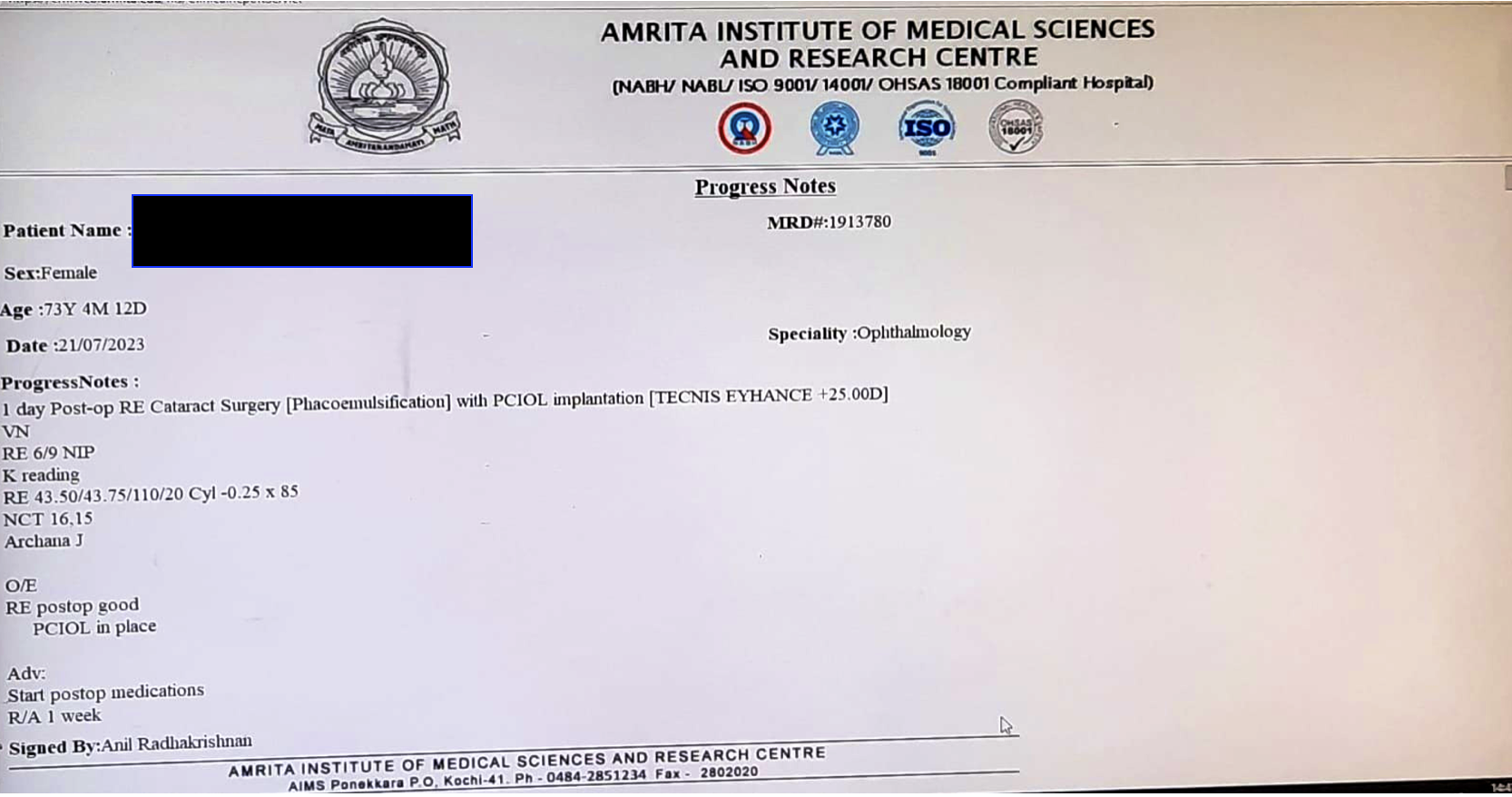
Subjective parameters: After 2 months- Patient got relief from all the symptoms. And she could undergo the cataract surgery as planned earlier by the Ophthalmologist.
Objective parameters: A complete cataract work up was done, at endpoint, to confirm the eligibility of the patient for surgery. The After 2 months- Patient got relief from symptoms
The Schirmers Test: RE 2mm and LE 3mm at baseline, became RE 5mm and LE 7mm at endpoint.
Clinician-based assessment; After two months of follow-up, Schirmer’s test improved to RE 5mm, LE 7mm with reduced tear film hyperosmolarity and the patient could be posted for cataract surgery after confirming the ocular surface stability.
Patient-assessed; Not relevant
Image 3. Progress notes and Cataract work up at endpoint dated 22.3.2023.
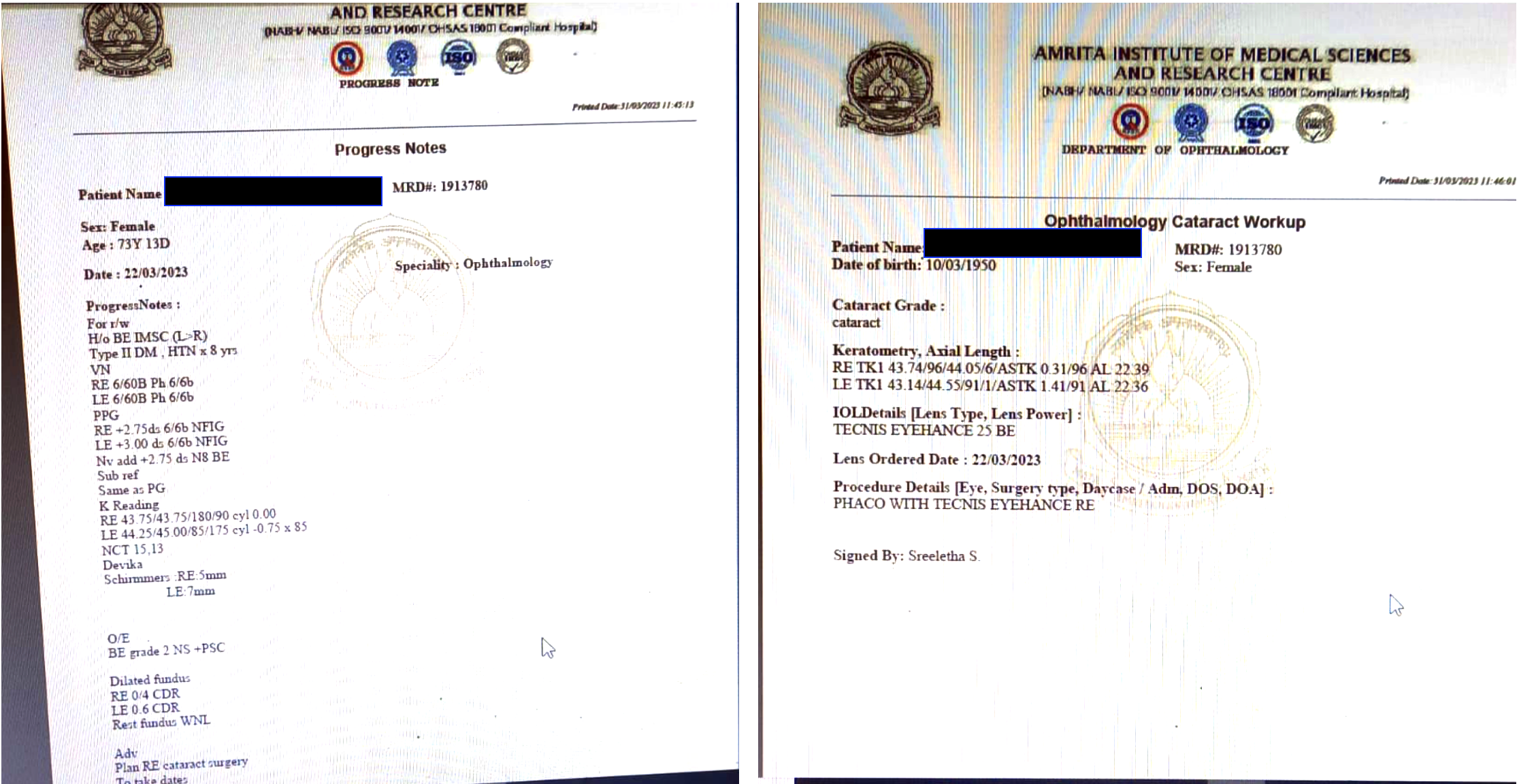
Image 4. Proof document for cataract surgery dated 21.7.2023
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported
DISCUSSION:
The patient was actually suffering from BE grade 2 NS +PSC (L>R), and had to undergo cataract surgery to address her symptoms. But on examination, as she had severe dryness of eyes, she could not be posted for surgery. She did not get relief following the prescription by the Ophthalmologist. So she opted for Ayurveda, to get relief from the dryness of eyes. The ayurvedic diagnosis was Shushkakshi paka, and the line of treatment was Amapacana and vata-pitta hara. The treatment also targeted the shodhana of the vitiated vata and pitta. With 2 months of treatment, she got relief from her symptoms and could undergo cataract surgery.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE HOME MESSAGES
This case report, highlights the potential benefits of Ayurveda as a complementary or preparatory treatment in certain medical conditions, particularly when conventional medicine fails to provide satisfactory results. A holistic approach to healthcare that integrates both conventional and alternative therapies can provide the best outcomes for patients.
INFORMED CONSENT
Written consent obtained from patient for publishing of the case report in the Portal
ACKNOWLEDGEMENTS
None specified
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
- https://www.healthline.com/health/aqueous-deficient-dry-eye
-
Immersive Learning
-
Modern Diagnosis
BIOMEDICAL DIAGNOSIS: Aqueous Deficient Dry Eye
ABOUT THE DISEASE:
One uncommon form of dry eye is called aqueous-deficient dry eye (ADDE), also known as aqueous tear-deficient dry eye. ADDE causes your tear glands to not make enough tears to keep your eyes moist. This can result in eye irritation or damage.
Symptoms-
- pain in your eyes without a clear cause
- burning sensation, especially when you blink
- noticeable redness in your eyes
- eye itchiness
- a sensation that you have something stuck in your eye, like dirt or sand
- blurred vision, especially when reading
- eye fatigue after reading or looking at a screen for even short periods of time
- difficulty putting in contact lenses or wearing them for a long period of time
- a lack of tears when you cry
Causes: ADDE happens when your tear glands (also known as your lacrimal glands) do not make enough fluid to properly lubricate the eye. There are two main types of ADDE, depending on their cause:
Sjögren’s-related: Sjögren’s disease is an autoimmune condition that affects your body’s ability to produce fluids. This includes tears and saliva.
Non-Sjögren’s-related: This type is not related to Sjögren’s disease. Age is one of the most common factors for ADDE in people who don’t have Sjögren’s.
Some other common risk factors for the second type of ADDE can include:
- other autoimmune conditions, such as lupus or rheumatoid arthritis
- undergoing hormone replacement therapy
- conditions that affect the eye, eyelids, or eyelashes, such as blepharitis or seborrheic dermatitis
- not blinking enough during long periods of using electronic devices
- being in very dry indoor environments, especially when running HVAC systems for long periods
- not getting enough vitamin A or omega-3 fatty acids in your diet
- using antihistamines or blood pressure medications that affect eye lubrication
- complications from an eye injury, especially from chemicals or damaging substances
- receiving orbital radiotherapy for treatment of cancer in the mouth or eyes
Diagnostic criteria- Here are some of the most common methods that a doctor or eye doctor might use to diagnose ADDE:
Blink frequency: A doctor examines how often you blink in 1 minute. You may have ADDE if you blink less than once every 30 seconds.
Ocular surface staining: A doctor stains your eye’s surface with specialized sodium drops and looks at the eye through a slit lamp to see if there’s damage to any of the eye’s protective layers.
Tear film breakup time: A doctor tracks for the film of tear fluid to break up after you blink and lubricate your eye using the same specialized eye drops. You may have ADDE if the tear film breaks up in fewer than 8 to 10 seconds.
Tear lake: A doctor looks at the amount of tears along the edges of your lower eyelid as they spill out onto the eye surface. You might have ADDE if this reservoir of tears is less than 0.2 mm across.
Eyelid examination: ADDE often leads to eyelid symptoms and debris on the eyelids that can cause redness or eyelid thickening. A close examination of your eyelids can help diagnose ADDE.
Tear analysis: A doctor takes a tear sample to analyze the tear fluid for high concentrations of blood or inflammation.
Schirmer’s test: A doctor numbs your eyes with special eye drops and inserts a small strip of paper into each eye to see how much fluid fills up the paper. You might have ADDE if the paper comes out and measures less than 10 mm down a strip of paper.
In this case report, a 73-year-old moderately built female, a known case of Type II Diabetes Mellitus and hypertension for 8 years, found to be suffering from BE grade 2 NS +PSC (L>R). She was advised cataract surgery. During the pre-operative examination, it was found that the patient was suffering from severe dry eye and the scheduled surgery was cancelled. She was prescribed teardrops and was advised to re-visit for an evaluation after a month. The patient’s condition did not improve and so she approached Dr Sushma for Ayurvedic management. Based on the previous treatment records and the clinical evaluation, the Biomedical diagnosis was Aqueous Deficient Dry Eye Syndrome and the Ayurvedic diagnosis was Shushkakshi paka- Vata pittaja.
Image 1. Diagnosis proof document dated 25.7.2022
Table 1. Examination of the eye at baseline
O/E
Right Eye
Left Eye
Eyelid
WNL, Normal Meibomian gland orifice.
WNL, Normal Meibomian gland orifice.
Conjunctiva
The mild congestion in bulbar conjunctiva Concretions present In palpebral conjunctiva of the lower lid.
The mild congestion in bulbar conjunctiva Concretions present. In palpebral conjunctiva of the lower lid.
Sclera
White
White
Cornea
Senile arcus present, Lustreless
Senile arcus present, Lustreless
Pupil
Small size, sluggish reaction
Small size, sluggish reaction
Prognosis & Treatment available: Dry eye disease is often considered chronic, with periods of exacerbation due to intermittent contributing factors. More severe diseases can result in corneal complications, including infectious keratitis, ulceration, and scarring, which may cause subsequent loss of vision.In this clinical presentation, patient was suffering from BE grade 2 NS +PSC (L>R), and was advised cataract surgery. As the patient was suffering from severe dry eye the scheduled surgery was cancelled. Even though the patient was under the standard of care medications for three months, she was non-responsive to the biomedical treatment. After two months of Ayurvedic treatments, the patient could be posted for cataract surgery after confirming the ocular surface stability.
The general treatments administered are:
- using eye drops or other lubricants to keep your eyes moist
- using lid wipes to reduce bacterial buildup on your eyelids that can lead to irritation or infection
- applying prescription topical treatments like corticosteroids
- applying warm compresses to your eyes to reduce irritation and swelling
Reference
-
Ayurveda Diagnosis
AYURVEDIC DIAGNOSIS: Shushkashipaka- Vata pittaja
About the disease:
Netra Roga are classified into different types depending upon the Dosha predominance, location and surgical treatment. Depending on the dosa predominance, there are 76 Netra rogas. Depending on the location, according to Sushruta there are 76, according to Bhavaprakasha 78, according to Ashtanga Hrdaya and Sangraha, there are 94. According to the surgical treatment, there are 33.
In this case report, a 73-year-old moderately built female, a known case of Type II Diabetes Mellitus and hypertension for 8 years, found to be suffering from BE grade 2 NS +PSC (L>R). She was advised cataract surgery. During the pre-operative examination, it was found that the patient was suffering from severe dry eye and the scheduled surgery was cancelled. She was prescribed teardrops and was advised to re-visit for an evaluation after a month. The patient’s condition did not improve and so she approached Dr Sushma for Ayurvedic management. Based on the previous treatment records and the clinical evaluation, the Biomedical diagnosis was Aqueous Deficient Dry Eye Syndrome and the Ayurvedic diagnosis was Shushkakshi paka- Vata pittaja.
In the category of dosa predominance, it falls under the batana type. In the category of location, Sushkakshi paka falls in the Sarvakshi roga. In the category of treatment, this falls under Ashastrakrutha.
But in this patient, the treating physician has connected it with both vata and kapha vitiation.
- Nidana - Dry eye is caused by vata vitiating nidanas. Later on, pitta vitiating factors also contribute to the disease pathology. There are two types of nidana to be considered. One is the general vata/pitta vitiating factors and vishesha achakshushya nidanas that affects netra avayava specifically.
- Samanya Nidanas - Nidanas which can cause vitiation of vata and pitta are Vegavinigraha or suppression of natural urges.
सर्वरोगनिदानोक्तैरहितैः कुपिता मलाः।
अचक्षुष्यैर्विशेषेण प्रायः पित्तानुसारिणः॥१॥
शिराभिरूर्ध्वं प्रसृता नेत्रावयवमाश्रिताः।
वर्त्म सन्धिं सितं कृष्णं दृष्टिं वा सर्वमक्षि वा॥२॥ (AH.Utt.1.1-2)
- Vishesha Nidana - Amongst these nidanas, those that lead to dry eye are Doorekshanata or looking at distant object for a long time. This results in infrequent blinking, resulting in decreased secretion from meibomian glands. Prolonged visual efforts associated with decreased blink rate such as reading or watching TV, Svapna viparyaya or altered sleep pattern.
- Samprapti - In case of dry eye, as the disease name suggests dryness or rukshata is the basic cause of disease. Nidanas mainly viharas and environmental factors predominantly cause an increase of ruksha guna in netra. This rukshata is responsible for caya of vata. Since tear film also is involved in the nourishment of cornea, is the most external part of netra and is directly exposed to nidanas, vata caya happens over the ocular surface, which is very evident from the reduced quality of components of tear film, which in turn affects the normal movements of lids especially unmeelana in the beginning.
- Lakshana - Dry eye is now recognised as a symptom based disease. Because of the general repeatability of symptoms compared to that of diagnostic tests, dry eye has been considered a symptom-based disease. Information on DED is limited due to lack of uniformity in its definition and the inability of any single diagnostic test or set of diagnostic tests to confirm or rule out the condition. Thus, there has been a shift towards symptom-based assessment as the key component of clinical diagnosis.
The line of treatment mentioned by Sushruta in Uttara tantra for Sushkakshipaka is as follows: Saindhava, Devadaru and Shunthi and the expressed juice of Matulunga, water, breast-milk and clarified butter mixed together and duly prepared should be applied as Anjana. Clarified butter cooked with the drugs of the Jivaniya group and the filling of the cavity of the eye with the same, as well as snuffing with the Anu-taila are also very effective in such cases. Kshalana with cold milk mixed with the admixture of Saindhava or of milk cooked with Rajani and. Deva-daru and mixed with (a little quantity of) Saindhava are efficacious. Sunthi rubbed over a stone-slab with clarified butter and breast-milk is also recommended as an Anjana. The Vasa of aquatic animals or of those which frequent swampy grounds, mixed with a little quantity of powdered Shunthi and Sanidhava should be applied as Anjana in a case of Shushkakshi-paka.
Treatment & rationale for treatment:The classical textbooks of Ayurveda specify this as Ashastrakruta. The rationale of treatment as explained by the treating physician is mentioned below.
Table 1. Medicines/therapies and the rationale of the treatment
Medicines
Rationale
Amritottara Kashaya +
Vaishwanara Churna
Ama Pachana
Snehapana with Indukanta Ghritam
Shodhana
Virechana with Gandharva hastadi Eranda Tailam
Shodhana- pitta vatahara
Drakshadi Kashaya
Vata pitta hara
Gandharva hastadi Eranda Tailam
Vata pitta hara
Sadhyasadhyata: This is specified as Ashastravrutha.
Reference
- Sushruta Samhita. Uttara tantra.
- Caraka Samhita.Ci.26
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Amritottara Kashaya + Vaishwanara Curna Samyoga 15 ml of Kasaya + 1 tsp of curna Oral- with warm water twice daily, before food 2022-10-27 - 2022-11-03 Amritottara Kashaya - Sahasrayoga Kashaya prakarana. ?Vaishwanara Curna - Sahasrayoga Curna prakarana Indukanta Ghritam Ghrtam 25 ml Oral, with warm water on empty stomach 2022-11-17 - 2022-11-19 Sahasrayoga Ghrita prakarana Gandharva hastadi Eranda Tailam Taila 10 ml Oral, with milk on empty stomach 2022-11-22 - 2022-11-22 AS.Ci.15.21 Drakshadi Kashaya Kashayam 20 ml Oral, with 60 ml of warm water morning and evening before food. 2022-11-25 - 2022-12-25 Sahasrayoga Kashaya prakarana Gandharva hastadi Eranda Tailam Taila 10 ml Oral, with milk on empty stomach 2022-11-15 - 2022-12-01 AS.Ci.15.21 Kottamchukkadi Tailam Taila 100 ml Sarvanga Abhyanga 2022-11-21 - 2022-11-21 Sahasrayoga Taila prakarana Anu Tailam Taila 6, 8, 10, 10, 12 drops in order Marsha Nasya 2022-11-26 - 2022-11-30 Sahasrayoga Taila prakarana Elaneer kuzhambu Kuzhambu 2 ml/day As eye salve 2022-12-01 - 2022-12-03 Sahasrayoga Taila prakarana Triphala kashaya Kashayam 200 ml/day For netra kshalana 2022-12-01 - 2022-12-03 Sahasrayoga Kashaya prakarana Anu Tailam Taila 2 drops in each nostril Pratimarsha Nasya 2022-12-05 - 2022-12-08 Sahasrayoga Taila prakarana Triphala-Yasti Kashaya Kashayam 200 ml/day Seka 2023-01-12 - 2023-01-13 Anubhuta Yoga Mukkadi Purambada Vati 1/day Vidalaka 2023-01-12 - 2023-01-13 Ayurvedic Patent & Proprietary Medicine Shatahwadi Ghrita Ghrtam 25 ml/day Tarpana 2023-01-12 - 2023-01-20 AH.Utt.13 Rasna Jambeera Svarasa Svarasa Required Quantity As Talam 2023-01-12 - 2023-01-20 Anubhuta Yoga -
Outcome Measures
OUTCOME MEASURES
In this case report, a 73-year-old moderately built female, a known case of Type II Diabetes Mellitus and hypertension for 8 years, found to be suffering from BE grade 2 NS +PSC (L>R). She was advised cataract surgery. During the pre-operative examination, it was found that the patient was suffering from severe dry eye and the scheduled surgery was cancelled. She was prescribed teardrops and was advised to re-visit for an evaluation after a month. The patient’s condition did not improve and so she approached Dr Sushma for Ayurvedic management. Based on the previous treatment records and the clinical evaluation, the Biomedical diagnosis was Aqueous Deficient Dry Eye Syndrome and the Ayurvedic diagnosis was Shushkakshi paka- Vata pittaja.
Assessment: Both objective and subjective parameters were assessed to analyse the outcome of the ayurvedic treatment.
Subjective parameters: After 2 months- Patient got relief from all the symptoms. And she could undergo the cataract surgery as planned earlier by the Ophthalmologist.
Objective parameters: A complete cataract work up was done, at endpoint, to confirm the eligibility of the patient for surgery. The After 2 months- Patient got relief from symptoms
The Schirmers Test: RE 2mm and LE 3mm at baseline, became RE 5mm and LE 7mm at endpoint.
Image 1. Progress notes and Cataract work up at endpoint dated 22.3.2023.
Image 2. Proof document for cataract surgery dated 21.7.2023
-