Featured Case
-
Abstract
A 38-year-old female patient presented with recurrent episodes of headaches since 3 months which were triggered by loud noise and the honking of vehicles. She also had persistent heaviness on the right side of her head. She consulted an Opthalmologic Surgeon and was diagnosed with Bilateral Papilledema along with idiopathic intracranial hypertension, right is more than left. Despite taking allopathic medication and doing a lumbar puncture, the condition persisted. So she was suggested to undergo brain shunt surgery. The patient refused surgery and opted for Ayurvedic management, and approached Dr Preethi Chhabra. The condition was diagnosed as shiroroga -shirashoola in Ayurveda. The line of treatment followed was Raktamokshana with jalauka as it is pitta and rakta vyadhi hara. Moderate relief in heaviness on the right side of the head was noticed from the first session of Jalaukavacarana. After 3 to 4 sessions of jalaukavacarana, patient had significant relief from all the symptoms. No further episodes of headaches were noticed after 10 sessions of jalaukavacarana. VAS score before treatment was 8 which became 1 after treatment. After treatment, the patient had vision improvement and papilledema resolved. This case report demonstrates the standalone ayurvedic management of papilledema with idiopathic intracranial hypertension, in a patient who did not get relief even after taking allopathic medications and undergoing a lumbar puncture.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 38-year-old female patient presented with recurrent episodes of headaches since 3 months which were triggered by loud noise and the honking of vehicles. She also had persistent heaviness on the right side of her head. She consulted an Opthalmologic Surgeon and was diagnosed with Bilateral Papilledema along with idiopathic intracranial hypertension, right is more than left. Despite taking allopathic medication and doing a lumbar puncture, the condition persisted. So she was suggested to undergo brain shunt surgery. The patient refused surgery and opted for Ayurvedic management, and approached Dr Preethi Chhabra. The condition was diagnosed as shiroroga -shirashoola in Ayurveda. The line of treatment followed was Raktamokshana with jalauka as it is pitta and rakta vyadhi hara. Moderate relief in heaviness on the right side of the head was noticed from the first session of Jalaukavacarana. After 3 to 4 sessions of jalaukavacarana, patient had significant relief from all the symptoms. No further episodes of headaches were noticed after 10 sessions of jalaukavacarana. VAS score before treatment was 8 which became 1 after treatment. After treatment, the patient had vision improvement and papilledema resolved. This case report demonstrates the standalone ayurvedic management of papilledema with idiopathic intracranial hypertension, in a patient who did not get relief even after taking allopathic medications and undergoing a lumbar puncture.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Standalone Ayurvedic management of papilledema with idiopathic intracranial hypertension- a case report
Dr Preethi Chhabra
ABSTRACT
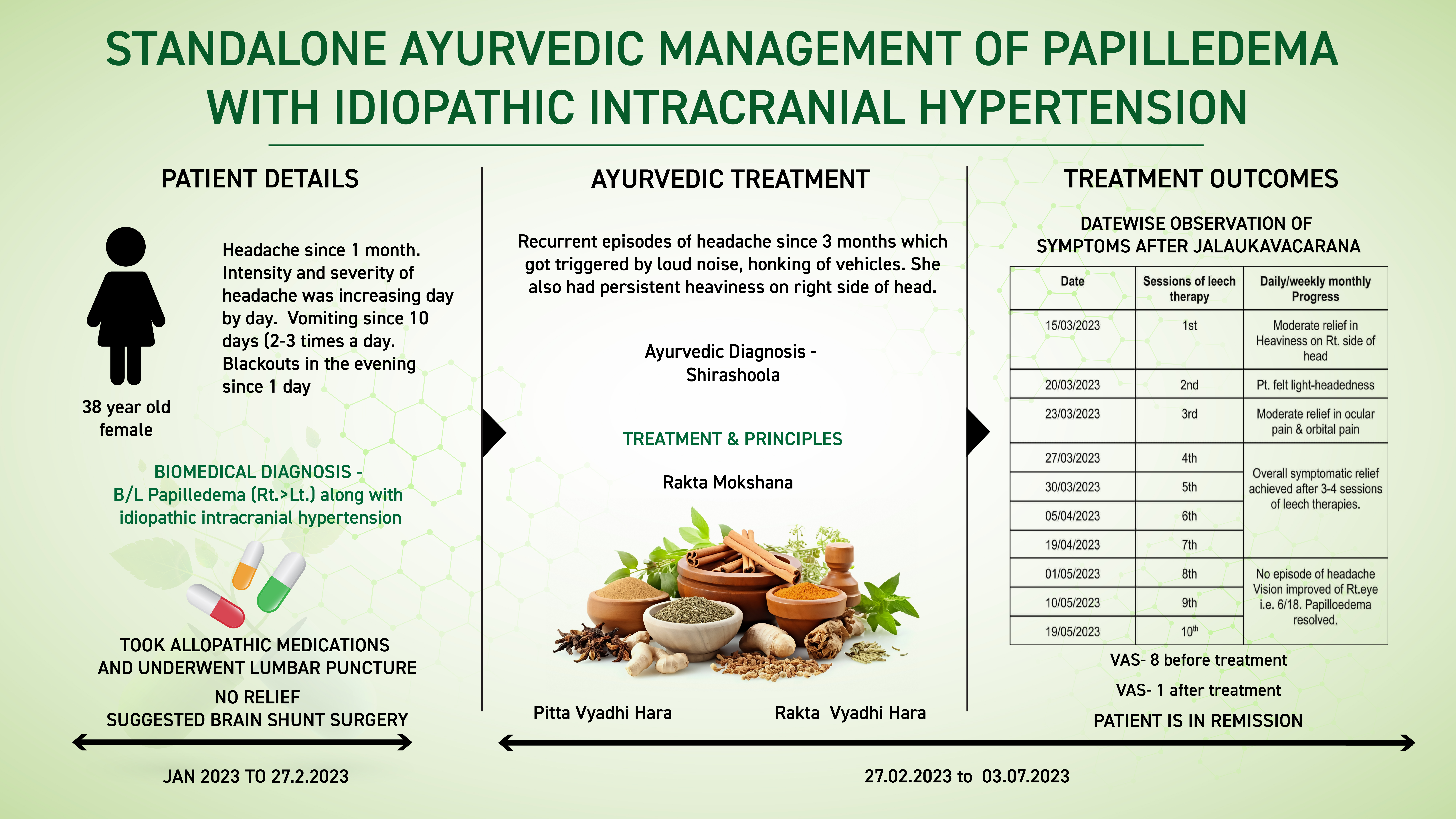
A 38-year-old female patient presented with recurrent episodes of headaches since 3 months which were triggered by loud noise and the honking of vehicles. She also had persistent heaviness on the right side of her head. She consulted an Opthalmologic Surgeon and was diagnosed with B/L Papilledema (Rt.>Lt.) along with idiopathic intracranial hypertension. Despite taking allopathic medication and doing a lumbar puncture, the condition persisted. So she was suggested to undergo brain shunt surgery (in patient's words). The patient refused surgery and opted for Ayurvedic management, and approached Dr Preethi Chhabra. The condition was diagnosed as shirashoola ie..shiroroga in Ayurveda. The line of treatment followed was Raktamokshana with jalauka as it is pitta and rakta vyadhi hara. Moderate relief in heaviness on the right side of the head was noticed from the first session of Jalaukavcharana. After 3-4 sessions of jalaukavacarana, patient had significant relief from all the symptoms. No further episodes of headaches were noticed after 10 sessions of jalaukavacarana. VAS score before treatment was 8 which became 1 after treatment. After treatment, the patient had vision improvement and papilledema resolved. This case report demonstrates the standalone ayurvedic management of papilledema with idiopathic intracranial hypertension, in a patient who did not get relief even after taking allopathic medications and undergoing a lumbar puncture.
KEYWORDS
Shiroroga, shira shoola, papilledema, jalaukavacarana, headache, intracranial hypertension, case report, standalone
INTRODUCTION
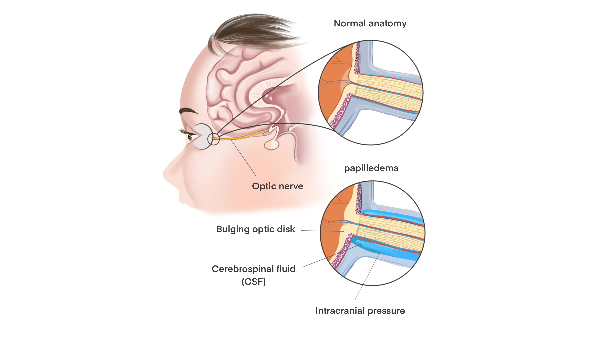
Papilledema is when pressure in your brain makes your optic nerve swell. A mild papilledema with minimal symptoms is usually nothing to worry about. More severe symptoms may indicate a serious underlying condition. However, papilledema can be a sign of an underlying condition or injury that needs to be treated as soon as possible. This is especially true if you notice the symptoms after major trauma to your head.
Causes: The fluid bathing your brain and spinal cord is known as cerebrospinal fluid, or CSF. Optic nerve swelling can happen when CSF builds up where your optic nerve and the central retinal vein travel between your brain and your eye nerve. This area is known as the subarachnoid space. When pressure pushes on the nerve and vein, blood and fluid can’t leave the eye at a normal rate, causing papilledema.
Symptoms:The most common early symptoms of papilledema are brief changes to your vision. These changes may barely be noticeable at first, with blurring, double vision, seeing flashes, or vision loss lasting a few seconds. If brain pressure continues, these changes may last for minutes at a time or longer. In some cases, they may become permanent.
Diagnosis: A full physical examination to check the overall health and clinical evaluation is the primary diagnostic tool. The field of vision will be checked by moving their hands back and forth past the eyes to see where your blind spots are. The ophthalmoscope is used to have a glance at the optic nerve. Additional tests like MRI test or a CT scan of your head to check for tumors or other abnormalities in the brain and skull may be resorted to. Tissue sample (biopsy) of the tumor is removed to test for cancerous cells or drain some of the CSF to test it for any abnormalities.
Treatment: This depends on the cause of the condition. The doctor will prescribe medications to reduce swelling. Corticosteroids, such as prednisone (Deltasone), dexamethasone (Ozurdex), and hydrocortisone (Cortef), can all be used to keep swelling down in your brain. These medications may be injected or taken by mouth. If high blood pressure is causing papilledema, the doctor may prescribe medications to keep the blood pressure under control. If there is a tumor, then brain surgery is done to remove the tumor. If there is an infection, then antibiotics are prescribed. If there is an abscess, a combination of antibiotics and drainage to treat a possible infection as well as to remove the infected pus or fluid from your brain will be adopted.If there is a major head injury, then the target is to reduce pressure and swelling in the head. This may involve draining CSF from head and removing a small piece of the skull to relieve the pressure.
Prognosis: Papilledema isn’t usually an issue on its own. It can typically be treated by draining extra CSF fluid, which reduces swelling. Symptoms then disappear in a few weeks. Swelling or injury to your brain can be serious and life-threatening. If papilledema is caused by an underlying condition, get treated right away to prevent any long-term complications.
PATIENT INFORMATION
In this case report, a 38-year-old female patient presented with recurrent episodes of headaches since 3 months which were triggered by loud noise and the honking of vehicles. She also had persistent heaviness on the right side of her head. She consulted an Opthalmologic Surgeon and was diagnosed with B/L Papilledema (Rt.>Lt.) along with idiopathic intracranial hypertension. Despite taking allopathic medication and doing a lumbar puncture, the condition persisted. So she was suggested to undergo brain shunt surgery (in patient's words). The patient refused surgery and opted for Ayurvedic management, and approached Dr Preethi Chhabra. T
No relevant family/genetic/surgical or psychosocial history.
No Addictions
CLINICAL FINDINGS
Vision Test
IOP
Distant vision - Rt.eye= 6/60 Lt.eye= 6/6
IOP - Rt.eye = 14mmHg Lt.eye = 13 mmHg
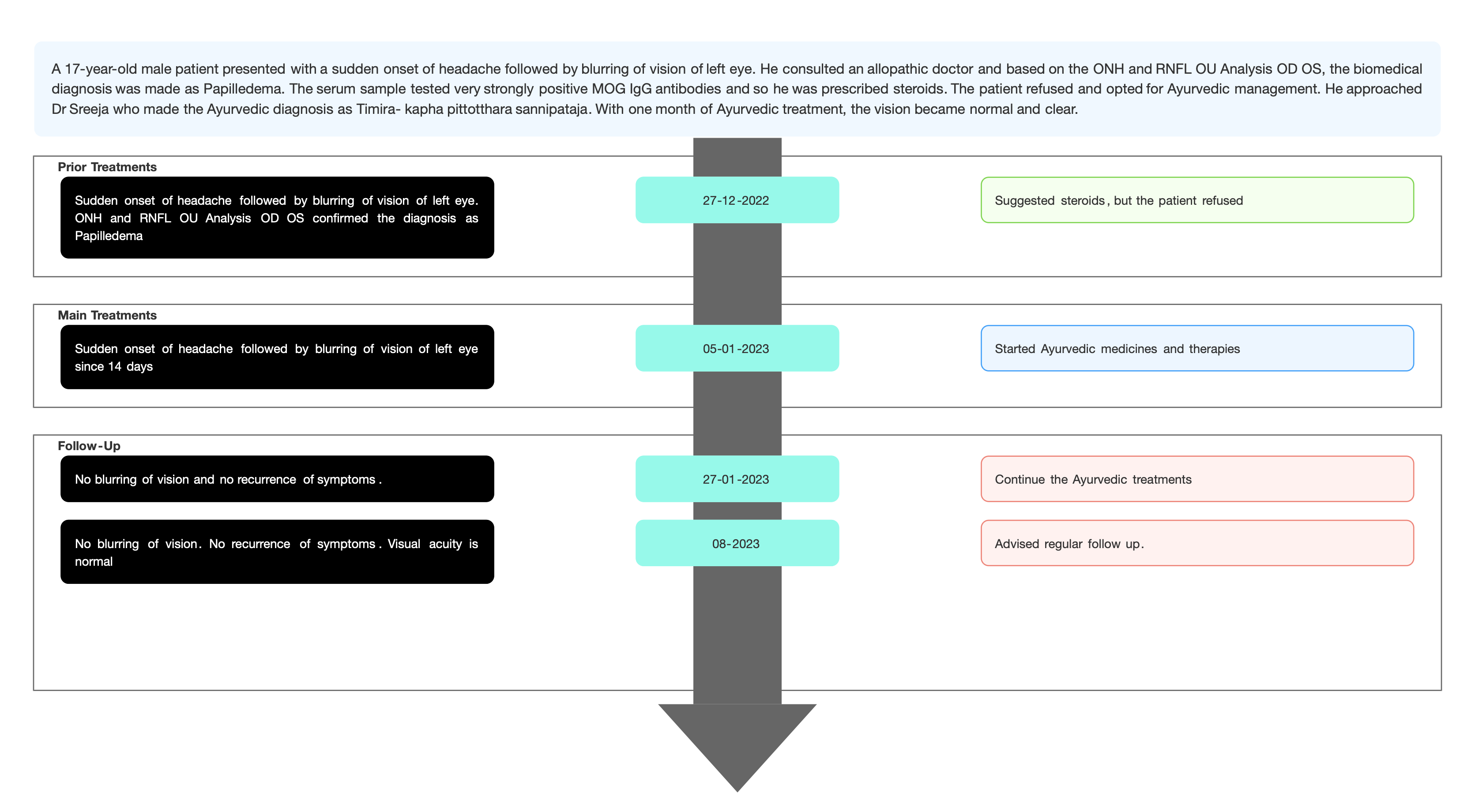
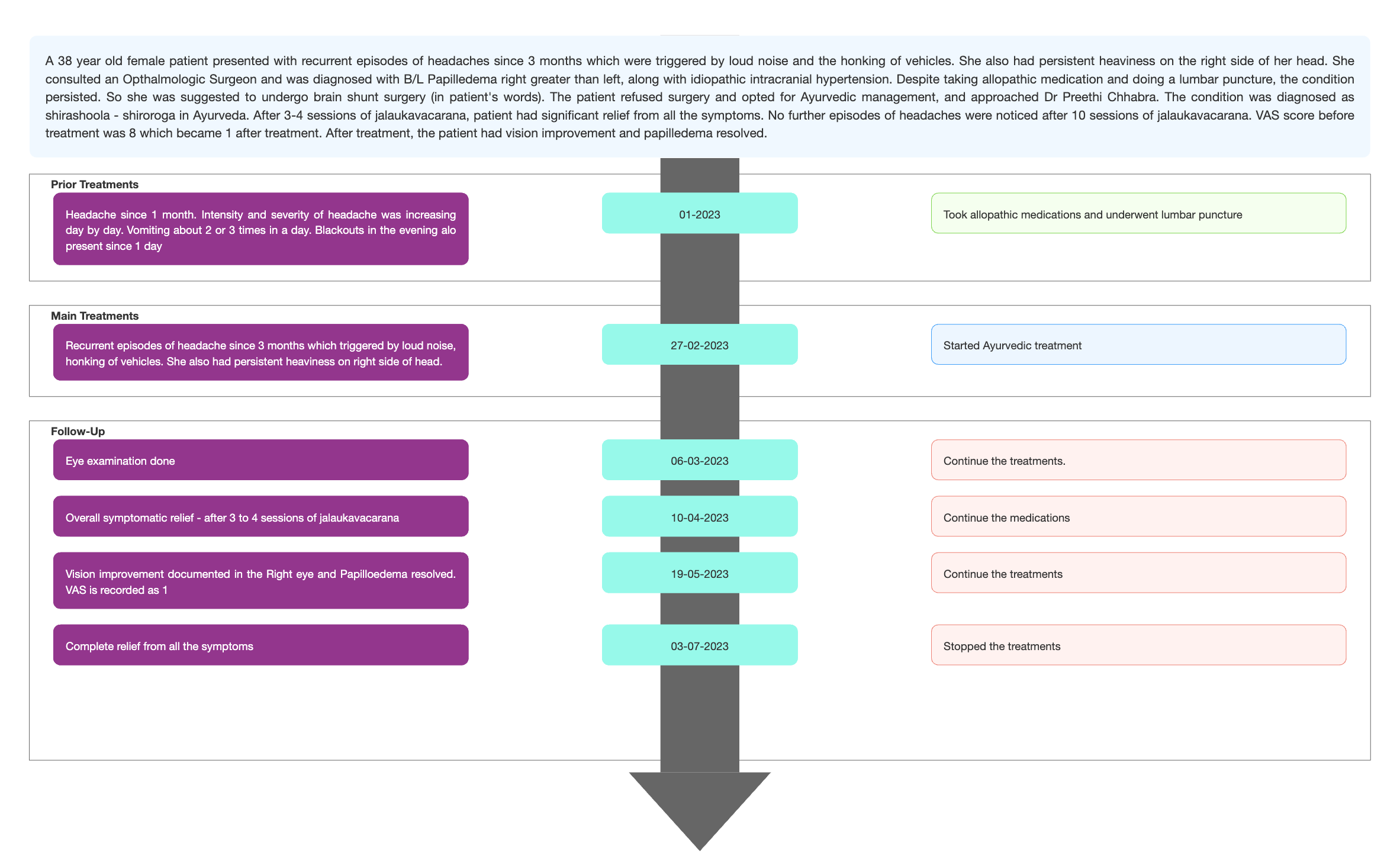
TIMELINE
Image 1. Timeline of events added below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter; Based on the clinical examination and MRI reports, the biomedical diagnosis was made as Bilateral Papilledema- Idiopathic intracranial pressure.
Special Investigations
Fundi disc -
Rt.eye = Severe papilloedema
Lt.eye =Moderate papiloedema
OCT RNFL value = 160
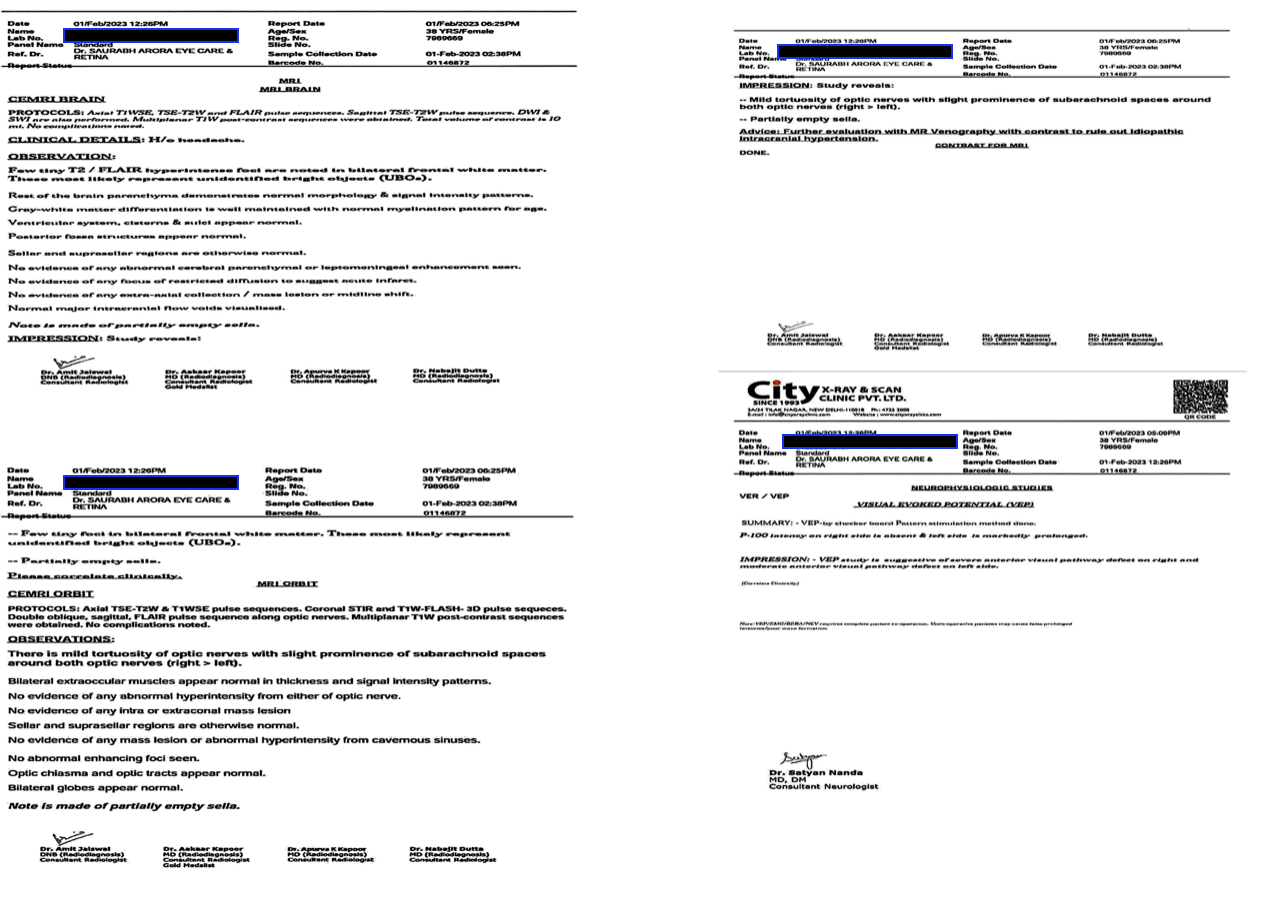
Image 2. Baseline MRI report dated 1.2.2023
Ayurvedic Assessment was done based on the presenting complaints and clinical evaluation. The treating physician confirmed the Ayurvedic diagnosis as Shira shoola/ Shiroroga.
Differential Diagnosis-
- Acute nerve injury
- Benign intracranial hypertension (Pseudotumor cerebri)
- Cerebrovascular ischemia/hemorrhage
- Hydrocephalus
- Intracranial epidural abscess
- Intracranial haemorrhage
Based on previous treatment records and clinical examination, this condition is diagnosed by the treating physician as Papilledema with idiopathic intra-cranial hypertension
Prognosis- Prognosis is highly variable depending on etiology and varies from benign to lethal. If not treated disc edema can cause irreversible optic neuropathy, and loss of color vision. In this case report, raktamokshana was planned as main treatment. After 3-4 sessions of jalaukavacarana, patient had a significant relief from all the symptoms. No further episodes of headaches were noticed after 10 sessions of jalaukavacarana.
THERAPEUTIC INTERVENTION
Refer the tab ‘Treatment’ in the Portal.
FOLLOW-UP AND OUTCOMES
The patient had 5 follow ups in total. Each follow up, the symptoms were assessed and tests were done to analyse the outcome.
Subjective parameters: After one month of Ayurvedic treatment, the vision became clear and normal.
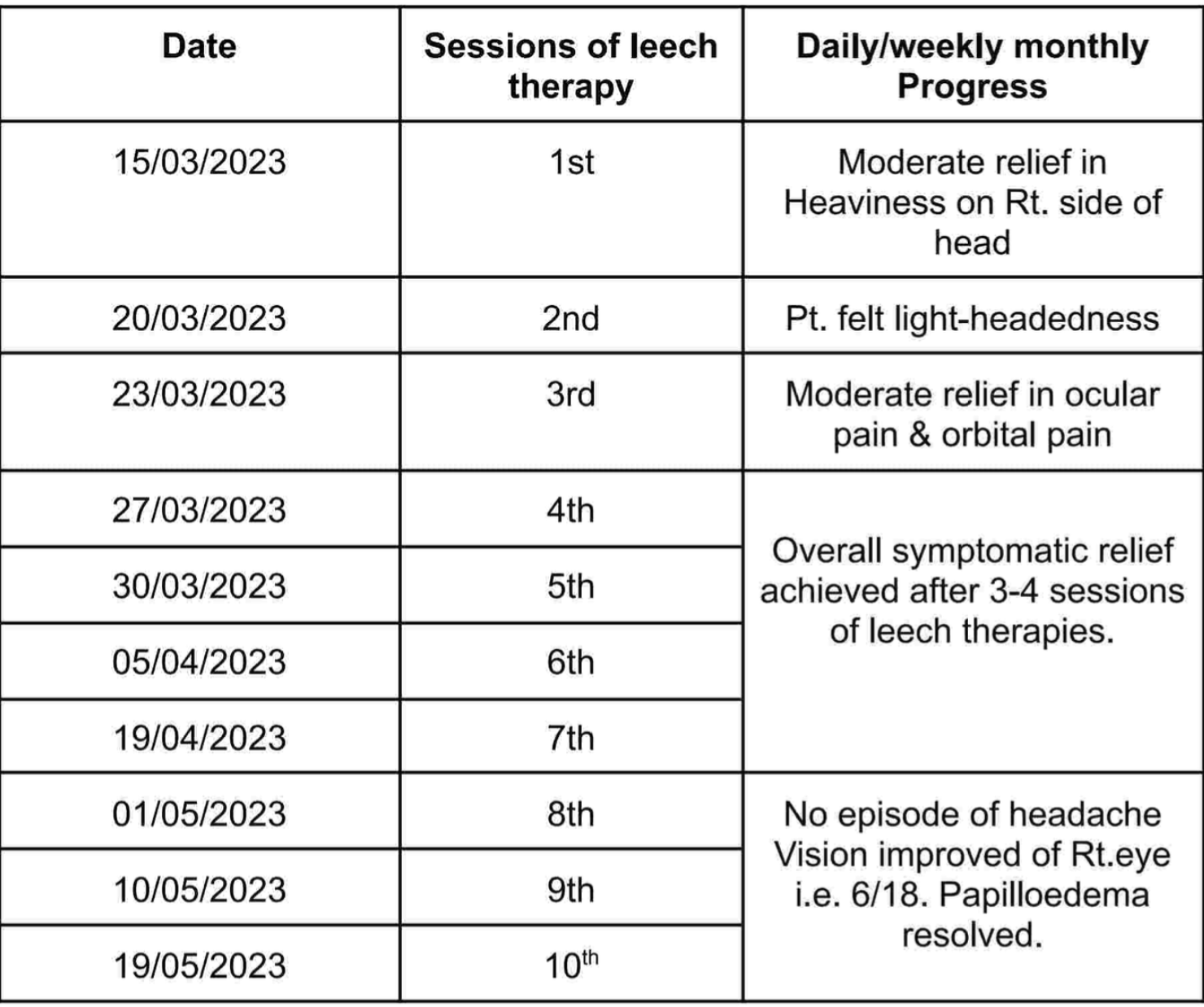
Table 1. Daily/weekly/monthly progress tabulated date wise
Objective parameters: Eye check up was done during follow ups to assess the outcome.
Image 3. Eye check up report during treatment dated 6.3.2023
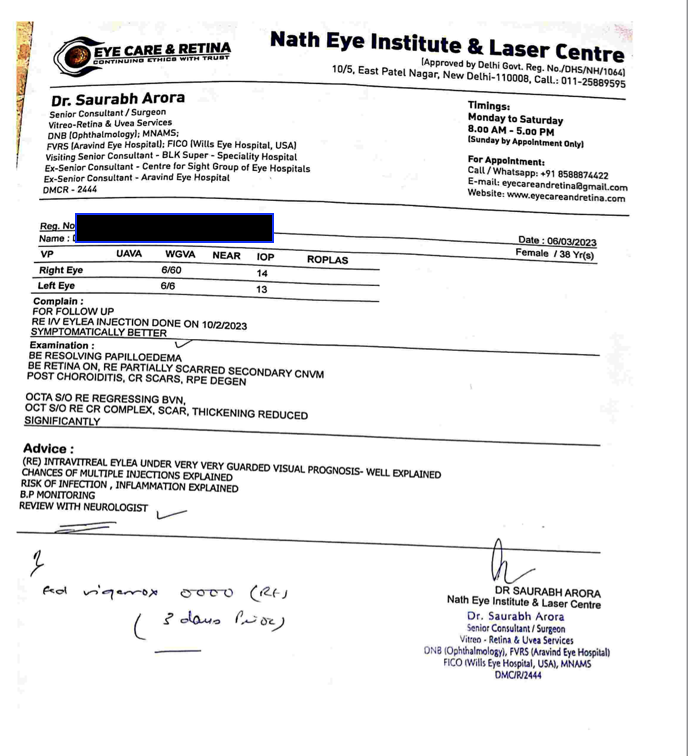
Image 4. Eye check up report during treatment dated 10.4.2023
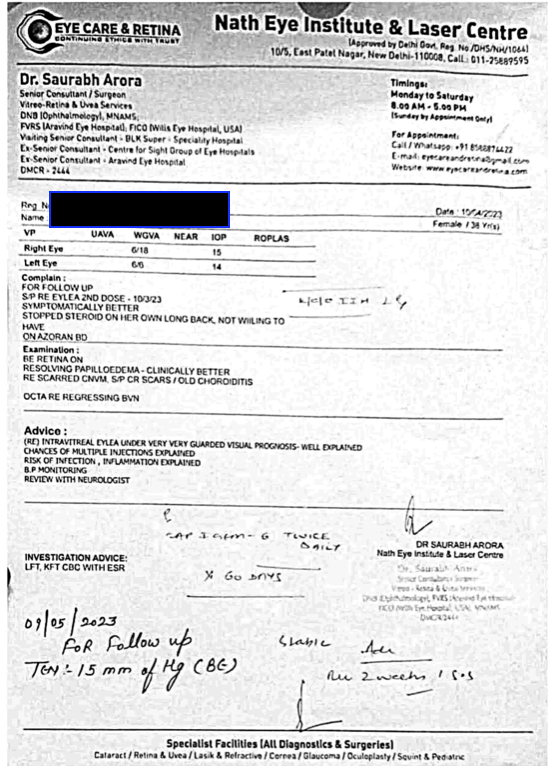
Image 5. Eye tests done 3.7.2023
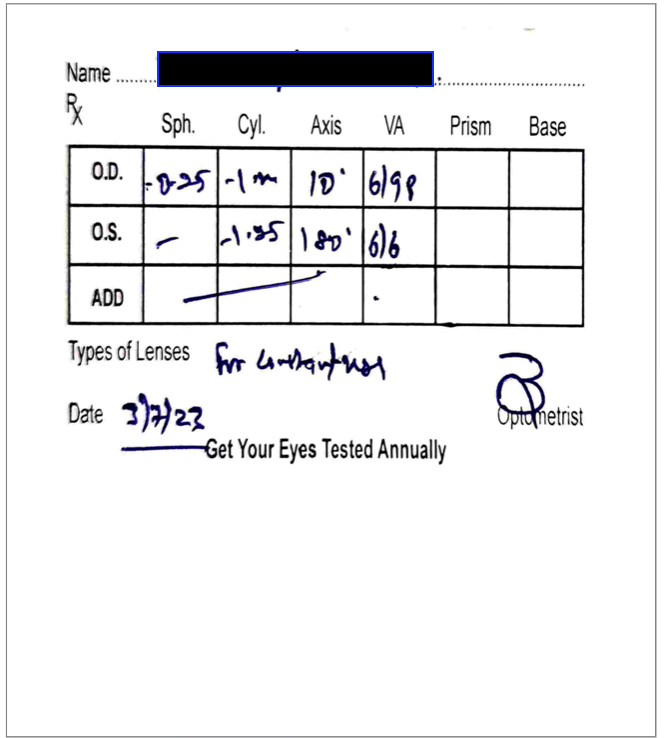
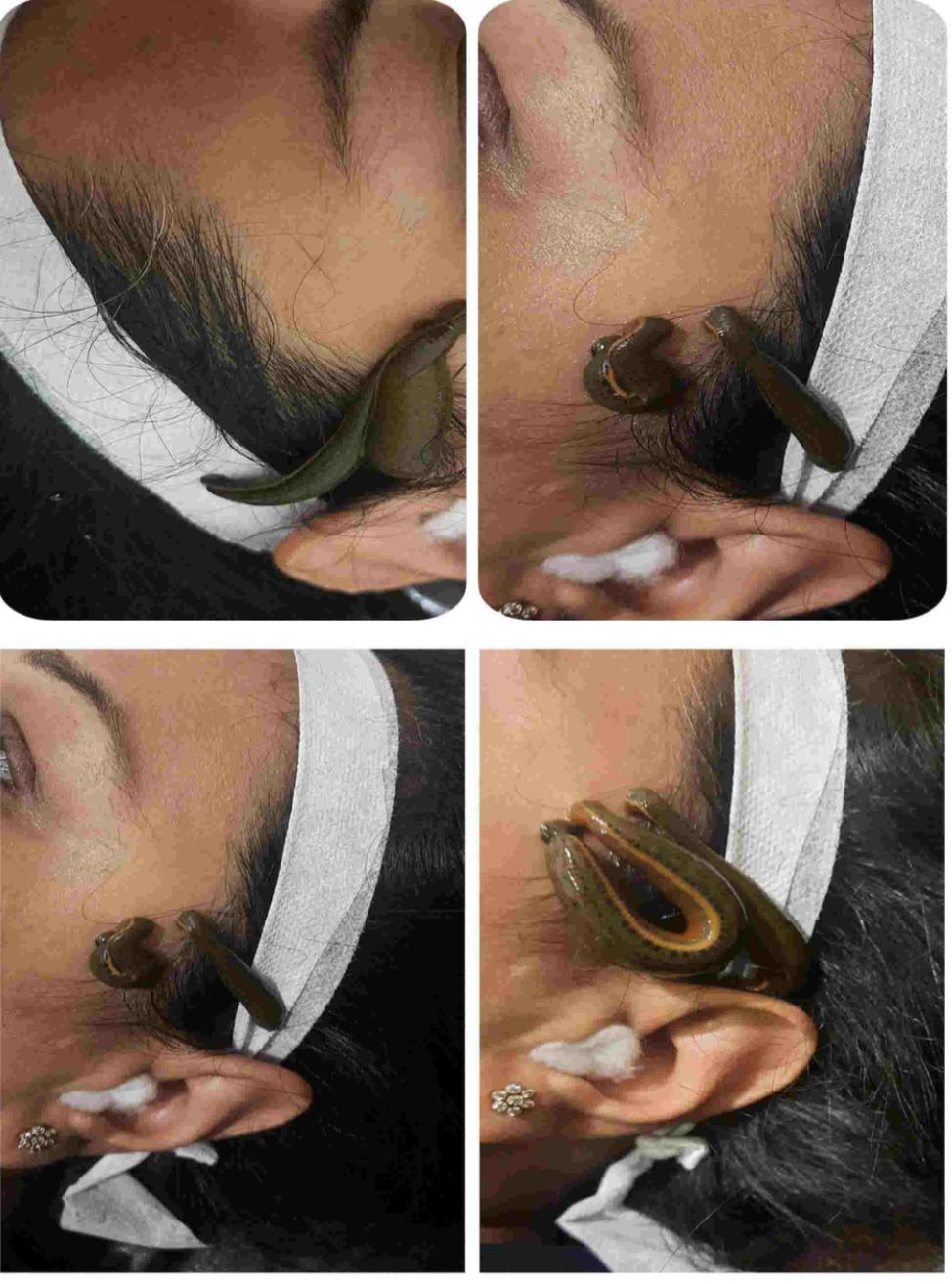
Image 6. Photographs of Jalaukavacarana taken during treatment
Clinician-based assessment; Moderate relief in heaviness on right side of head was noticed from the first session of Jalaukavacarana.After 3-4 sessions of jalaukavacarana, patient had a significant relief from all the symptoms. No further episodes of headaches were noticed after 10 sessions of jalaukavacarana. After treatment, the patient had vision improvement and papilloedema resolved.
Patient-assessed; VAS was recorded as 8 before treatment became 1 after treatment.
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- Subjective and objective parameters were the main assessment tools.
Adverse and unanticipated events; None reported
DISCUSSION:
Papilledema is when pressure in your brain makes your optic nerve swell. A mild papilledema with minimal symptoms is usually nothing to worry about. More severe symptoms may indicate a serious underlying condition. However, papilledema can be a sign of an underlying condition or injury that needs to be treated as soon as possible. This patient was surgery but she was not willing and so opted for Ayurveda. The line of treatment was Raktamokshana, with jalauka as it is pitta vyadhi and rakta vyadhi hara.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE HOME MESSAGES
This case highlights the efficacy of ayurveda in treating Papilledema with idiopathic intra cranial hypertension, in a patient who was suggested surgery and was not willing to undergo surgery.
INFORMED CONSENT
Written consent obtained from patient for publishing of the case report in the Portal
ACKNOWLEDGEMENTS
None
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Bilateral Papilledema- Idiopathic intracranial hypertension
ABOUT THE DISEASE:
Papilledema is when pressure in your brain makes your optic nerve swell. A mild papilledema with minimal symptoms is usually nothing to worry about. More severe symptoms may indicate a serious underlying condition. However, papilledema can be a sign of an underlying condition or injury that needs to be treated as soon as possible. This is especially true if you notice the symptoms after major trauma to your head.
Causes: The fluid bathing your brain and spinal cord is known as cerebrospinal fluid, or CSF. Optic nerve swelling can happen when CSF builds up where your optic nerve and the central retinal vein travel between your brain and your eye nerve. This area is known as the subarachnoid space. When pressure pushes on the nerve and vein, blood and fluid can’t leave the eye at a normal rate, causing papilledema. Brain swelling can be caused by a number of injuries and conditions, including:
traumatic injury to your head
not having enough red blood cells or hemoglobin (anemia)
CSF buildup in your brain (hydrocephalus)
brain bleeding (hemorrhage)
brain inflammation (encephalitis)
brain tissue inflammation (meningitis)
high blood pressure (hypertension)
collection of infected pus in the brain (abscess)
brain tumor
Sometimes, brain pressure builds up for no apparent reason. This is known as idiopathic intracranial hypertension, which is more likely to happen if you’re obese. In this case report, a 38 years female patient presented with recurrent episodes of headaches since 3 months which were triggered by loud noise and the honking of vehicles. She also had persistent heaviness on the right side of her head. She was diagnosed with B/L Papilledema (Rt.>Lt.) along with idiopathic intracranial hypertension. In spite of taking allopathic medication and lumbar puncture, the condition persisted, for which she was suggested to undergo brain shunt surgery (in patient's words). The patient refused surgery and opted for Ayurvedic management. The condition was diagnosed as shirashoola/ shiroroga in Ayurveda and managed with shamana yogas along with Jalaukavacarana.
Symptoms:The most common early symptoms of papilledema are brief changes to your vision. These changes may barely be noticeable at first, with blurring, double vision, seeing flashes, or vision loss lasting a few seconds. If brain pressure continues, these changes may last for minutes at a time or longer. In some cases, they may become permanent. The brain swelling that causes papilledema triggers other symptoms that distinguish it from other eye conditions, including:
feeling nauseous
throwing up
having abnormal headaches
hearing ringing or other noises in your ears (tinnitus)
Diagnosis: A full physical examination to check the overall health and clinical evaluation is the primary diagnostic tool. The field of vision will be checked by moving their hands back and forth past the eyes to see where your blind spots are. The ophthalmoscope is used to have a glance at the optic nerve. Additional tests like MRI test or a CT scan of your head to check for tumors or other abnormalities in the brain and skull may be resorted to. Tissue sample (biopsy) of the tumor is removed to test for cancerous cells or drain some of the CSF to test it for any abnormalities.
Image 1. Baseline MRI report dated 1.2.2023
Treatment: This depends on the cause of the condition. The doctor will prescribe medications to reduce swelling. Corticosteroids, such as prednisone (Deltasone), dexamethasone (Ozurdex), and hydrocortisone (Cortef), can all be used to keep swelling down in your brain. These medications may be injected or taken by mouth. If high blood pressure is causing papilledema, the doctor may prescribe medications to keep the blood pressure under control. Common medications for high blood pressure include:
- Diuretics: bumetanide (Bumex) and chlorothiazide (Diuril)
- Beta blockers: atenolol (Tenormin) and esmilol (Brevibloc)
- ACE inhibitors: captopril and moexipril
If there is a tumor, then brain surgery is done to remove the tumor. If there is an infection, then antibiotics are prescribed. If there is an abscess, a combination of antibiotics and drainage to treat a possible infection as well as to remove the infected pus or fluid from your brain will be adopted.If there is a major head injury, then the target is to reduce pressure and swelling in the head. This may involve draining CSF from head and removing a small piece of the skull to relieve the pressure.
Prognosis: Papilledema isn’t usually an issue on its own. It can typically be treated by draining extra CSF fluid, which reduces swelling. Symptoms then disappear in a few weeks. Swelling or injury to your brain can be serious and life-threatening. If papilledema is caused by an underlying condition, get treated right away to prevent any long-term complications.
Reference
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Shiroroga- Shirashoola
ABOUT THE DISEASE:
In this case report, a 38 years female patient presented with recurrent episodes of headaches since 3 months which were triggered by loud noise and the honking of vehicles. She also had persistent heaviness on the right side of her head. She was diagnosed with B/L Papilledema (Rt.>Lt.) along with idiopathic intracranial hypertension. In spite of taking allopathic medication and lumbar puncture, the condition persisted, for which she was suggested to undergo brain shunt surgery (in patient's words). The patient refused surgery and opted for Ayurvedic management. The condition was diagnosed as shirashoola/ shiroroga in Ayurveda and managed with shamana yogas along with Jalaukavacarana.
The word ‘Shira’ stands for head and ‘Roga’ means disease. The disease pertaining to shira has been specified as ‘Shira shoola’ which means ‘headache’. This is also called as Shiroruk, Shiropida or Shirovedana. It may occur as a symptom of some underlying disease or as a problem in itself. Shirashoola is classified into eight types based upon the cause and the dosha involved.
Causes:
Ahara- Excessive eating, preferring ruksha ahara, liquids - alcohol in excess, food which aggravates dosha altogether and individually are causative factors.
Vihara- Exposure to smoke, frost, breeze, dew, vishamashana, adyashana, ratri jagarana, diva swapna, atapa dhuma sevan, asatmya gandha sevana, exposure to bright and high intensity light, light stimuli, placing pillows in wrong height, aversion to abyanga, indulging in water sport, chinta, krodha, shoka, lamenting, weeping, bhaya, Vega dharana of mutra, mala, kshavatu and nidra, weight lifting, talking too much and too loudly.
Environmental factors
Ayogya upchara - genetic, hereditary, or other diseases
Abhighataja
Types of Shirashoola and their lakshanas:
Ayurveda classifies a headache into the following types:
Vataja: This type of headache occurs due to an imbalance in the vata dosha. It usually causes loss of balance while walking.
Pittaja: It originates in pitta dosha and leads to a burning sensation along with headache.
Kaphaja: It is caused due to kapha and occurs with cold and cough.
Sannipatika: The vitiation of tridoshas causes a sannipatika headache, and it could show symptoms from any or all of the types of headaches mentioned above.
Ananta vata: In this type of headache, pain is felt all over the head with accompanying nausea and giddiness.
Ardhavabhedaka: It involves pain in half of the head.
Samkhaka: In this type of headache, pain is confined to the left and right sides of the head, which swells and become red.
Suryavarta: This type of headache follows the path of the sun – it starts in the morning, increases till midday, and decreases as the sun goes down.
But in this case report, the treating physician has not specified the type of headache.
Treatment & rationale of treatment as specified by the treating physician:
In general the treatments given for Shirashoola are as follows:
Basti karma
Nasya karma
Lepa
Virechana (purgation) karma
Seka
Snehana
Shirodhara
The treating physician explains that the line of treatment adopted is Raktamokshana with Jalauka as it is Pitta vyadhi and Rakta vyadhi hara.
Sadhyasadhyata: The cause of the shirashoola plays an important role in determining the sadhyasadhyata. If the cause can be addressed, then there is curability. But if the cause persists, then the condition is not curable.
Reference:
- Caraka Samhita. Su. 17
- Sushruta Samhita. Utt.25
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Shirahshooladi Vajra Rasa Tablet 1 Oral, thrice daily after food 2023-02-27 - 2023-03-13 Bhaishajya Ratnavali Shirorogadhikara - 140 - 144 Cap. Netramritam Capsule 2 Oral, once daily after food 2023-02-27 - 2023-03-13 Ayurvedic Patent & Proprietary Medicine Prabhakar Mishran Tablet 2 Oral, twice daily after food 2023-02-27 - 2023-03-13 Ayurvedic Patent & Proprietary Medicine Prabhakar Mishran Tablet 2 Oral, twice daily after food 2023-03-20 - 2023-04-03 Ayurvedic Patent & Proprietary Medicine Punarnava arka Arka 20 ml Oral, thrice daily after food 2023-02-27 - 2023-03-13 Ayurveda Sara Sangraha Arka prakarana Punarnava arka Arka 20 ml Oral, thrice daily after food 2023-03-20 - 2023-04-03 Ayurveda Sara Sangraha Arka prakarana Arjuna ksheera paka Ksheera Kalpa 100 ml Oral, thrice daily after food 2023-03-20 - 2023-04-03 Bhaishajya ratnavali.33.11 Brahmi taila Taila Required Quantity For Shiro Abhyanga 2023-02-27 - 2023-03-13 Ayurveda Sara sangraha. Taila prakarana Anutaila Taila 7 drops in each nostril Nasya 2023-02-27 - 2023-03-13 AH.Su.20.37-39 Anutaila Taila 2 drops in each nostril Nasya 2023-04-29 - 2023-05-29 AH.Su.20.37-39 -
Outcome Measures
In this case report, a 38 years female patient presented with recurrent episodes of headaches since 3 months which were triggered by loud noise and the honking of vehicles. She also had persistent heaviness on the right side of her head. She was diagnosed with B/L Papilledema (Rt.>Lt.) along with idiopathic intracranial hypertension. In spite of taking allopathic medication and lumbar puncture, the condition persisted, for which she was suggested to undergo brain shunt surgery (in patient's words). The patient refused surgery and opted for Ayurvedic management. The condition was diagnosed as shirashoola/ shiroroga in Ayurveda and managed with shamana yogas along with Jalaukavacarana.
Assessment: Only Subjective and objective parameters were assessed to analyse the outcome of the treatment.
Subjective parameters: The symptoms were documented after each Jalaukavacarana and tabulated.
Image 1.Daily/weekly/monthly progress tabulated date wise
Objective parameters: VAS was documented as 8 before treatment, became 1 after treatment
Image 2. Photographs of Jalaukavacarana taken during treatment
Eye check up was done during follow ups to assess the outcome.
Image 3. Eye check up report during treatment dated 6.3.2023
Image 4. Eye check up report during treatment dated 10.4.2023
Image 5. Eye tests done 3.7.2023
-