Featured Case
-
Abstract
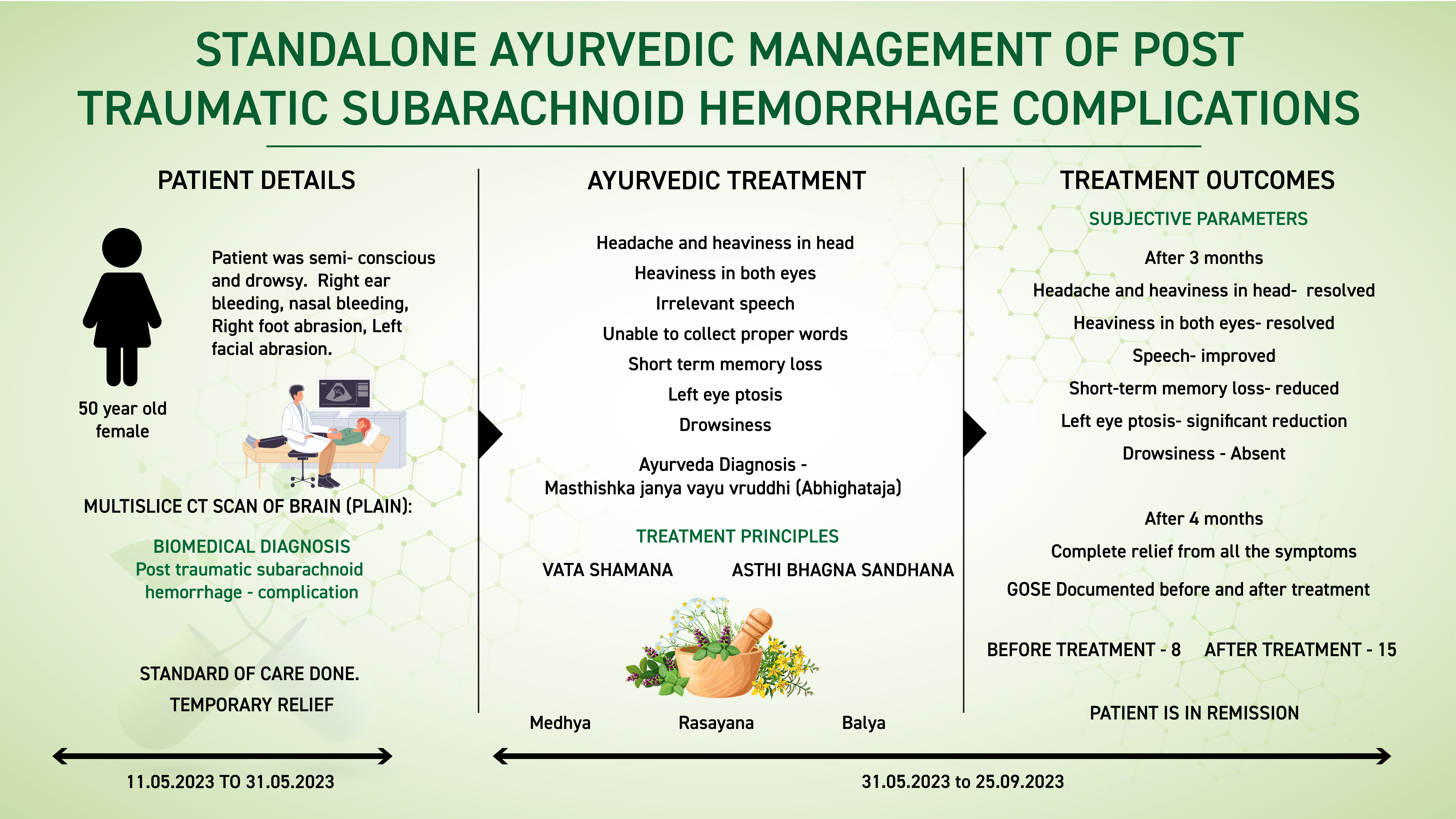
A 50-year-old female patient presented with headache and heaviness in the head, associated with heaviness in both eyes, irrelevant speech, short term memory loss, left eye ptosis and drowsiness for 10 days. She had a history of Road Traffic Accident before 20 days. She was diagnosed with left frontoparietal temporal subarachnoid bleed. The condition resolved with the standard of care, but the patient gradually developed several complications. The patient’s family opted for Ayurvedic treatment and approached Dr Rajnikanth for further management. Based on the Multiple CT Scan of the Brain and clinical examination, the biomedical diagnosis was Post traumatic subarachnoid haemorrhage complications. The Ayurvedic diagnosis was Masthishka janya vayu vruddhi (Abhighataja). The line of treatment followed was to pacify the vata and do the sandhana of asthi bhagna. The medicines chosen were also of balya, medhya and rasayana karma.
After 4 months of Ayurvedic treatment, patient completely recovered from all the symptoms and regain normalcy. This case report demonstrates the standalone successful ayurvedic management of complications caused by Subarachnoid haemorrhage due to a road traffic accident.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 50-year-old female patient presented with headache and heaviness in the head, associated with heaviness in both eyes, irrelevant speech, short term memory loss, left eye ptosis and drowsiness for 10 days. She had a history of Road Traffic Accident before 20 days. She was diagnosed with left frontoparietal temporal subarachnoid bleed. The condition resolved with the standard of care, but the patient gradually developed several complications. The patient’s family opted for Ayurvedic treatment and approached Dr Rajnikanth for further management. Based on the Multiple CT Scan of the Brain and clinical examination, the biomedical diagnosis was Post traumatic subarachnoid haemorrhage complications. The Ayurvedic diagnosis was Masthishka janya vayu vruddhi (Abhighataja). The line of treatment followed was to pacify the vata and do the sandhana of asthi bhagna. The medicines chosen were also of balya, medhya and rasayana karma.
After 4 months of Ayurvedic treatment, patient completely recovered from all the symptoms and regain normalcy. This case report demonstrates the standalone successful ayurvedic management of complications caused by Subarachnoid haemorrhage due to a road traffic accident.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Standalone Ayurvedic management of complications of post traumatic subarachnoid haemorrhage- a case report
Dr Rajnikanth
ABSTRACT
A 50-year-old female patient presented with headache and heaviness in the head, associated with heaviness in both eyes, irrelevant speech, short term memory loss, left eye ptosis and drowsiness for 10 days. She had a history of Road Traffic Accident before 20 days. She was diagnosed with left frontoparietal temporal subarachnoid bleed. The condition resolved with the standard of care, but the patient gradually developed several complications. The patient’s family opted for Ayurvedic treatment and approached Dr Rajnikanth for further management. Based on the Multislice CT Scan of the Brain and clinical examination, the biomedical diagnosis was Post traumatic subarachnoid haemorrhage complications. The Ayurvedic diagnosis was Masthishka janya vayu vruddhi (Abhighataja). The line of treatment followed was to pacify the vata and do the sandhana of asthi bhagna. The medicines chosen were also of balya, medhya and rasayana karma. After 4 months of Ayurvedic treatment, patient completely recovered from all the symptoms and regain normalcy. This case report demonstrates the standalone successful ayurvedic management of complications caused by Subarachnoid haemorrhage due to a road traffic accident.
KEYWORDS
Trauma, subarachnoid hemorrhage, ayurveda, masthishka, abhighataja, case report, vayu vriddhi, standalone
INTRODUCTION
Subarachnoid hemorrhage (SAH) is a frightening and potentially life-threatening condition in which blood leaks from a damaged artery in the brain into the cerebrospinal fluid (CSF). It often results from head trauma or a ruptured aneurysm.
This type of brain bleed can set off a cascade of other problems, which are associated with poor outcomes. To safeguard against these further complications, victims of subarachnoid are monitored in an intensive care unit after they first come into the hospital.
There are four major complications to subarachnoid hemorrhage. Those complications are vasospasm, hydrocephalus, seizures, and re-bleeding.While the four main complications of subarachnoid hemorrhage may seem like more than enough, unfortunately, there are several more potential dangers that come from needing care in an intensive care unit. Deep vein thrombosis of the legs, hyponatremia, and hospital-acquired infections must also be guarded against. Surviving the initial bleed is only part of the challenge of subarachnoid hemorrhage.
Diagnostic criteria: Initial evaluation of a patient suspected of having a subarachnoid haemorrhage should include a head computed tomogram (CT). A CT angiography should be performed if an aSAH is identified to determine the location and size of the aneurysm. However, if the initial Head CT is negative, a lumbar puncture is performed in case of strong suspicion. A lumbar puncture should ideally be performed 6 hours after the initial Head CT to detect the presence of xanthochromia. Often xanthochromia can be assessed at the bedside due to visible cerebrospinal fluid color change. A CT angiogram helps confirm and identify an intracerebral aneurysm's location. If the CT angiogram is negative, it should be followed by cerebral angiography or digital subtraction angiography (DSA).[32] A few factors should be considered in patients allergic to contrast or who have decreased renal function. These patient populations need pre-procedure treatment to decrease the risk of an adverse reaction. Time-of-flight magnetic resonance angiography (TOF-MRA) is another acceptable mode of imaging that does not require contrast injection.
The sensitivity of CT scans and red blood cell (RBC) counts are time-dependent and very sensitive early in the diagnosis. This loss of sensitivity over time can be due to the brisk physiologic flow of cerebrospinal fluid (CSF). Over time, the RBCs present in the CSF undergo lysis resulting in breakdown products such as bilirubin and oxyhemoglobin. RBC lysis explains that xanthochromia becomes increasingly sensitive after a few hours.
Treatment & Prognosis: All Patients presenting with SAH should be organised according to the severity of disease. In general, management include medical measures and interventional options like endovascular coiling or direct surgical clipping of the IA. Patients are typically treated with both medical and interventional options. More conservative or less invasive interventions may be sufficient for patients with grade I or II SAH. The key goals for all SAH patients are the prevention of re-bleeding, delayed cerebral ischemia (DCI), supportive care, pain management, and accurate diagnosis and treatment.
PATIENT INFORMATION
In this case report, a 50-year-old female patient presented with headache and heaviness in the head, associated with heaviness in both eyes, irrelevant speech, short term memory loss, left eye ptosis and drowsiness for 10 days. She had a history of Road Traffic Accident before 20 days. She was diagnosed with left frontoparietal temporal subarachnoid bleed. The condition resolved with the standard of care, but the patient gradually developed several complications. The patient’s family opted for Ayurvedic treatment and approached Dr Rajnikanth for further management. Based on the Multislice CT Scan of the Brain and clinical examination, the biomedical diagnosis was Post traumatic subarachnoid haemorrhage complications.
No relevant family, genetic, psychosocial or surgical history
CLINICAL FINDINGS
General examinations were done.
Clinical Findings- Patient was not able to coordinate with question, not able to recall memories, unable to speak clearly, unable to walk.
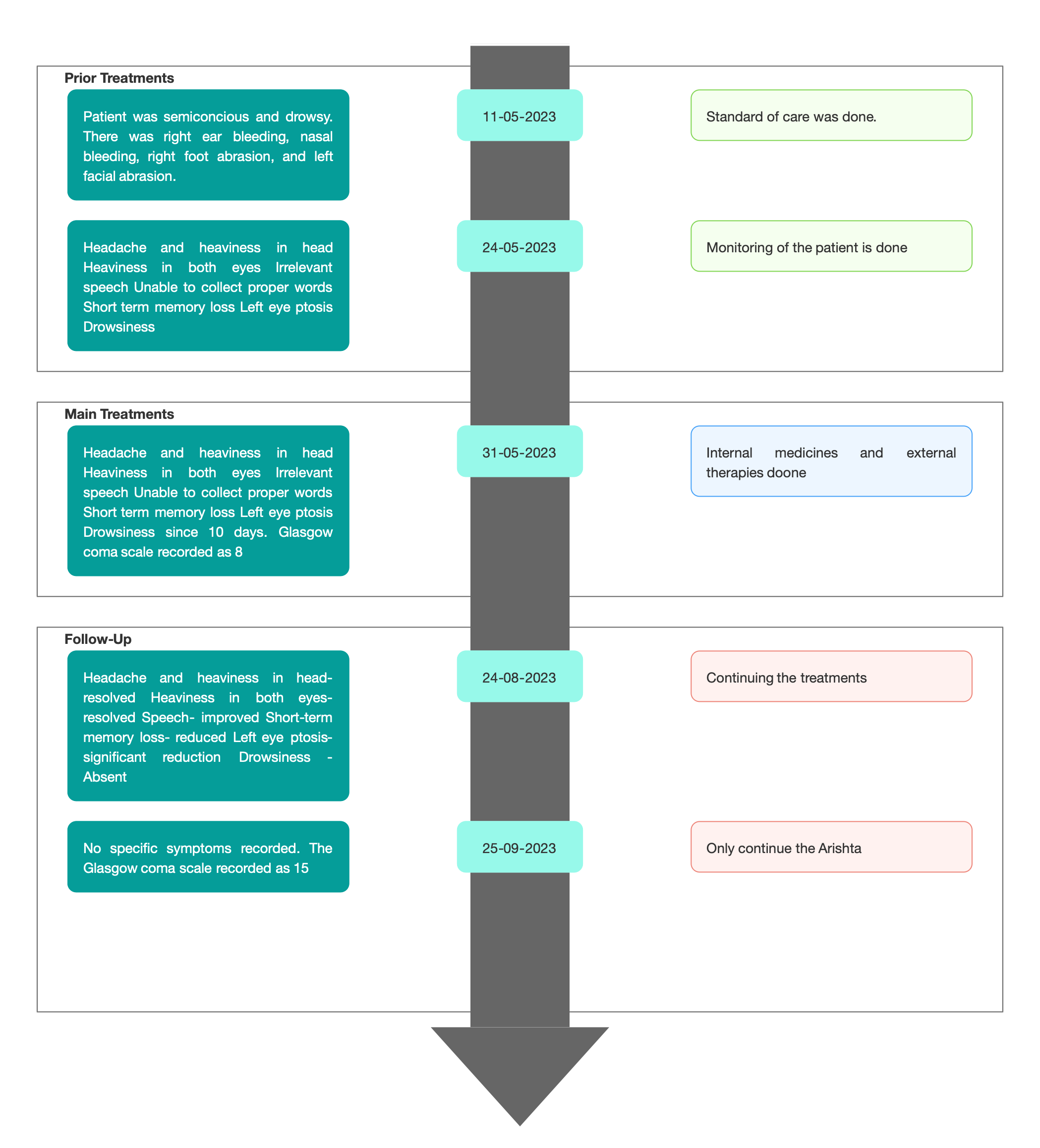
TIMELINE
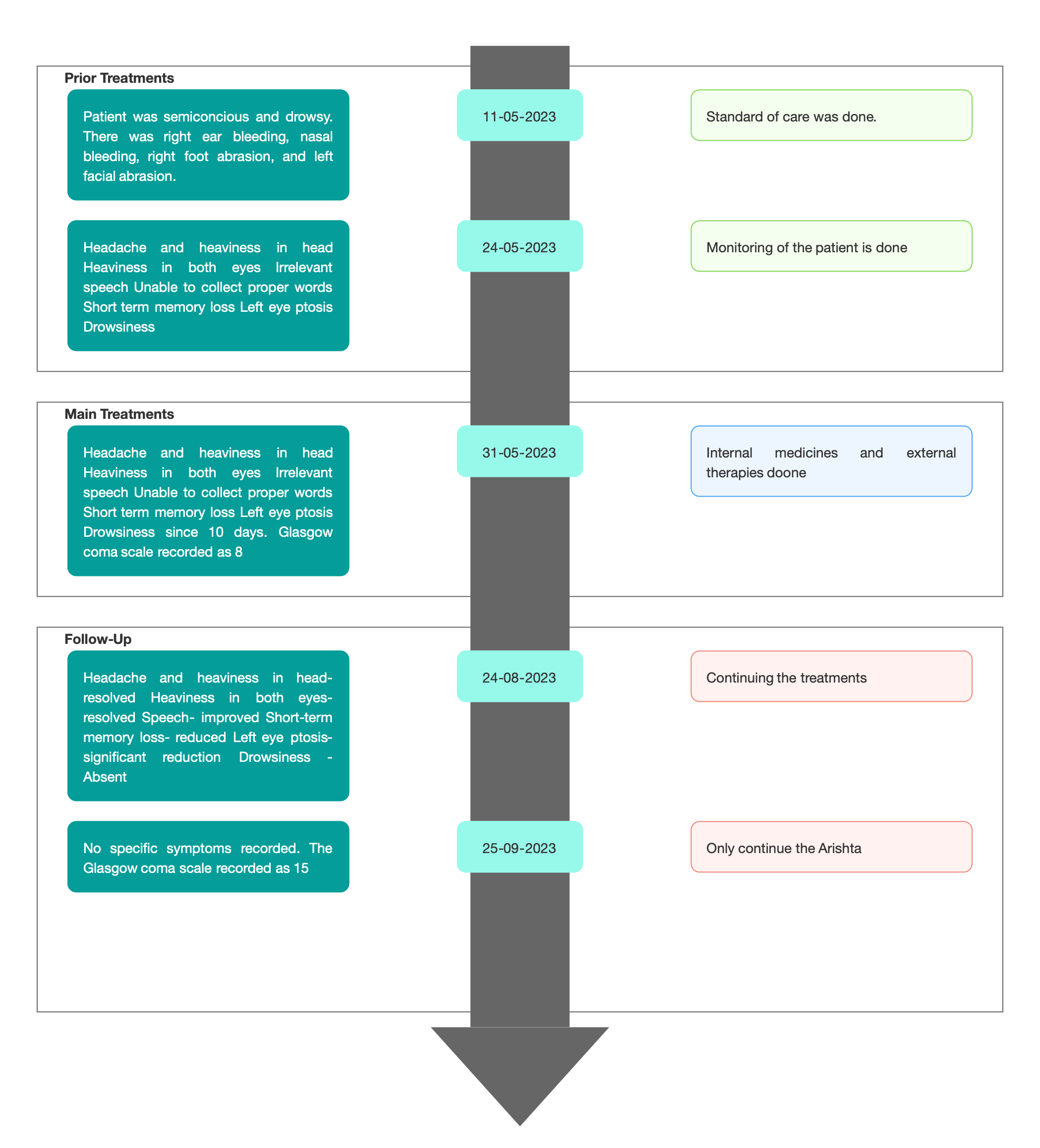
Image 1. Timeline of events added below
DIAGNOSTIC ASSESSMENT
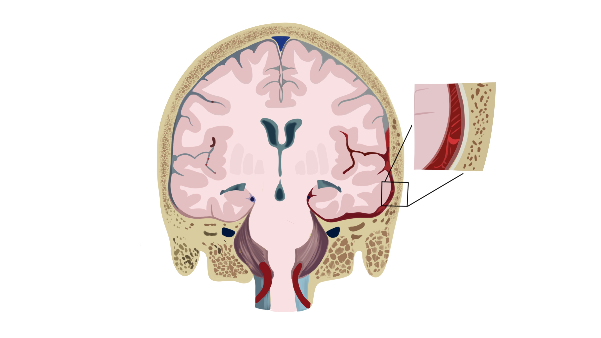
Modern Diagnostic parameter; Based on the clinical evaluation and the of Brain,, the treating physician confirmed the biomedical diagnosis as Post Traumatic Subarachnoid Haemorrhage complications.
Image 2. Multislice CT Scan of Brain dated 11.5.2023
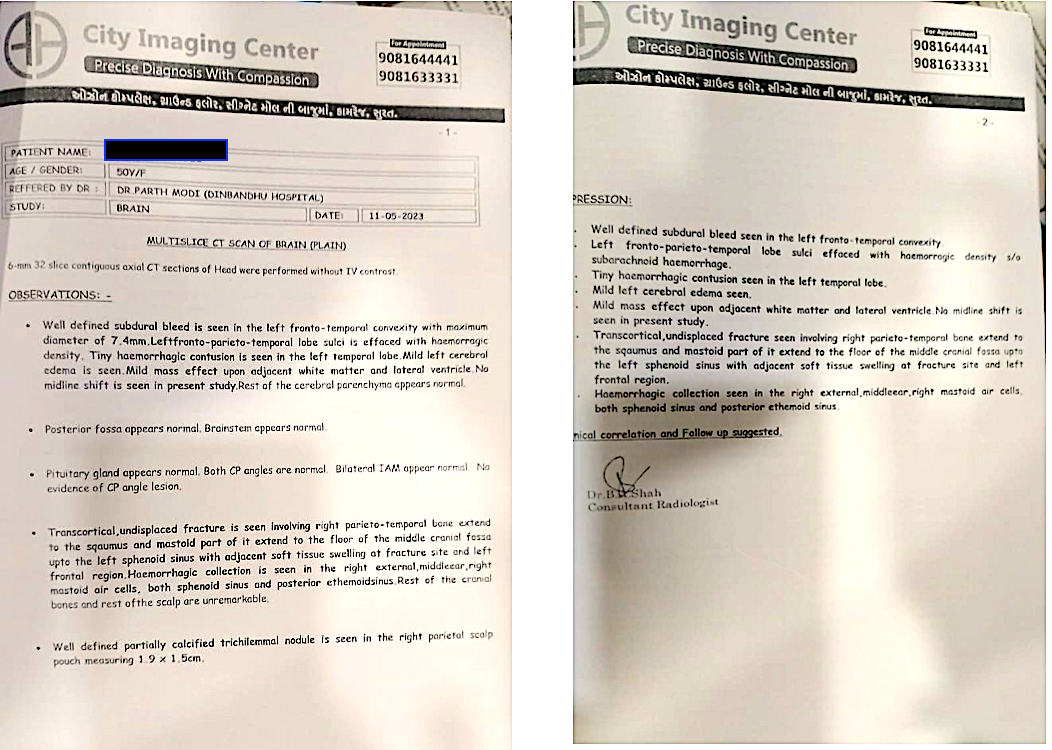
Image 3. Multislice CT Scan of Brain dated 24.5.2023
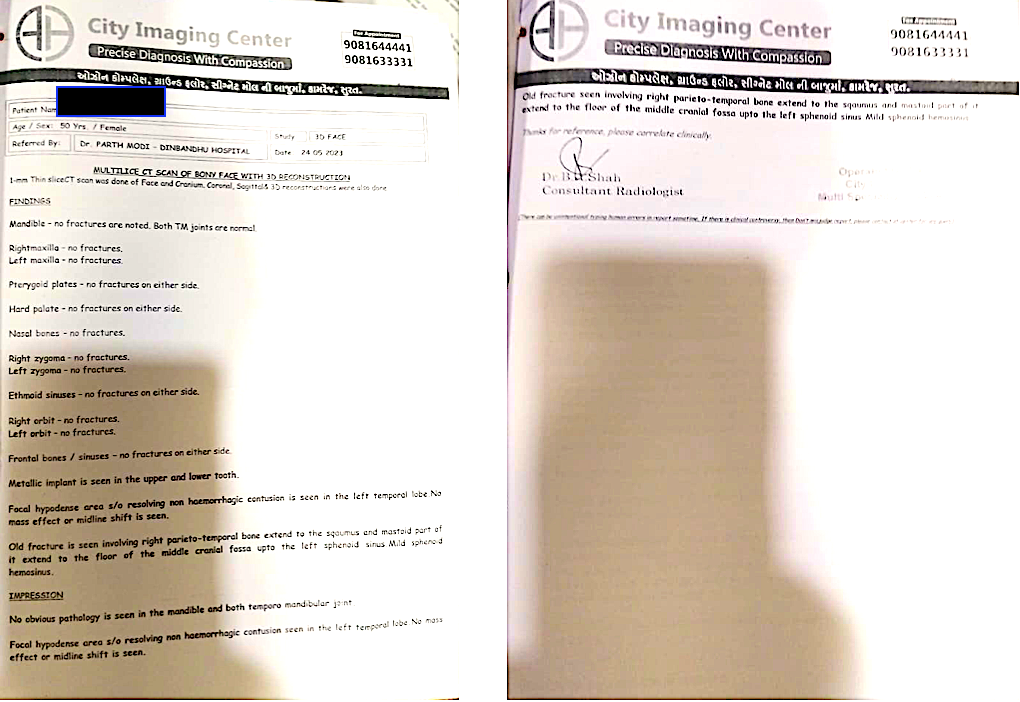
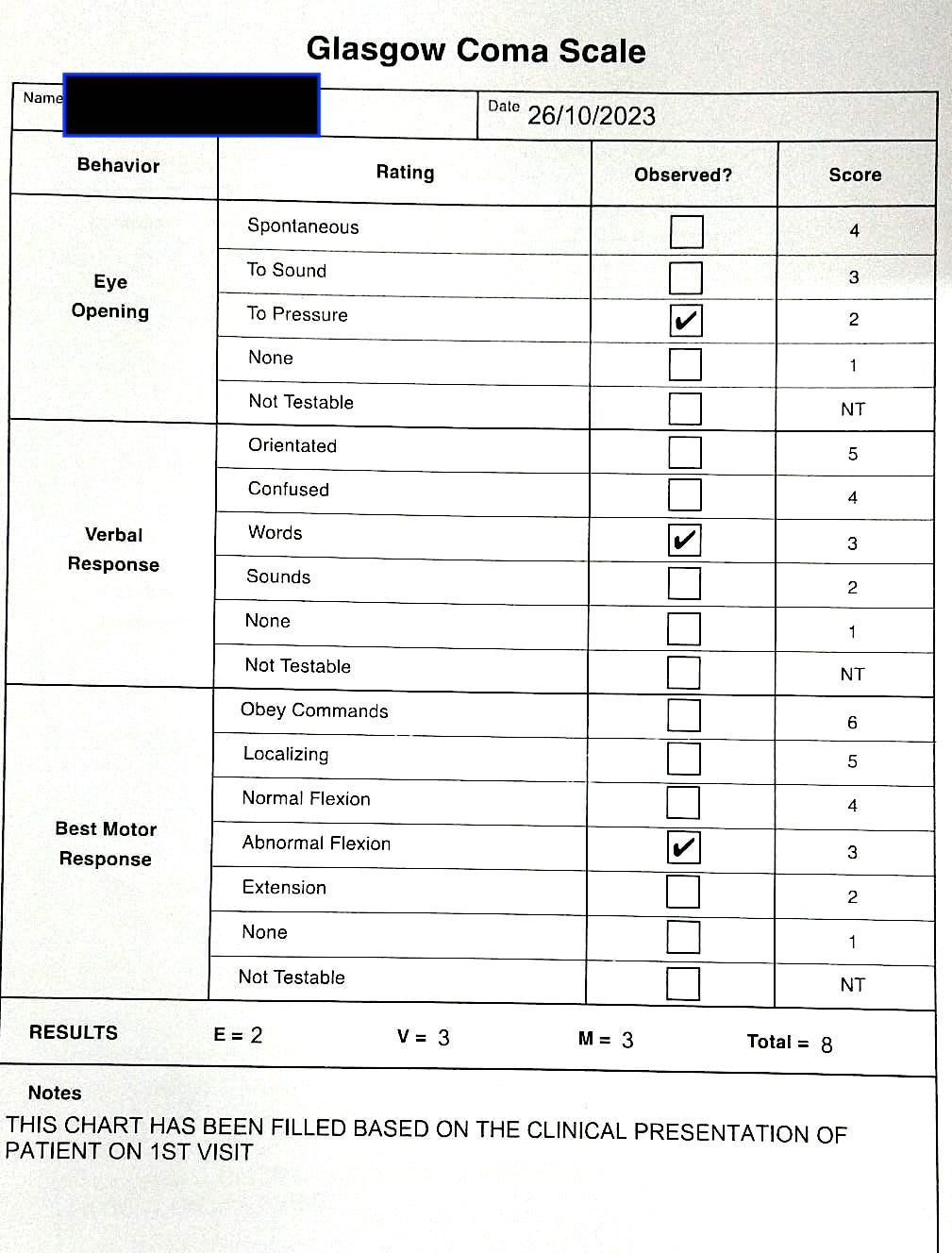
Image 4. Glasgow Coma Scale assessed at baseline
Ayurvedic Assessment was done based on the presenting complaints, clinical evaluation and the Multislice CT Scan of the Brain.
Differential Diagnosis-
Subdural hemorrhage, meningitis, encephalitis, brain tumor, hemorrhagic stroke, neurosyphilis, migraine, hypertensive encephalopathy, wernicke's encephalopathy. Based on previous treatment records and clinical examination, in this case report, the treating physician diagnosed the condition as Post traumatic subarachnoid haemorrhage complications.
Prognosis & Treatment available: Recovery and prognosis are highly variable and largely dependent on the severity of the initial SAH. In general, one-third of patients who suffer a SAH will survive with good recovery, one-third will survive with a disability or stroke and one-third will die. SAH patients may suffer short-term and/or long-term deficits as a result of the bleed or the treatment. In this case report, the patient is diagnosed with post traumatic subarachnoid haemorrhage. The condition resolved with the standard of care, but the patient gradually developed headache and heaviness in the head, associated with heaviness in both eyes, irrelevant speech, short-term memory loss, left eye ptosis and drowsiness. With 4 months of Ayurvedic treatments, patient completely recovered from all the symptoms and regained normalcy.
THERAPEUTIC INTERVENTION
Please refer the tab ‘Treatment’ in the Portal.
FOLLOW-UP AND OUTCOMES
Both objective and subjective parameters were assessed to analyse the outcome of the ayurvedic treatment.
Subjective parameters: The symptoms were assessed through out the treatment.
- After 3 months of treatment, headache and heaviness in head- resolved, heaviness in both eyes- resolved, speech- improved and short-term memory loss- reduced.
- After 4 months of treatment, the patient got complete relief from symptoms.
Objective Parameters:
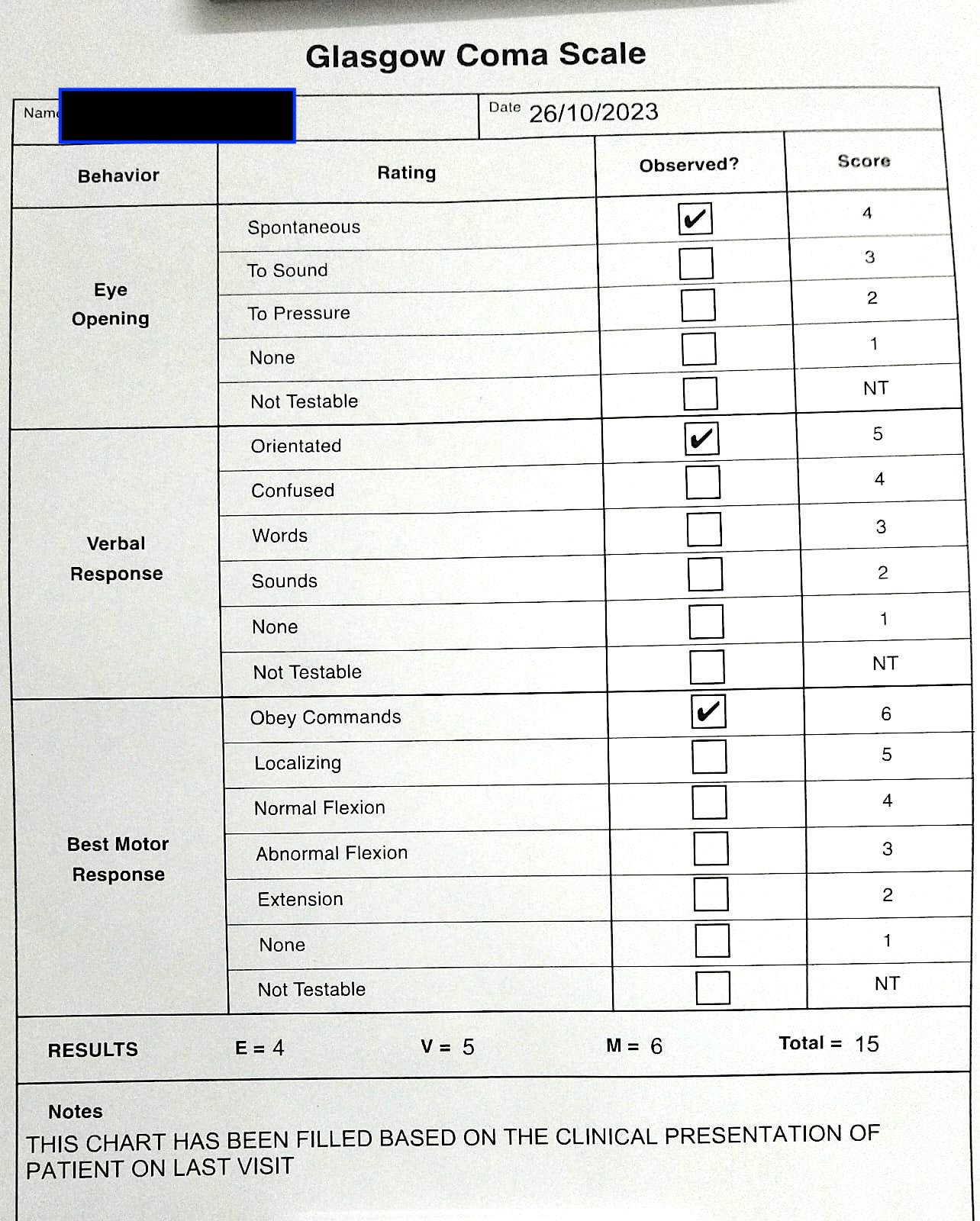
Glasgow Coma scale was documented at baseline and endpoint to assess the outcome of the ayurvedic treatment. Glasgow Coma Scale was recored as 8 at baseline that improved to 15 at endpoint, indicating the improvement in the quality of life and the relief from the symptoms.
Image 5. Glasgow Coma scale documented at endpoint filled by the Physician on the mentioned date.
Clinician-based assessment; With 3 months of Ayurvedic treatment, headache and heaviness in head resolved, heaviness in both eyes resolved, speech improved, memory improved.There was significant reduction in left eye ptosis and drowsiness. After 4 months of treatment, patient completely recovered from all the symptoms and regained normalcy. Improvement in patient status was assessed using Glasgow Coma scale at endpoint.
Patient-assessed; Not relevant.
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported
DISCUSSION ;
The patient had a history of road traffic accident, and there was a left fronto parietal temporal subarachnoid bleed. This was resolved with the standard of care, but then she developed complications. The physician diagnosed this condition as Mastishka janya vayu vruddhi (Abhighataja) and the line of treatment followed was to pacify the vata and do the sandhana of asthi bhagna. The medicines chosen were also of balya, medhya and rasayana karma.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE HOME MESSAGES
This case highlights the effectiveness of Ayurveda in managing complications arising from Post-traumatic subarachnoid haemorrhage. It demonstrates Ayurveda's potential to achieve favourable outcomes through timely intervention. Remarkably, after four months of treatment, the patient made a full recovery, regaining normalcy and relief from all the symptoms.
INFORMED CONSENT
Written consent obtained from patient for publishing of the case report in the Portal
ACKNOWLEDGEMENTS
None specified
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
1. https://www.verywellhealth.com/complications-of-subarachnoid-hemorrhage-2488897
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Post traumatic Subarachnoid haemorrhage (SAH) complications
About The Disease:
Subarachnoid hemorrhage (SAH) is a frightening and potentially life-threatening condition in which blood leaks from a damaged artery in the brain into the cerebrospinal fluid (CSF). It often results from head trauma or a ruptured aneurysm.
This type of brain bleed can set off a cascade of other problems, which are associated with poor outcomes. To safeguard against these further complications, victims of subarachnoid are monitored in an intensive care unit after they first come into the hospital.
There are four major complications to subarachnoid hemorrhage. Those complications are vasospasm, hydrocephalus, seizures, and re-bleeding.While the four main complications of subarachnoid hemorrhage may seem like more than enough, unfortunately, there are several more potential dangers that come from needing care in an intensive care unit. Deep vein thrombosis of the legs, hyponatremia, and hospital-acquired infections must also be guarded against. Surviving the initial bleed is only part of the challenge of subarachnoid hemorrhage.
Diagnostic criteria: Initial evaluation of a patient suspected of having a subarachnoid haemorrhage should include a head computed tomogram (CT). A CT angiography should be performed if an aSAH is identified to determine the location and size of the aneurysm. However, if the initial Head CT is negative, a lumbar puncture is performed in case of strong suspicion. A lumbar puncture should ideally be performed 6 hours after the initial Head CT to detect the presence of xanthochromia. Often xanthochromia can be assessed at the bedside due to visible cerebrospinal fluid color change. A CT angiogram helps confirm and identify an intracerebral aneurysm's location. If the CT angiogram is negative, it should be followed by cerebral angiography or digital subtraction angiography (DSA).[32] A few factors should be considered in patients allergic to contrast or who have decreased renal function. These patient populations need pre-procedure treatment to decrease the risk of an adverse reaction. Time-of-flight magnetic resonance angiography (TOF-MRA) is another acceptable mode of imaging that does not require contrast injection.
The sensitivity of CT scans and red blood cell (RBC) counts are time-dependent and very sensitive early in the diagnosis. This loss of sensitivity over time can be due to the brisk physiologic flow of cerebrospinal fluid (CSF). Over time, the RBCs present in the CSF undergo lysis resulting in breakdown products such as bilirubin and oxyhemoglobin. RBC lysis explains that xanthochromia becomes increasingly sensitive after a few hours.
In this case report, a 50-year-old female patient presented with headache and heaviness in the head, associated with heaviness in both eyes, irrelevant speech, short term memory loss, left eye ptosis and drowsiness for 10 days. She had a history of Road Traffic Accident before 20 days. She was diagnosed with left frontoparietal temporal subarachnoid bleed. The condition resolved with the standard of care, but the patient gradually developed several complications. The patient’s family opted for Ayurvedic treatment and approached Dr Rajnikanth for further management. Based on the Multislice CT Scan of the Brain and clinical examination, the biomedical diagnosis was Post traumatic subarachnoid haemorrhage complications. The Ayurvedic diagnosis was Masthishka janya vayu vruddhi (Abhighataja).
Treatment & Prognosis: All Patients presenting with SAH should be organised according to the severity of disease. In general, management include medical measures and interventional options like endovascular coiling or direct surgical clipping of the IA. Patients are typically treated with both medical and interventional options. More conservative or less invasive interventions may be sufficient for patients with grade I or II SAH. The key goals for all SAH patients are the prevention of re-bleeding, delayed cerebral ischemia (DCI), supportive care, pain management, and accurate diagnosis and treatment.
Image 1. Multislice CT Scan of Brain dated 11.5.2023
Image 2. Multislice CT Scan of Brain dated 24.5.2023
Image 3. Glasgow Coma Scale assessed at baseline
Reference
- https://www.verywellhealth.com/complications-of-subarachnoid-hemorrhage-2488897
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Mastishka janya vayu vruddhi (Abhighataja).
ABOUT THE DISEASE:
The biomedical diagnosis of Subarachnoid haemorrhage complication has been correlated to Mastishka janya vayu vriddhi (Abhigataja). Subarachnoid haemorrhage complications cannot be directly correlated to any disease in the classical textbooks of Ayurveda.
In this case report, a 50-year-old female patient presented with headache and heaviness in the head, associated with heaviness in both eyes, irrelevant speech, short term memory loss, left eye ptosis and drowsiness for 10 days. She had a history of Road Traffic Accident before 20 days. She was diagnosed with left frontoparietal temporal subarachnoid bleed. The condition resolved with the standard of care, but the patient gradually developed several complications. The patient’s family opted for Ayurvedic treatment and approached Dr Rajnikanth for further management. Based on the Multislice CT Scan of the Brain and clinical examination, the biomedical diagnosis was Post traumatic subarachnoid haemorrhage complications. The Ayurvedic diagnosis was Masthishka janya vayu vruddhi (Abhighataja).
Here the patient has a history of road traffic accident, that was a cause for the condition. Hence the reason has been mentioned as ‘Abhighataja’. The sthana samshraya of the vyadhi is mastishka. And the dosa is the aggravated vata.
वातवृद्धौ वाक्पारुष्यं कार्श्यं कार्ष्ण्यं गात्रस्फुरणमुष्णकामि(म)ता निद्रानाशोऽअल्पबलत्वं गाढवर्चस्त्वं च; (SS.Su.15.13)
Sushruta mentions that when vata aggravates, the lakshanas are vakparushyam, karshyam, karshnyam, gatra sphurana, ushna kamitva, nidra nasham, alpabalatva and gadha varcastvam.
Caraka mentions in detail the diseases that can be caused by vitiated vata in general.
सङ्कोचः पर्वणां स्तम्भो भेदोऽस्थ्नां पर्वणामपि ||२०||
लोमहर्षः प्रलापश्च पाणिपृष्ठशिरोग्रहः |
खाञ्ज्यपाङ्गुल्यकुब्जत्वं शोषोऽङ्गानामनिद्रता ||२१||गर्भशुक्ररजोनाशः स्पन्दनं गात्रसुप्तता |
शिरोनासाक्षिजत्रूणां ग्रीवायाश्चापि हुण्डनम् ||२२||भेदस्तोदार्तिराक्षेपो मोहश्चायास एव च |
एवंविधानि रूपाणि करोति कुपितोऽनिलः ||२३||हेतुस्थानविशेषाच्च भवेद्रोगविशेषकृत् |२४| (CS.Ci.28)
Vitiated vata causes various symptoms like contractures, joint stiffness, splitting of bones and joints, horripilation, delirium, spasticity of hands, back and neck; limping, paraplegia, hunch back; organ atrophy, insomnia, intrauterine death of embryo and fetus, diminishing sperms and menstruation fasciculation, generalised numbness, benumbing or paralysis of muscles of head, nose, eyes, supraclavicular part and neck; splitting, pricking or aching type of pains; convulsions, loss of consciousness, fatigue etc. Different specific diseases of vata are caused by specificity in etiological factors and site of affliction. Here, vata vriddhi lakshana and the vata vyadhi can be connected as the treating physician has mentioned that there is a vata vriddhi.
The treatment and the rationale of treatment: As the vata is the predominant dosa that is causing the disease, vata vyadhi cikitsa can be followed. Snehana, swedana and mridu shodhan are the general treatments followed. Apart from this, there are specific treatments mentioned for specific vata vyadhis. Vangasena mentions Dipana, pacana, vamana, virecana, vasti and siravyadha as the line of treatment. This being a vatavyadhi, the basic treatment target is to pacify vata.
The rationale of treatment as explained by the treating physician is given below.
Table 1. The medicines/therapies chosen and their specific rationales explained by the physician
Sadyasadhyata:
As this is not a direct correlation from the Classical textbooks of Ayurveda, the sadhyasadhyata cannot be given a direct reference. But, hypothetically the general rule of sadhyasadhyata can be applied to this.
नवान्बलवतस्त्वेतान्साधयेन्निरुपद्रवान्||७४|| (CS.Ci. 28/74)
The disease of recent onset, in a strong person and without any complications are sadhya. But in this case report, there is a serious damage to the brain, and the complications have manifested. Inspite of the standard of care, the patient was not improving. So from the Ayurvedic perspective, it can be said that it is Kricchrasadhya.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Dhanadanayanadi Kwatha Kashayam 20 ml Oral, thrice daily With 20 ml of warm water before food 2023-05-31 - 2023-06-30 Sahasrayoga.Kashaya prakarana Sandhaniya Mahakashaya Tablet 2 Oral, twice daily after food 2023-05-31 - 2023-09-30 Ayurvedic Patent & Proprietary Medicine Panchamrita loha guggulu Tablet 2 Oral, thrice daily after food 2023-05-31 - 2023-09-30 Bhaishajya Ratnavali Mastishka Rogadhikara 52-55 Vata kulantak rasa Tablet 1 Oral, thrice daily after food 2023-05-31 - 2023-09-30 Bhaishajya Ratnavali Apasmara Rogadhikara 40 - 43 Bruhat vat chintamani rasa Tablet 2 Oral, twice daily after food 2023-05-31 - 2023-09-30 Bhaishajya Ratnavali Vatavyadhi Rogadhikara 502 - 505 Gandha tailam capsule Capsule 2 Oral, twice daily after food 2023-05-31 - 2023-09-30 Ayurvedic Patent & Proprietary Medicine Medha sagar rasa Capsule 1 Oral, twice daily after food 2023-05-31 - 2023-09-30 Ayurvedic Patent & Proprietary Medicine Tab Amlant Tablet 1 Oral, twice daily after food 2023-08-24 - 2023-09-30 Ayurvedic Patent & Proprietary Medicine Ashwgandharishta Arishta 10 ml Oral, twice daily With 10 ml of warm water after food 2023-09-24 - 2023-10-31 Bhaishajya Ratnavali. Murccha Rogadhikara 13-17 Balarishta Arishta 10 ml Oral, twice daily With 10 ml of warm water after food 2023-09-24 - 2023-10-31 Bhaishajya Ratnavali Vatavyadhi 569 - 572 Punarnava + vaca + jatiphala+ haridra and fresh bamboo shoot Samyoga lepa dravya Required Quantity- Dravyas boiled in rice washed water and made into a homegenous lepa Apply as lepa on shiras 2023-05-31 - 2023-09-15 Anubhuta Yoga Maha sneha Sneha yoga 100 ml Matra vasti 2023-05-31 - 2023-06-30 AH.Su.19 -
Outcome Measures
OUTCOME MEASURES
In this case report, a 50-year-old female patient presented with headache and heaviness in the head, associated with heaviness in both eyes, irrelevant speech, short term memory loss, left eye ptosis and drowsiness for 10 days. She had a history of Road Traffic Accident before 20 days. She was diagnosed with left fronto parietal temporal subarachnoid bleed. The condition resolved with the standard of care, but the patient gradually developed several complications. The patient’s family opted for Ayurvedic treatment and approached Dr Rajnikanth for further management. Based on the Multislice CT Scan of the Brain and clinical examination, the biomedical diagnosis was Post traumatic subarachnoid haemorrhage complications. The Ayurvedic diagnosis was Masthishka janya vayu vruddhi (Abhighataja).
Assessment: Both objective and subjective parameters were assessed to analyse the outcome of the ayurvedic treatment.
Subjective parameters:
- After 3 months of treatment, headache and heaviness in head- resolved, heaviness in both eyes- resolved, speech- improved and short-term memory loss- reduced.
- After 4 months of treatment, the patient got complete relief from symptoms.
Objective Parameters:
Glasgow Coma scale was documented at baseline and endpoint to assess the outcome of the ayurvedic treatment. Glasgow Coma Scale was recored as 8 at baseline that improved to 15 at endpoint, indicating the improvement in the quality of life and the relief from the symptoms.
Image 1. Glasgow Coma scale documented at endpoint filled by the Physician on the mentioned date.
-