Featured Case
-
Abstract
A 43-year-old male patient complained of a painless hard mass in the left axillary region that was slowly progressing since the past 2 months. He consulted Dr Aditya Mishra via telephone and took ayurvedic medicines for 20 days, but did not get relief. So he consulted an allopathic doctor and took conventional medicine for a few days, but the symptom did not resolve. He restarted ayurvedic treatments and was referred to a Modern Hospital for detailed investigations. FNAC, PET Scan and Biopsy done confirmed the biomedical diagnosis as Diffuse Large B cell Lymphoma- stage 3, and was scheduled for Chemotherapy. The Ayurvedic diagnosis was Mamsa arbuda. The line of treatment adopted was Tridosa shamana specifically kapha and pitta hara. Dipana- Pacana, medhya and rasayana dravyas were also given. Along with chemotherapy, ayurvedic treatments were integrated with specific dietary recommendations and psychotherapy. This integrative approach could minimise the side effects during CT, no delay in CT and no secondary infections reported. The Scored Patient- Generated Subjective Global Assessment, revealed that the quality of life of the patient could be enhanced. The Deauville Score that was documented as 3 at baseline, became 1 at endpoint. This case report portrays the successful integrative management of DLBCL with Chemotherapy, ayurveda, diet, psychotherapy, and specific use of functional food.
-
Summaries
-
Listen
-
Watch
-
View
-
Read

A 43-year-old male patient complained of a painless hard mass in the left axillary region that was slowly progressing since the past 2 months. He consulted Dr Aditya Mishra via telephone and took ayurvedic medicines for 20 days, but did not get relief. So he consulted an allopathic doctor and took conventional medicine for a few days, but the symptom did not resolve. He restarted ayurvedic treatments and was referred to a Modern Hospital for detailed investigations. FNAC, PET Scan and Biopsy done confirmed the biomedical diagnosis as Diffuse Large B cell Lymphoma- stage 3, and was scheduled for Chemotherapy. The Ayurvedic diagnosis was Mamsa arbuda. The line of treatment adopted was Tridosa shamana specifically kapha and pitta hara. Dipana- Pacana, medhya and rasayana dravyas were also given. Along with chemotherapy, ayurvedic treatments were integrated with specific dietary recommendations and psychotherapy. This integrative approach could minimise the side effects during CT, no delay in CT and no secondary infections reported. The Scored Patient- Generated Subjective Global Assessment, revealed that the quality of life of the patient could be enhanced. The Deauville Score that was documented as 3 at baseline, became 1 at endpoint. This case report portrays the successful integrative management of DLBCL with Chemotherapy, ayurveda, diet, psychotherapy, and specific use of functional food.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
An integrative approach to successful management of cancer- a case report
Dr Aditya Mishra
ABSTRACT
A 43-year-old male patient complained of a painless hard mass in the left axillary region that was slowly progressing since the past 2 months. He consulted Dr Aditya Mishra via telephone and took ayurvedic medicines for 20 days, but did not get relief. So he consulted an allopathic doctor and took conventional medicine for a few days, but the symptom did not resolve. He restarted ayurvedic treatments and was referred to a Modern Hospital for detailed investigations. FNAC, PET Scan and Biopsy done confirmed the biomedical diagnosis as Diffuse Large B cell Lymphoma- stage 3, and was scheduled for Chemotherapy. The Ayurvedic diagnosis was Mamsa arbuda. The line of treatment adopted was Tridosa shamana specifically kapha and pitta hara. Dipana- Pacana, medhya and rasayana dravyas were also given. Along with chemotherapy, ayurvedic treatments were integrated with specific dietary recommendations and psychotherapy. This integrative approach could minimise the side effects during CT, no delay in CT and no secondary infections reported. The Scored Patient- Generated Subjective Global Assessment, revealed that the quality of life of the patient could be enhanced. The Deauville Score that was documented as 3 at baseline, became 1 at endpoint. This case report portrays the successful integrative management of DLBCL with Chemotherapy, ayurveda, diet, psychotherapy, and specific use of functional food.
KEYWORDS
Cancer, arbuda, lymphoma, case report, DLBCL, Integrative
INTRODUCTION
Diffuse large B-cell lymphoma (DLBCL) is a fast-growing blood cancer and the most common form of non-Hodgkin lymphoma. There are different forms of DLBCL that happen when several different genetic changes, or mutations, turn healthy cells into cancerous cells.
B-cell lymphomas frequently affect the lymphatic system. The lymphatic system is a network of tissues, vessels and organs that work together to move a colorless, watery fluid called lymph, back into your bloodstream. Lymph contains B cells (B lymphocytes). B cells make antibodies. Antibodies are proteins that target intruders such as viruses and bacteria. Normally, healthy B-cells die when they’re done fighting infection. B-cell lymphoma happens when healthy B-cells change into fast-growing cancer cells that don’t die the way that they should. The cancer cells duplicate, eventually overwhelming healthy cells. In diffuse large B-cell lymphoma, cancerous B-cells may appear in the lymph nodes, but in some cases, they can appear in virtually any organ, including your gastrointestinal tract, thyroid, skin, breast, bone or brain. Diffuse large B-cell lymphoma is aggressive, meaning it may spread very quickly.
Causes:Diffuse large B-cell lymphoma happens when B-cells mutate. These are acquired genetic mutations, meaning you develop them during your lifetime instead of being born with them. Medical researchers aren’t sure what triggers these mutations, but having a family history of DLBCL could be a risk factor. A risk factor is an activity or condition that increases your risk of developing a disease.
Symptoms:The symptoms most people notice are swollen lymph nodes in their neck, armpits or groin. They may notice a lump or mass that doesn’t go away and seems to be getting larger. Other symptoms sometimes include:
Unexplained fever: A fever that stays above 103 degrees Fahrenheit (39.5 degrees Celsius) that lasts longer than two days or that comes back may be a sign of a serious issue.
Heavy night sweats: This is sweating that’s so intense it drenches your sheets.
Unexplained weight loss: This is losing body weight without trying. Losing 10% of your total body weight over six months is a sign of unexplained weight loss.
Diagnosis: Several different blood tests and an imaging test to diagnose this condition. They also do genetic testing to understand whether specific mutations, or changes, are part of how a given case of diffuse large B-cell lymphoma occurred. Some commonly used diagnostic tests are as follows:
- Complete blood count (CBC) with differential.
- Comprehensive metabolic profile (CMP).
- Lactate dehydrogenase (LDH).
- Human immunodeficiency virus (HIV/AIDS).
- Hepatitis B and Hepatitis C virus.
- Lymph node biopsy.
- Positron emission tomography (PET) scan and/or computed tomography (CT) scan.
Treatment: There are 4 stages of DLBCL, and the treatment will be planned taking into consideration the stage that the patient is in. The standard treatment is R-CHOP. It combines the monoclonal antibody drug rituximab with three chemotherapy drugs and a drug that helps kill lymphoma cells. This treatment is safe and effective but doesn’t always work or keep DLBCL from coming back. (Studies show relapses or recurring disease affect an estimated 10% to 35% of people who receive R-CHOP.) If that happens, healthcare providers may recommend the following treatments: Second-line therapy and autologous stem cell transplant, Chimeric antigen receptor (CAR) T-cell therapy and Targeted therapy
Prognosis: Like many kinds of cancer, healthcare providers have more success treating early-stage DLBCL than advanced or later-stage cancer that’s spread. In general, people who are cancer-free two years after their diagnosis can expect to live as long as most people in their age group. However, diffuse large B-cell lymphoma can relapse. And there are different forms of DLBCL that are more difficult to treat.
PATIENT INFORMATION
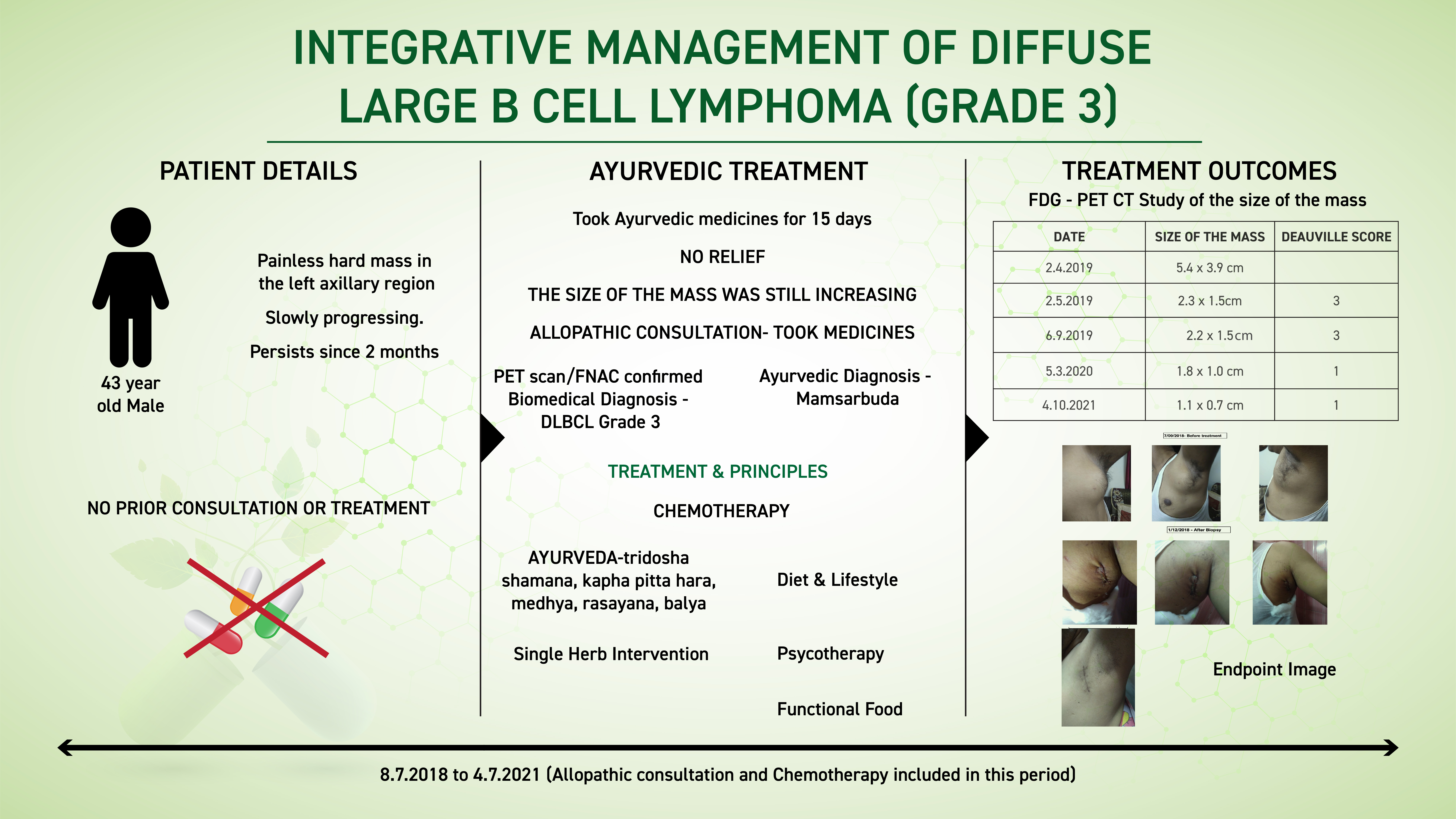
In this case report, a 43-year-old male patient complained of a painless hard mass in the left axillary region that was slowly progressing since the past 3 months. He tried Ayurvedic medicines but there was no relief. He consulted an allopathic doctor and took conventional medicine, which also did not resolve his complaints. Again he restarted ayurvedic medicines and was referred to a modern hospital. FNAC, PET Scan and Biopsy done confirmed the biomedical diagnosis as Diffuse Large B cell Lymphoma- Stage 3.
No relevant family/genetic/surgical history
Psychosocial history- Stressed
CLINICAL FINDINGS
On examination
July 2018- No examinations were done as it was a telephonic consultation
August 2018- Physical examination done. On palpation of left axillary region- tenderness, hard mass, movable. It was a lemon sized mass. No discoloration or redness observed.
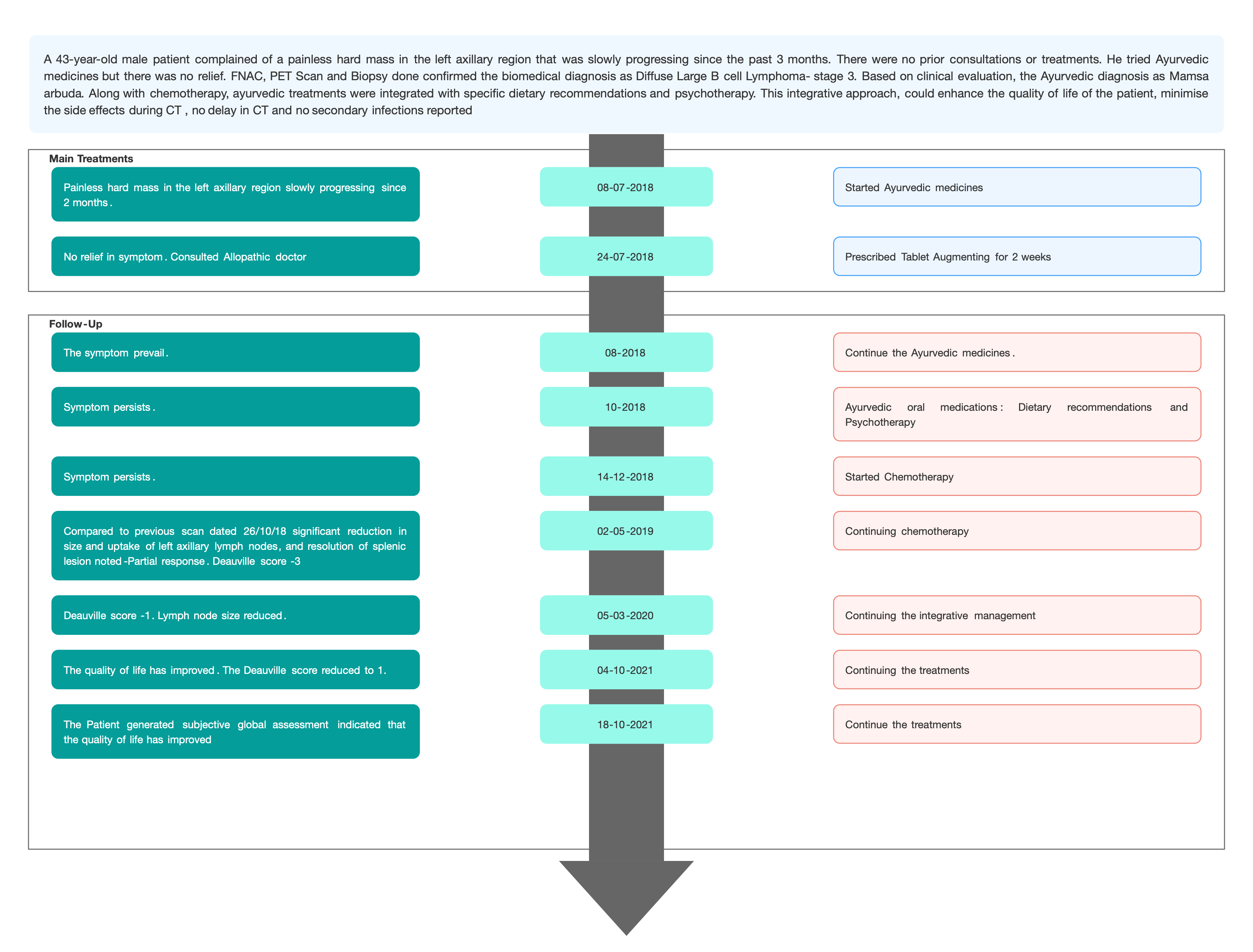
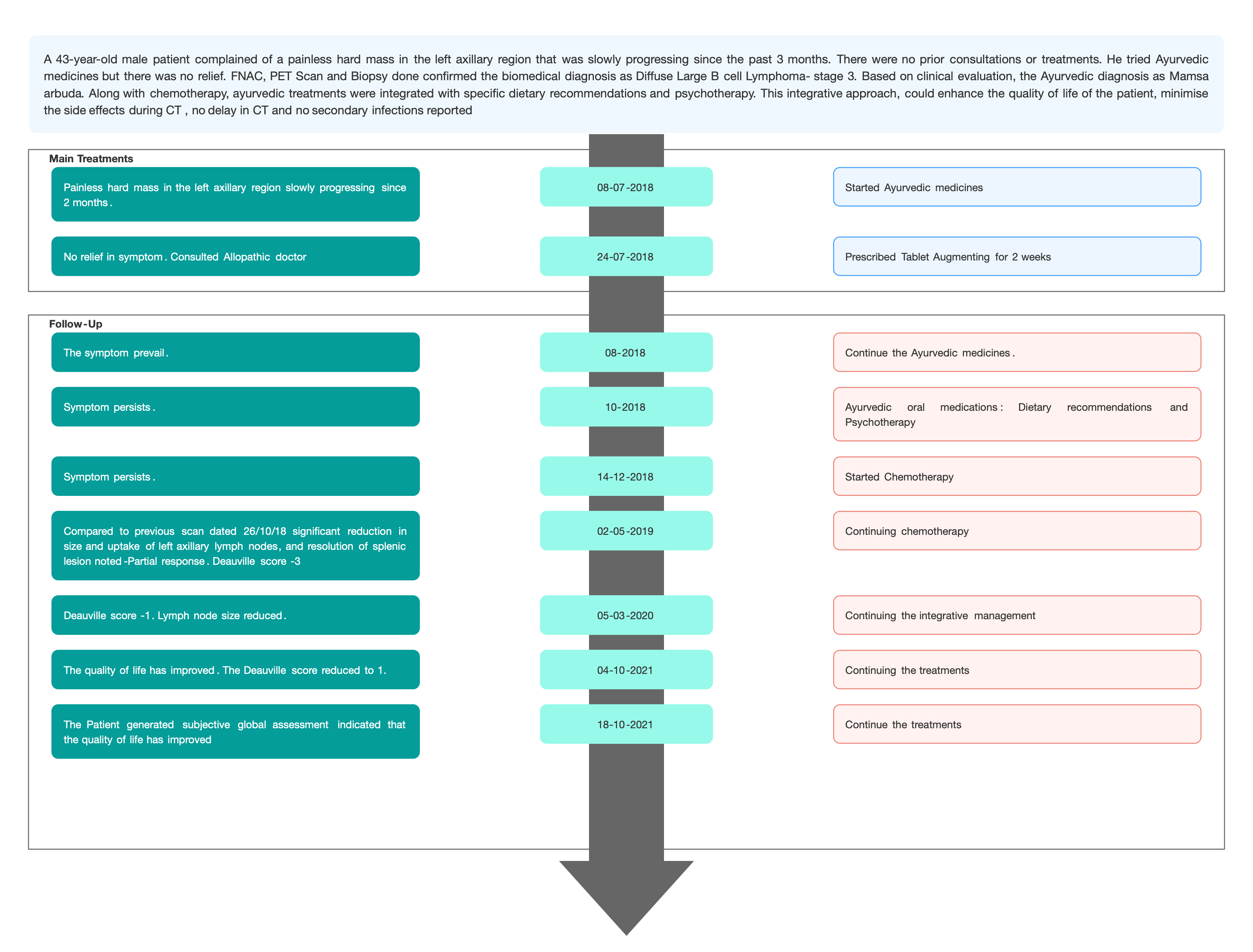
TIMELINE
Image 1. Timeline of events added below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter; Based on the clinical examination and FNAC- PET Scan, the biomedical diagnosis was made as Diffuse Large B Cell Lymphoma- Stage 3.
Image 2. Before treatment dated 7.9.2018

Image 3. Diagnosis proof document dated 26.10.2018
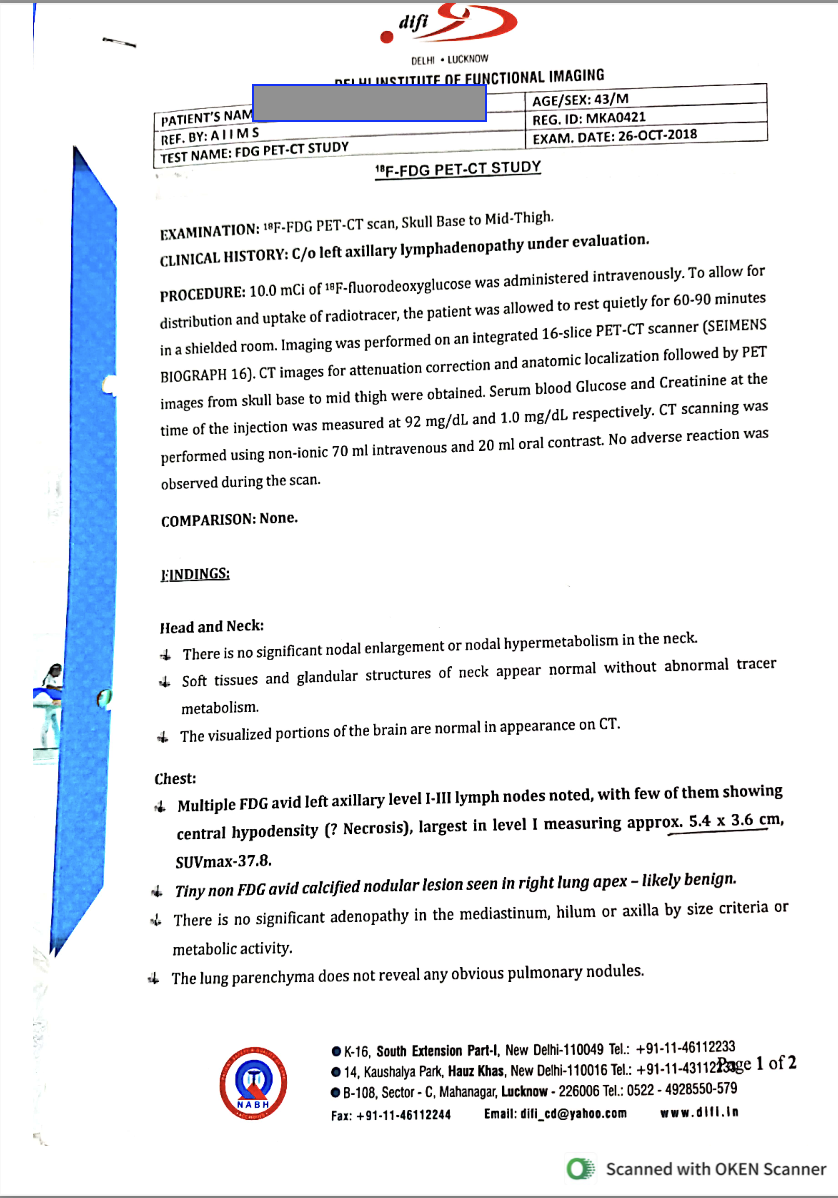
Image 4. Histopathology report dated 5.12.2018
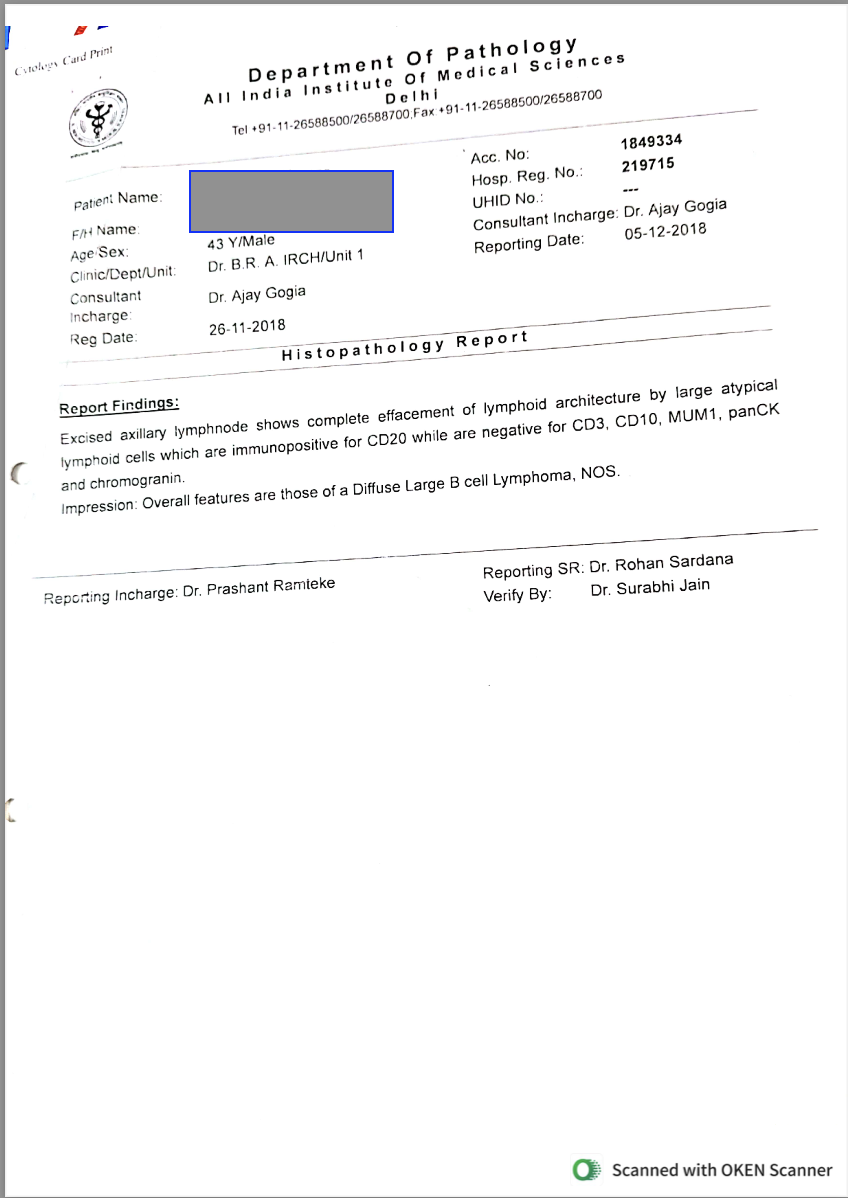
Ayurvedic Assessment was done based on the presenting complaints and clinical evaluation. The treating physician confirmed the Ayurvedic diagnosis as Mamasarbuda.
Differential Diagnosis-
Infectious mononucleosis, Hodgkin lymphoma, T-cell lymphomas.
Based on previous treatment records and investigation reports, the condition was previously diagnosed as DLBCL- grade 3 and reconfirmed by the treating physician.Prognosis- Diffuse large B cell lymphoma (DLBCL) is the most common form of non-hodgkin lymphoma, accounting for approximately 25% to 30% of all cases. This disease typically presents as a rapidly growing mass or the enlargement of lymph nodes in either nodal or extranodal locations. Although it is an aggressive condition, DLBCL generally responds well to chemotherapy. In this case, Ayurvedic treatment along with dietary regimens and psychotherapy could provide supportive care in cancer treatment thereby enhancing the overall quality of life.
THERAPEUTIC INTERVENTION
Refer the tab ‘Treatment’ in the Portal.
FOLLOW-UP AND OUTCOMES
The patient had 8 follow ups in total. Each follow up, the symptoms were assessed and tests were done to analyse the outcome.
Subjective parameters: Images were taken of the mass during the entire course of treatment so as to assess the outcome.
Image 5. After Biopsy dated 1.12.2018

Image 6. After Biopsy dated 20.3.2019

Image 7. After Biopsy dated 28.4.2019

Image 8. After the 6th Chemotherapy

Clinician-based assessment; The repeat PET CT Scan done at regular intervals to assess the size of the mass.
Image 9. PET CT scan dated 2.5.2019
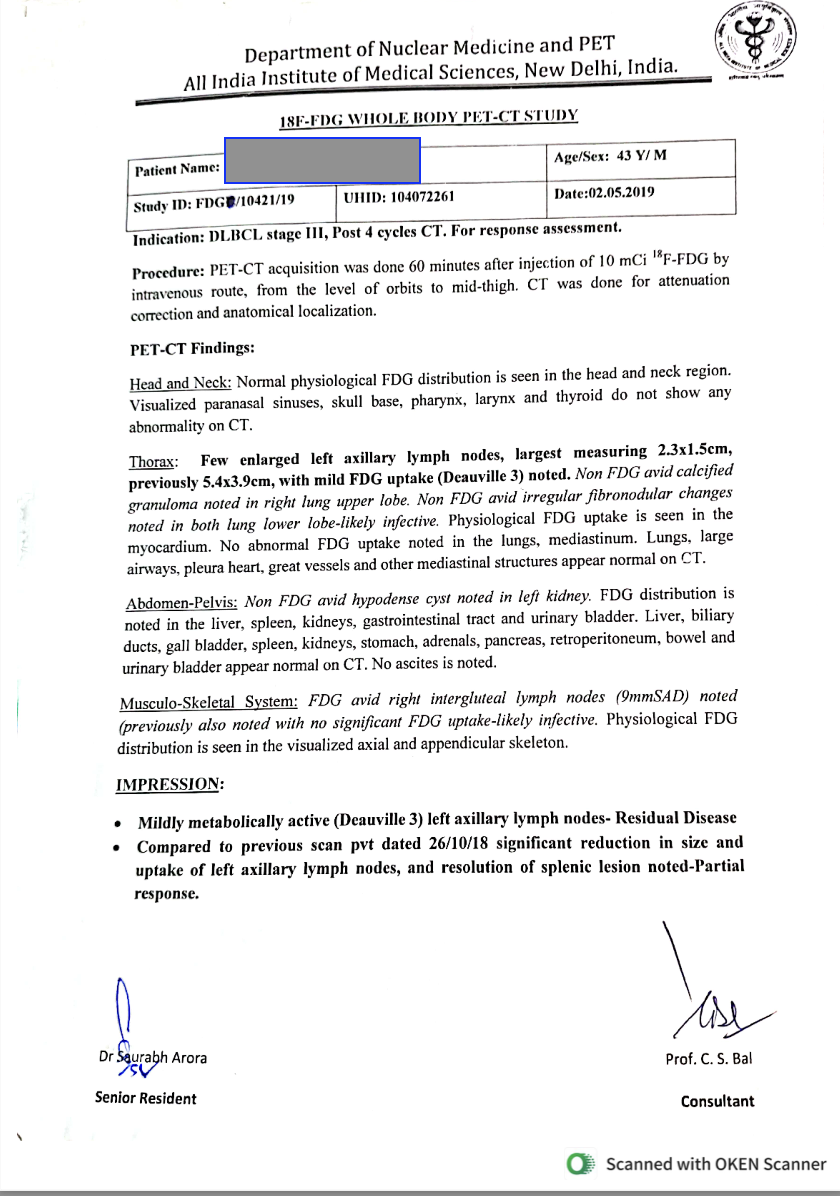
Image 10. PET CT scan dated 6.9.2019
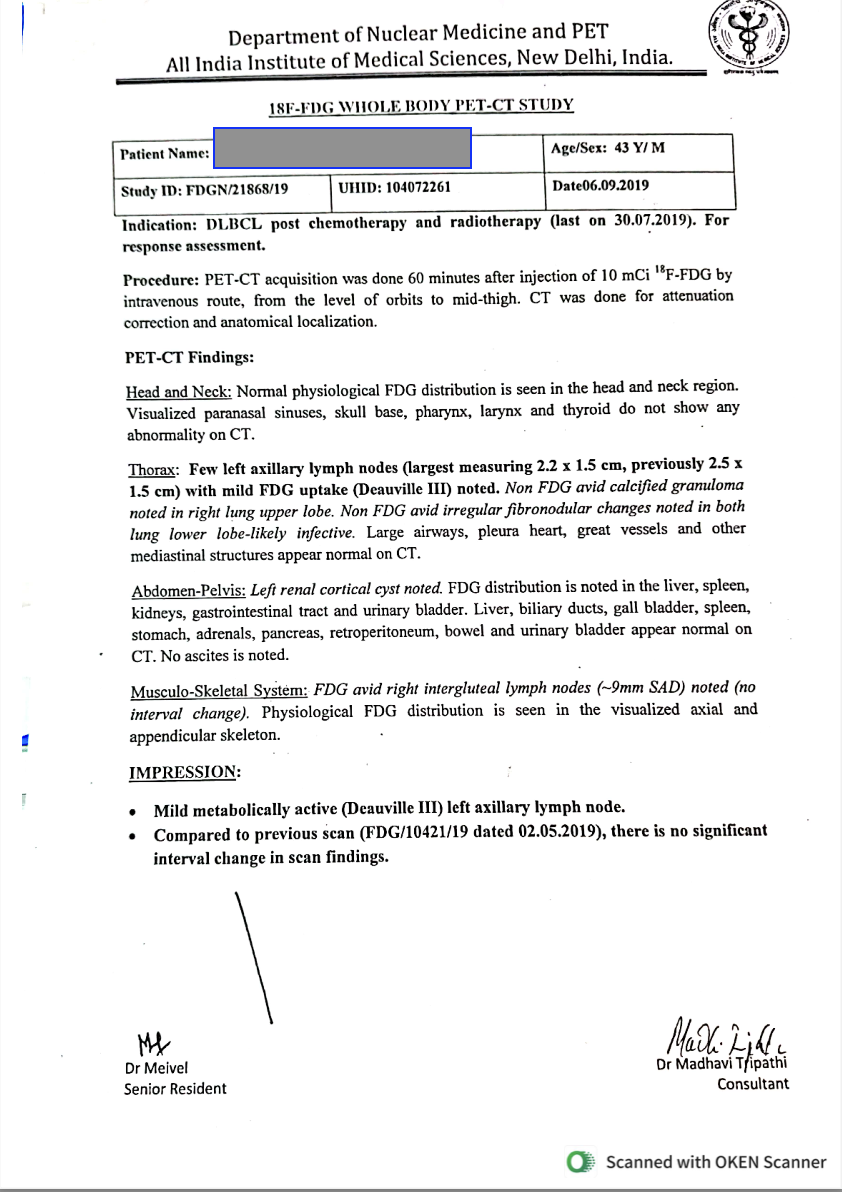
Image 11. PET CT scan dated 5.3.2020
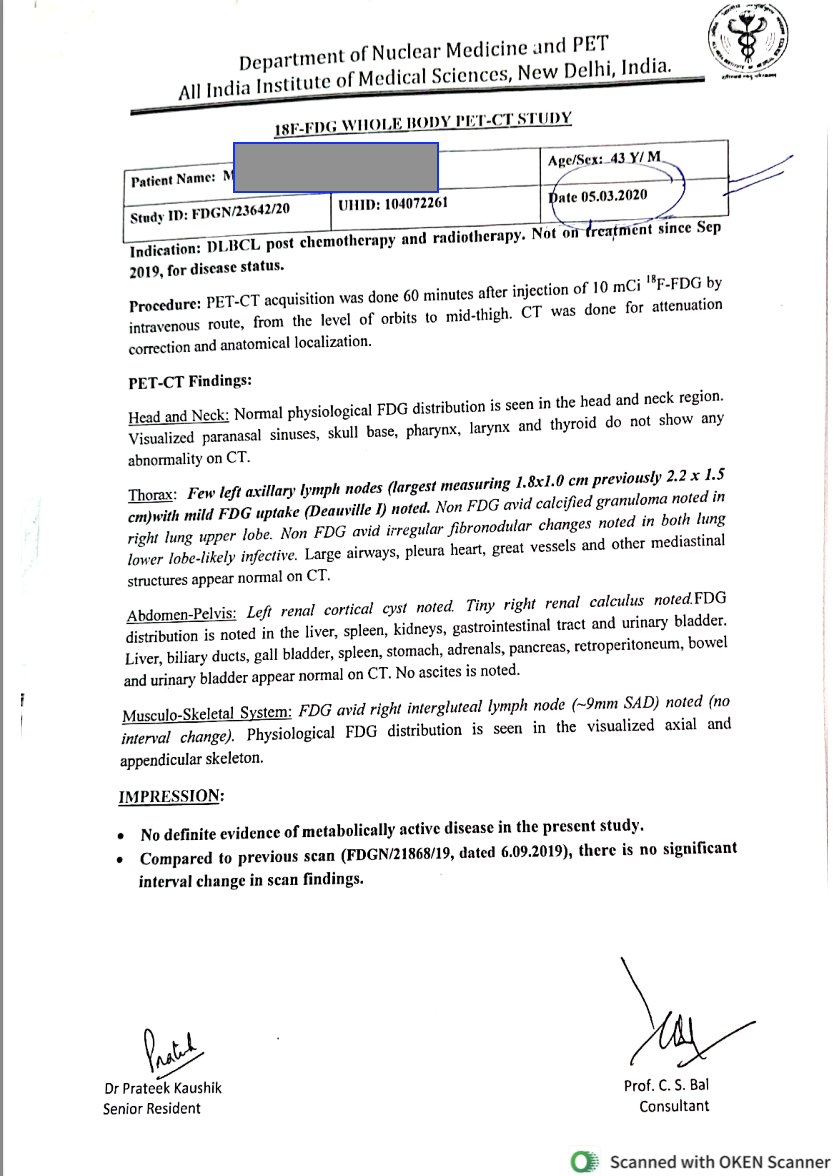
Image 12. PET CT scan dated 4.10.2021
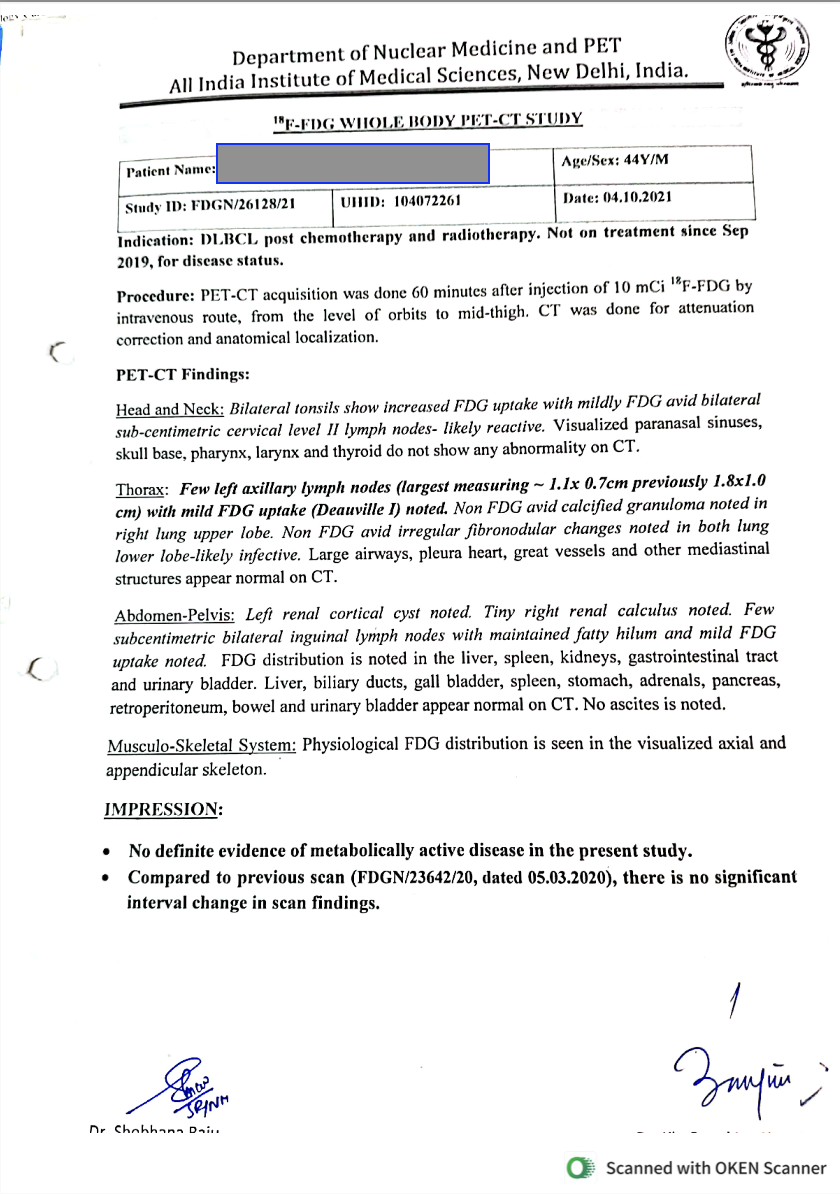
There was a significant reduction in the size of the mass as evident from the PET CT Scan reports.
Table 1. The size of the mass and the Deauville score assessed throughout the treatment
DATE
SIZE OF THE MASS
DEAUVILLE SCORE
26.10.2018
5.4 x 3.9 cm
2.5.2019
2.3 x 1.5cm
3
6.9.2019
2.2 x 1.5
3
5.3.2020
1.8 x 1.0 cm
1
4.10.2021
1.1 x 0.7 cm
1
Patient-assessed; The OG- SGA score was done at endpoint indicating the enhancement in the the quality of life of the patient, minimise the side effects during CT , no delay in CT and no secondary infections reported.
Image 14. The Patient generated subjective global assessment at endpoint
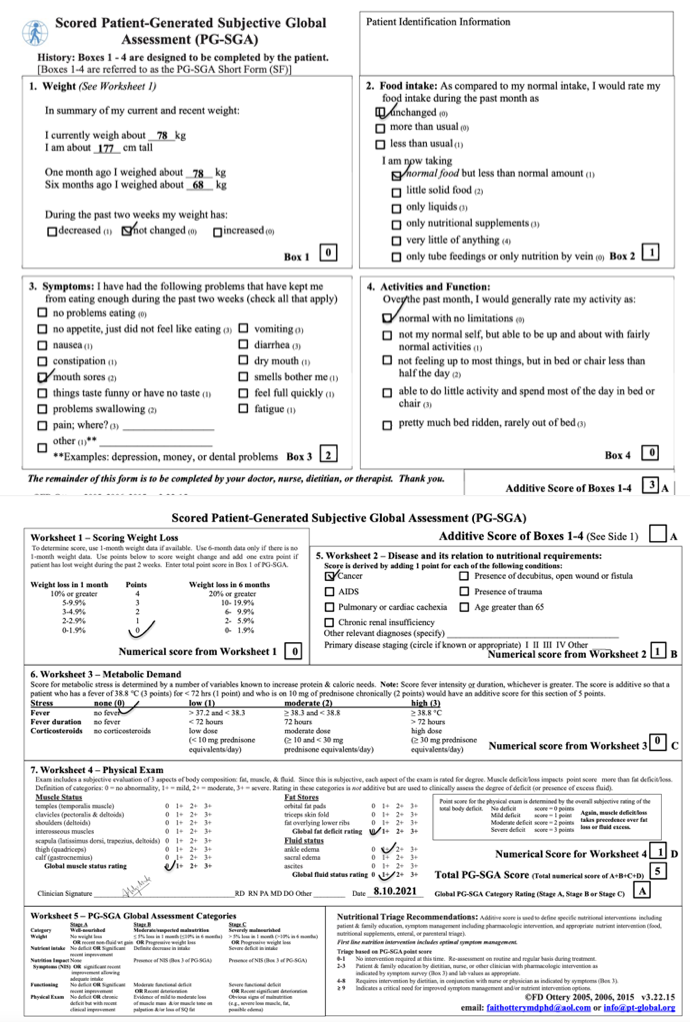
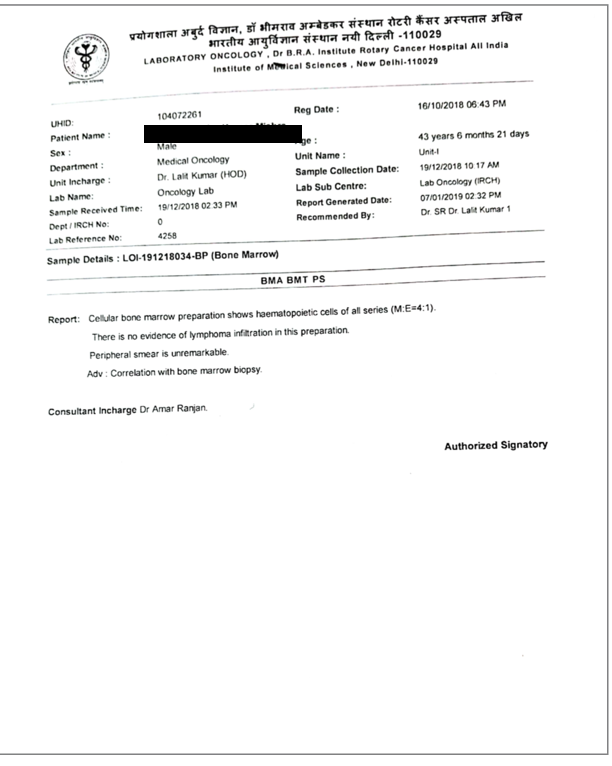
Image 15. Bone marrow biopsy done dated 7.1.2019
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- Subjective and objective parameters were the main assessment tools.
Adverse and unanticipated events; None reported
DISCUSSION:
Early-stage DLBCL can be treated successfully than advanced or later-stage cancer that’s spread. In general, people who are cancer-free two years after their diagnosis can expect to live as long as most people in their age group. In this patient the stage was identified as 3, indicating that it had crossed the mild intensity stage. The ayurvedic diagnosis was Mamsa arbuda and the treatment targeted at Tridosa shamana specifically kapha and pitta hara. Dipana- Pacana, medhya and rasayana dravyas were also incorporated. Specific diet chart was given to combat the side effects of chemotherapy. Psychotherapy, chemotherapy, diet and ayurvedic treatments, helped managed this condition successfully.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE HOME MESSAGES
This case highlights the efficacy of integrative approach in a patient who was suffering from DLBCL 3. With an integrative approach he achieved a better quality of life with a stable mental status.
INFORMED CONSENT
Written consent obtained from patient for publishing of the case report in the Portal
ACKNOWLEDGEMENTS
None
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
1. https://my.clevelandclinic.org/health/diseases/24405-diffuse-large-b-cell-lymphoma
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Diffuse large B-cell lymphoma (DLBCL) Stage 3
ABOUT THE DISEASE:
Diffuse large B-cell lymphoma (DLBCL) is a fast-growing blood cancer and the most common form of non-Hodgkin lymphoma. There are different forms of DLBCL that happen when several different genetic changes, or mutations, turn healthy cells into cancerous cells.
B-cell lymphomas frequently affect the lymphatic system. The lymphatic system is a network of tissues, vessels and organs that work together to move a colorless, watery fluid called lymph, back into your bloodstream. Lymph contains B cells (B lymphocytes). B cells make antibodies. Antibodies are proteins that target intruders such as viruses and bacteria. Normally, healthy B-cells die when they’re done fighting infection. B-cell lymphoma happens when healthy B-cells change into fast-growing cancer cells that don’t die the way that they should. The cancer cells duplicate, eventually overwhelming healthy cells. In diffuse large B-cell lymphoma, cancerous B-cells may appear in the lymph nodes, but in some cases, they can appear in virtually any organ, including your gastrointestinal tract, thyroid, skin, breast, bone or brain. Diffuse large B-cell lymphoma is aggressive, meaning it may spread very quickly.
Causes:Diffuse large B-cell lymphoma happens when B-cells mutate. These are acquired genetic mutations, meaning you develop them during your lifetime instead of being born with them. Medical researchers aren’t sure what triggers these mutations, but having a family history of DLBCL could be a risk factor. A risk factor is an activity or condition that increases your risk of developing a disease. Other risk factors may include:
Certain viruses, including Epstein-Barr virus, human immunodeficiency virus (HIV), hepatitis B and hepatitis C.
Immunosuppressant drugs taken after organ transplants.
Autoimmune disorders. Immunodeficiency.
Increased body mass index in young adults.
Agricultural pesticides.
Ionizing radiation.
Symptoms:The symptoms most people notice are swollen lymph nodes in their neck, armpits or groin. They may notice a lump or mass that doesn’t go away and seems to be getting larger. Other symptoms sometimes include:
Unexplained fever: A fever that stays above 103 degrees Fahrenheit (39.5 degrees Celsius) that lasts longer than two days or that comes back may be a sign of a serious issue.
Heavy night sweats: This is sweating that’s so intense it drenches your sheets.
Unexplained weight loss: This is losing body weight without trying. Losing 10% of your total body weight over six months is a sign of unexplained weight loss.
This patient had Stage 3, which implies there’s lymphoma in lymph node areas on both sides of (above and below) your diaphragm.
Diagnosis: Several different blood tests and an imaging test to diagnose this condition. They also do genetic testing to understand whether specific mutations, or changes, are part of how a given case of diffuse large B-cell lymphoma occurred. Some commonly used diagnostic tests are as follows:
- Complete blood count (CBC) with differential.
- Comprehensive metabolic profile (CMP).
- Lactate dehydrogenase (LDH).
- Human immunodeficiency virus (HIV/AIDS).
- Hepatitis B and Hepatitis C virus.
- Lymph node biopsy.
- Positron emission tomography (PET) scan and/or computed tomography (CT) scan.
In this case report, a 43-year-old male patient complained of a painless hard mass in the left axillary region that was slowly progressing since the past 3 months. He tried Ayurvedic medicines but there was no relief. He consulted an allopathic doctor and took conventional medicine, which also did not resolve his complaints. Again he restarted ayurvedic medicines and was referred to a modern hospital. FNAC, PET Scan and Biopsy done confirmed the biomedical diagnosis as Diffuse Large B cell Lymphoma- Stage 3. The Ayurvedic diagnosis was made as Mamsa arbuda.
Image 1. Before treatment dated 7.9.2018
Image 2. Diagnosis proof document dated 26.10.2018
Image 3. Histopathology report dated 5.12.2018
Treatment: There are 4 stages of DLBCL, and the treatment will be planned taking into consideration the stage that the patient is in. The standard treatment is R-CHOP. It combines the monoclonal antibody drug rituximab with three chemotherapy drugs and a drug that helps kill lymphoma cells. This treatment is safe and effective but doesn’t always work or keep DLBCL from coming back. (Studies show relapses or recurring disease affect an estimated 10% to 35% of people who receive R-CHOP.) If that happens, healthcare providers may recommend the following treatments:
Second-line therapy and autologous stem cell transplant: Second-line therapy is intensive treatment with combined cancer drugs.
Chimeric antigen receptor (CAR) T-cell therapy: This treatment may be helpful for people with diffuse large B-cell lymphoma that comes back after treatment.
Targeted therapy: This treatment targets the genetic changes or mutations that cause diffuse large B-cell lymphoma.
Prognosis: Like many kinds of cancer, healthcare providers have more success treating early-stage DLBCL than advanced or later-stage cancer that’s spread. In general, people who are cancer-free two years after their diagnosis can expect to live as long as most people in their age group. However, diffuse large B-cell lymphoma can relapse. And there are different forms of DLBCL that are more difficult to treat.
Reference
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Mamsa Arbuda
ABOUT THE DISEASE:
The biomedical diagnosis of Diffuse Large B cell Lymphoma, in this case report has been correlated to Arbuda by the treating physician. The biomedical diagnosis specifies the stage as Grade 3. The treating physician has specified the arbuda as mamsa.
According to Acharya Sushruta, the father of surgery, the aggravated Dosas are accumulated in a particular localised area of the body. There, they cause excess aberration in muscular tissues (mamsa pradushana) and hence in the area, circular- stable-mild painful-larger-broad based-non suppurative growths are caused which are gradually maturing in nature. Such muscular growths will have broader (wider) base and often the base (site of origin) is not visible too. Such abnormal, prominent growths are termed as Arbuda.
गात्रदेशे क्विचदेव दोषा: सम्मूर्च्छिता मांसं अिभप्रदूष्य ।
वृत्तं स्थिरं मन्दरूजं महान्तं अनल्पमूलं चिरवृधिं अपाकं॥
कुर्वन्ति मांसोच्छ्रायं अत्यगाधं तदर्बुदं शस्त्रविदो वदिन्त ॥ (Su.Ni. )Types Based upon the dominance of dosha factor and tissues involved, they are classified as-
1. Vataja arbuda
2. Pittaja arbuda
3. Kaphaja arbuda4. Raktarbuda
5. Mamsarabuda6. Medo arbuda
The symptoms will vary depending upon the type of arbuda.
In this case report, a 43-year-old male patient complained of a painless hard mass in the left axillary region that was slowly progressing since the past 3 months. He tried Ayurvedic medicines but there was no relief. He consulted an allopathic doctor and took conventional medicine, which also did not resolve his complaints. Again he restarted ayurvedic medicines and was referred to a modern hospital. FNAC, PET Scan and Biopsy done confirmed the biomedical diagnosis as Diffuse Large B cell Lymphoma- Stage 3. The Ayurvedic diagnosis was made as Mamsa arbuda.
Lakshana of Mamsarbuda: Constant trauma or damage in any muscular part of the body leads to vitiation of localised area. Further, these tissues undergo instant transformation and quick multiplication of abnormal cells result into a tumour. This is usually painless, unctuous, vivid coloured, non suppurative, palpated like stone and stable in nature. This is caused usually in non vegetarians and such a condition (mamsarbuda) is incurable.
Prognosis: Even among the curable forms of arbuda, the following are to be rejected – that which has heavy discharges (exudation): that occurring on or around the vital organs; that occurring on or around the channels including nasal passage etc (and hence imparting pressure on them and obstructing their functioning); that which is immobile
Treatment and rationale of treatment as specified by the treating physician: Acharya Charaka denotes that the metastasis should be treated as like the cysts or abscesses, as they have similar site of origin, aetiology, characteristic features, dosha and dushya (tissues). The efforts should be carried to achieve the paka of the arbuda and then cauterise it.Table 1. The medicines prescribed and the rationale behind using them
Medicines/ Procedures
Rationale
Arogyavardhini vati
Indicated in Yakrit vikara
Kanchanara guggulu
Helps to balance kapha and reduces medha dhatu.
Sutasekara rasa
Pittashamanam
Gandhaka Rasayana
Broad-spectrum antibiotic activity
Mahalaxmi Vilas rasa
Tridoshamaka
Kutaja ghan vati
In Diarrhoea
Sanka vati
Deepana and pachana
Chitrakadi vati
Kapha shamana
Triphala rasayanam
Tridosha shamaka
Chyavanaprasha + Swarna bhasma
Rasayana, Improve low appetite
Amalaki Rasayana
Kesheya
Brahma Rasayana
Medhya
Kamadudha rasa
Pittashamanam
Sataverex granules
Pittashamanam
Cruelcap
Lekhana
Suvarnavasantha Malathi
Kapha samanam
Triphala churnam
Tridoshaghna
Sitopaladi Churnam + Sphatik bhasma + Abharak bhasm + Praval Pisti
Madiphala rasayana
Cough , cold
Indicated in mandagni
Table 2. Specific diet was advocated to manage the symptoms caused due to chemotherapy.
Diet & its form
Quantity
Time
Indication
Orange
2
11am- 3pm
Vomiting, Dysplasia
Pappaya/ Apple
2
10am- 5pm
Constipation
Banana
2
8am
Diarrhoea
Munnaka
5
At bed time
Immunity, Mucositis
Lemon
1
Juice form
Nausea, Dry mouth
Ginger
Small quantity
Juice/ Curry
Vomiting, Nausea
Palak
Small quantity
Juice/ Curry
Constipation
Potato
Small quantity
Juice/ Curry
Diarrhoea
Lashuna
Small quantity
Juice/ Curry
Cough
Beetroot
Small quantity
Juice/ Curry
Immunity
Honey
Small quantity
Added in juices
Mucositis
Tomato
Small quantity
Juice/ Curry
Dysplasia
Beetroot+ Lemon+ Tomato+ Palak+ Carrot+ Amla+ Giloy+ Pudina+ Wheat grass+ Turmeric Juice
2 glass
7 am- 4:30 pm
Immunity
Table 3. Psychotherapy for the patient
Type of regimen
Duration reccommended
Yajna
on special occasion/ festival
Mantra Chanting
10 min at bed time
Bhaktiyoga
30 min
Meditation
30 min
Yogasana- Sukshma yayama, Padmasana, vajrasana
10 min
Mudras- Jnana mudra, Dhyana mudra
15 min
Pranayamas- Anuloma Viloma, bhastrika, kapalabhati, bramari
30 min (Morning- Evening)
Counselling
As required
Reference:
1. Madhavana Nidana. Chapter 38. Galaganda gandamala apaci grantyarbuda nidanam
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Arogyavardhini vati Vati 2-0-2 Oral, with warm water before food 2018-07-08 - 2018-07-23 Rasendrasarasangraha. Jwararogadhikara 13- 105 Kanchanara guggulu Tablet 2-0-2 Oral, with warm water before food 2018-07-08 - 2018-07-23 Sharangadhara Samhita Madhyamakhanda 7.94 Sutasekara rasa Tablet 1-0-1 Oral, with warm water after food 2018-08-05 - 2018-08-09 Yogaratnakara. Amlapitta cikitsa 705 Gandhaka Rasayana Tablet 1-0-1 Oral, with warm water after food 2018-08-10 - 2018-10-20 Rasatarangini.8. 81-86 Mahalaxmi Vilas rasa Tablet 1-0-1 Oral, with warm water after food 2018-08-10 - 2018-10-20 Rasendrasarasangraha Kapharoga cikitsa.17-29 Kutaja ghan vati Tablet 2-0-2 Oral, with warm water after food 2019-02-11 - 2019-02-13 Sidhayogasangraha -Atisara pravahika grahani rogadhikara Shanka vati Tablet 1-0-1 Oral, with warm water after food 2019-01-15 - 2019-02-13 Bhaishajya Ratnavali Agnimandhya rogadhikara 182-183 Chitrakadi vati Tablet 1-0-1 Oral, with warm water after food 2019-02-15 - 2019-02-25 CS. Ci. 15.96-97 Triphala rasayanam Lehya 1 tsp Oral, at bedtime 2019-02-15 - 2019-02-25 CS. Ci 1.3.41-47 Chyavanaprasha + Swarna bhasma Samyoga 1 tsp + 500 mg of bhasma Oral, at bedtime 2021-10-12 - 2021-11-10 Chyavanaprasha- CS. Ci 1.1.73: ?Swarna bhasma- Rasaratna samucchaya 5.15 Amalaki Rasayana Lehya 1/2 tsp Oral, at bedtime 2021-11-21 - 2021-12-21 CS. Ci- 1.1.75 Brahma Rasayana Lehya 1/2 tsp Oral, at bedtime 2022-01-01 - 2022-02-14 AH. Utt. 39.15-23 Kamadudha rasa Tablet 1-0-1 Oral, at bedtime 2019-05-02 - 2019-07-05 Ayurveda sarasangraha - Rasa Rasayana prakarana Sataverex granules Granules 1 tsp Oral, at 10.30 am and 10 pm 2019-04-01 - 2019-08-24 Patent and Proprietary Medicine Cruelcap Capsule 1 Oral, with warm water after food 2018-08-10 - 2018-10-30 Patent and Proprietary Medicine Suvarnavasantha Malathi Tablet 1 Oral, with warm water after food 2018-08-10 - 2018-10-30 Bhaishajyaratnavali - Jvara cikitsa Triphala curnam Curna 1 Teaspoon Oral, with warm water at bedtime 2018-08-10 - 2018-10-30 Bhavaprakasa Haritakyadi varga Sitopaladi Churnam + Sphatik bhasma + Abhraka bhasma + Praval Pisti Samyoga {50 gm+ 50 gm+ 5 gm+ 10 gm } mixed- 1/2 tsp Oral, with warm water before food 2018-08-10 - 2018-10-30 Sitopaladi Churnam- Sa. Sam Madhyama Khanda 6.134-137: ?Sphatik bhasma- Ayurveda Prakasha 257 - 258: ?Abhraka bhasma- Rasa Tarangini 10.39-42: ?Pravala Pisti- Ayurveda Sara Sangraha, Shodhana marana prakarana p:119, AFI Vol. 1. Madiphala rasayana Lehya 1 tsp Oral, after food twice daily 2018-08-10 - 2019-09-05 Sahasrayogam - Rasayana prakarana Dasamula Kwatha Kashayam Required Quantity Bahya Swedana, once daily 2018-08-10 - 2018-10-30 Bhaishajya Ratnavali Kasarogadhikara 13- 15 -
Outcome Measures
In this case report, a 43-year-old male patient complained of a painless hard mass in the left axillary region that was slowly progressing since the past 3 months. He tried Ayurvedic medicines but there was no relief. He consulted an allopathic doctor and took conventional medicine, which also did not resolve his complaints. Again he restarted ayurvedic medicines and was referred to a modern hospital. FNAC, PET Scan and Biopsy done confirmed the biomedical diagnosis as Diffuse Large B cell Lymphoma- Stage 3. The Ayurvedic diagnosis was made as Mamsa arbuda.
Assessment: Objective parameters were assessed to analyse the outcome of the treatment.
Table 1. FDG- PET Scan reports and Deauville Score during and after treatment tabulated
DATE
SIZE OF THE MASS
DEAUVILLE SCORE
26.10.2018
5.4 x 3.9 cm
2.5.2019
2.3 x 1.5cm
3
6.9.2019
2.2 x 1.5
3
5.3.2020
1.8 x 1.0 cm
1
4.10.2021
1.1 x 0.7 cm
1
The size of the lymph nodes were continuously reducing and the reduction of the Deauville score indicated the intensity of the disease was coming down.
Image 1. PET CT scan dated 2.5.2019
Image 2. PET CT scan dated 6.9.2019
Image 3. PET CT scan dated 5.3.2020
Image 4. PET CT scan dated 4.10.2021
The appearance of the mass was documented with photographs to assess the outcome.
Image 5. After Biopsy dated 1.12.2018
Image 6. After Biopsy dated 20.3.2019
Image 7. After Biopsy dated 28.4.2019
Image 8. After the 6th Chemotherapy
Image 9 Bone marrow biopsy done dated 7.1.2019
Image 10. The Patient generated subjective global assessment at endpoint
This integrative approach, could enhance the quality of life of the patient, minimise the side effects during CT , no delay in CT and no secondary infections reported.
-