Featured Case
-
Abstract
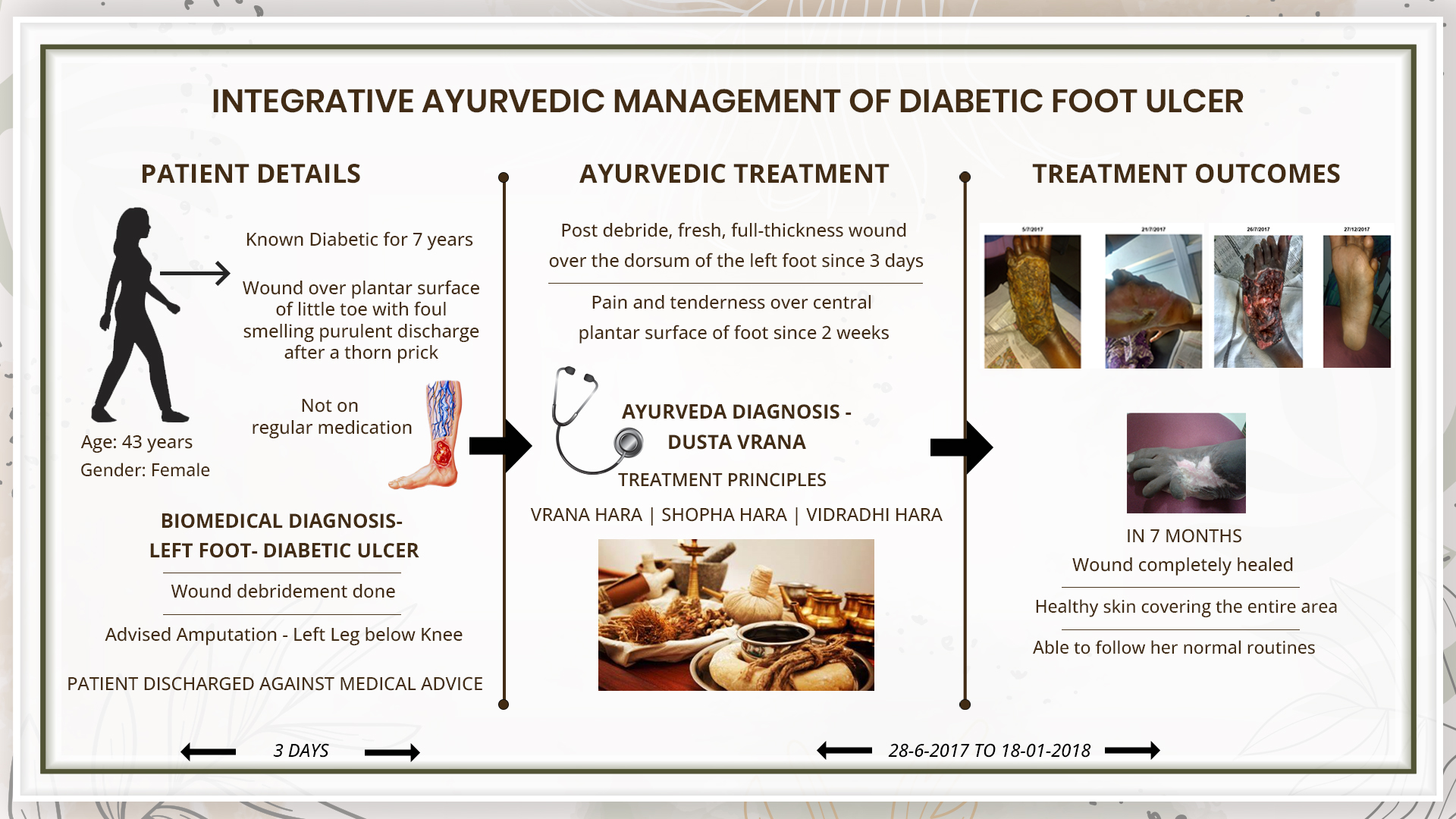
A 43 year old female patient complaints of post debride, fresh, full thickness wound over the dorsum of left foot since 3 days. There is also tenderness over lower 1/4th of tibia and calf muscles since more than 7 years, aggravated since 2 weeks. Pain and tenderness is present over the central plantar surface of foot since 2 weeks. Patient is a known diabetic since 7 years, but not on regular medication. She was diagnosed with Diabetic foot ulcer- based on the clinical examination and USG Colour Doppler of the left leg, by the allopathic doctor. Wound debridement on spinal anaesthesia was done followed by oral medications and injections. She was advised for a below knee amputation to save the limb. As the patient was not willing she approached Dr Jishnu Narayanan for ayurvedic management. The Ayurvedic diagnosis was Dusta Vrana. The line of treatment followed was Vrana, Shopha and Vidradhi hara. With Ayurvedic treatment, the wound healed completely and was covered with healthy skin in 5 months. This case report demonstrates the successful management of a non-healing diabetic foot ulcer, in a patient who was recommended amputation to save the limb.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 43 year old female patient complaints of post debride, fresh, full thickness wound over the dorsum of left foot since 3 days. There is also tenderness over lower 1/4th of tibia and calf muscles since more than 7 years, aggravated since 2 weeks. Pain and tenderness is present over the central plantar surface of foot since 2 weeks. Patient is a known diabetic since 7 years, but not on regular medication. She was diagnosed with Diabetic foot ulcer based on the clinical examination and USG Colour Doppler of the left leg, by the allopathic doctor. Wound debridement on spinal anaesthesia was done followed by oral medications and injections. She was advised for a below knee amputation to save the limb. As the patient was not willing she approached Dr Jishnu Narayanan for ayurvedic management. The Ayurvedic diagnosis was Dusta Vrana. The line of treatment followed was Vrana, Shopha and Vidradhi hara. With Ayurvedic treatment, the wound healed completely and was covered with healthy skin in 5 months. This case report demonstrates the successful management of a non-healing diabetic foot ulcer, in a patient who was recommended amputation to save the limb.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Ayurvedic management of infected post-debride Diabetic Foot ulcer - A case report
Dr Jishnu Narayanan
ABSTRACT
A 43 year old female patient complaints of post debride, fresh, full thickness wound over the dorsum of left foot since 3 days. There is also tenderness over lower 1/4th of tibia and calf muscles since more than 7 years, aggravated since 2 weeks. Pain and tenderness is present over the central plantar surface of foot since 2 weeks. Patient is a known diabetic since 7 years, but not on regular medication. She was diagnosed with Diabetic foot ulcer- based on the clinical examination and USG Colour Doppler of the left leg, by the allopathic doctor. Wound debridement on spinal anaesthesia was done followed by oral medications and injections. She was advised for a below knee amputation to save the limb. As the patient was not willing she approached Dr Jishnu Narayanan for ayurvedic management. The Ayurvedic diagnosis was Dusta Vrana. The line of treatment followed was Vrana, Shopha and Vidradhi hara. With Ayurvedic treatment, the wound healed completely and was covered with healthy skin in 5 months. This case report demonstrates the successful management of a non-healing diabetic foot ulcer, in a patient who was recommended amputation to save the limb.
KEYWORDS
Dusta vrana, foot ulcer, case report, diabetic foot ulcer, standalone
INTRODUCTION
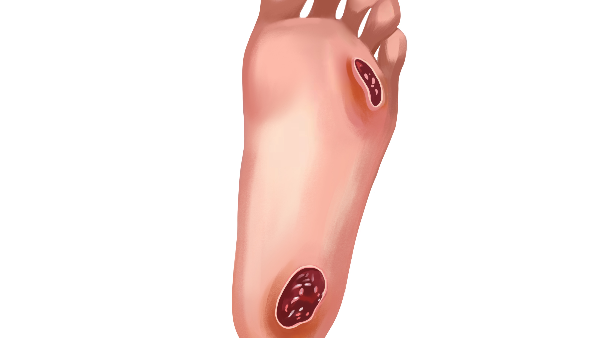
Foot ulcers are a common complication of uncontrolled diabetes- improper diet and lifestyle. Ulcers are formed as a result of skin tissue breaking down and exposing the layers underneath. They’re most common under your big toes and the balls of your feet, and they can affect your feet down to the bones. All people with diabetes can develop foot ulcers, but good foot care can help prevent them. Treatment for diabetic foot ulcers varies depending on their causes.
The lifetime risk of a foot ulcer in patients with diabetes (type 1 or 2) may be as high as 34 percent. Diabetic foot ulcers are a major cause of morbidity, accounting for at least two-thirds of all nontraumatic amputations performed in the United States. Moreover, patients with diabetes with or without a diabetic foot ulcer have increased rates of depression, and expressing signs of depression is associated with an increased risk of diabetic foot ulcers. These observations illustrate the importance of prompt and appropriate treatment of foot ulcers in patients with diabetes.
Symptoms- One of the first signs of a foot ulcer is drainage from your foot that might stain your socks or leak out in your shoe. Unusual swelling, irritation, redness, and odors from one or both feet are also common early symptoms. The most visible sign of a serious foot ulcer is black tissue (called eschar) surrounding the ulcer. This forms because of an absence of healthy blood flow to the area around the ulcer. Partial or complete gangrene, which refers to tissue death due to infections, can appear around the ulcer. In this case, odorous discharge, pain, and numbness can occur. Signs of foot ulcers are not always obvious. Sometimes, you won’t even show symptoms of ulcers until the ulcer has become infected.
Causative factors:
Ulcers in people with diabetes are most commonly caused by:
- poor circulation
- high blood sugar (hyperglycemia)
- nerve damage
- irritated or wounded feet
Nerve damage is a long-term effect and can lead to a loss of feeling in your feet. Damaged nerves can feel tingly and painful. Nerve damage reduces sensitivity to foot pain and results in painless wounds that can cause ulcers.
Diagnostic criteria: Basically, the history taking and clinical evaluation are the important diagnostic tools. Blood tests and swab test can be done as supportive investigations. The University of Texas (UT, San Antonio) in the United States introduced a clinical classification system for diabetic foot wounds that evaluates wound depth, the presence of infection, and peripheral arterial occlusive disease for every category of the wound assessment. The UT system was the first diabetic foot ulcer classification to be validated. This system updated the Wagner classification.
Prognosis: This depends on factors like, how early the wound was found, presence and extent of spread of an infection, and efficacy of the treatment provided. If the infection has spread very far and deep, then amputation may be necessary.
Treatment: The first step in managing diabetic foot ulcers is assessing, grading, and classifying the ulcer. Classification is based upon clinical evaluation of the extent and depth of the ulcer and the presence of infection or ischemia, which determine the nature and intensity of treatment. To assess for ischemia, all patients with diabetic foot ulcers should have ankle-brachial index and toe pressure measurements.The management of diabetic foot ulcers, including local wound care, use of mechanical offloading, treatment of infection, and indications for revascularization.
PATIENT INFORMATION
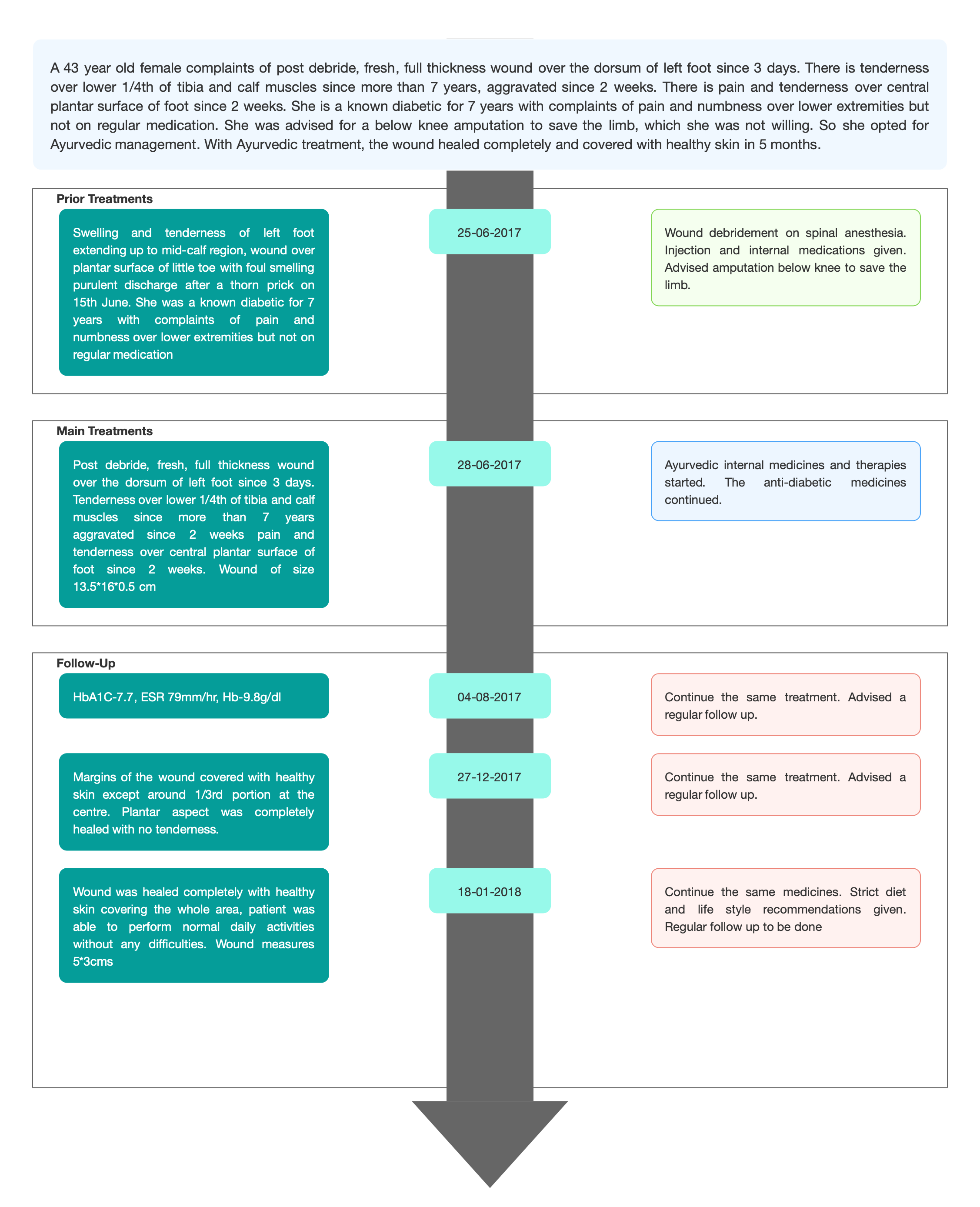
The patient is a 43 year old house wife who is a known diabetic since 7 years. She complained of post debride, fresh, full thickness wound over the dorsum of left foot since 3 days. Tenderness was present over lower 1/4th of tibia and calf muscles since more than 7 years, aggravated since 2 weeks. Pain and tenderness over central plantar surface of foot since 2 weeks. She underwent, Wound debridement on spinal anesthesia and prescribed a course of medicines. But as the wound was not showing any signs of healing, she was advised for a below knee amputation to save the limb.
Surgical history- Wound debridement on spinal anaesthesia on 25/6/17 for left diabetic foot, h/o LSCS.
Psychosocial history- Low economic background.
Addiction- Tobacco chewing
CLINICAL FINDINGS
Toes and surrounding area were showing limited tactile sensation and movements. The foot was cold to the touch with tenderness over the lower 1/4th of the tibia, calf muscles and central plantar surface of the foot.swelling at the knee, elbow, and wrist joints.
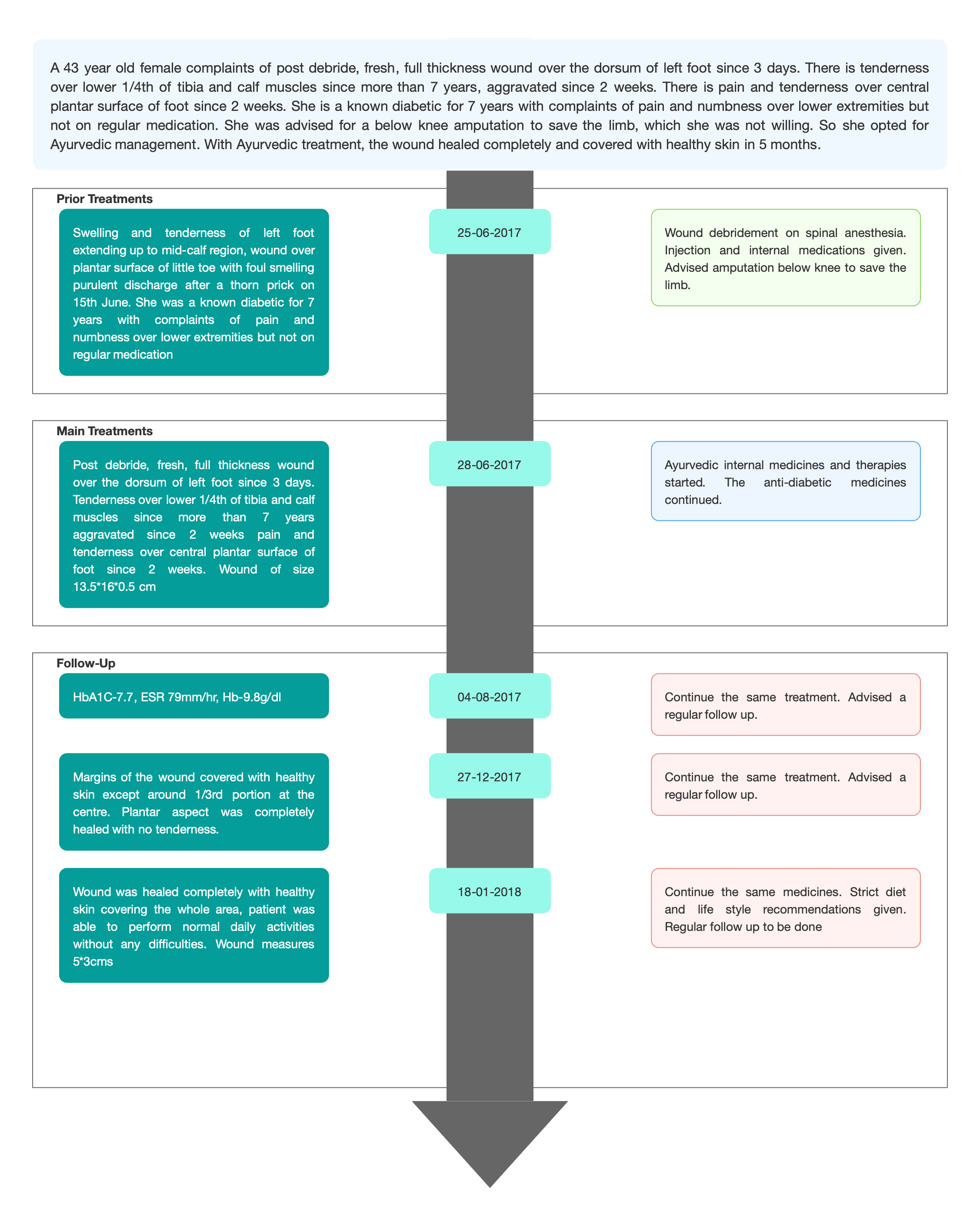
TIMELINE
Image 1. Timeline of events added below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter; The patient was pre-diagnosed with Left Foot Diabetic ulcer.
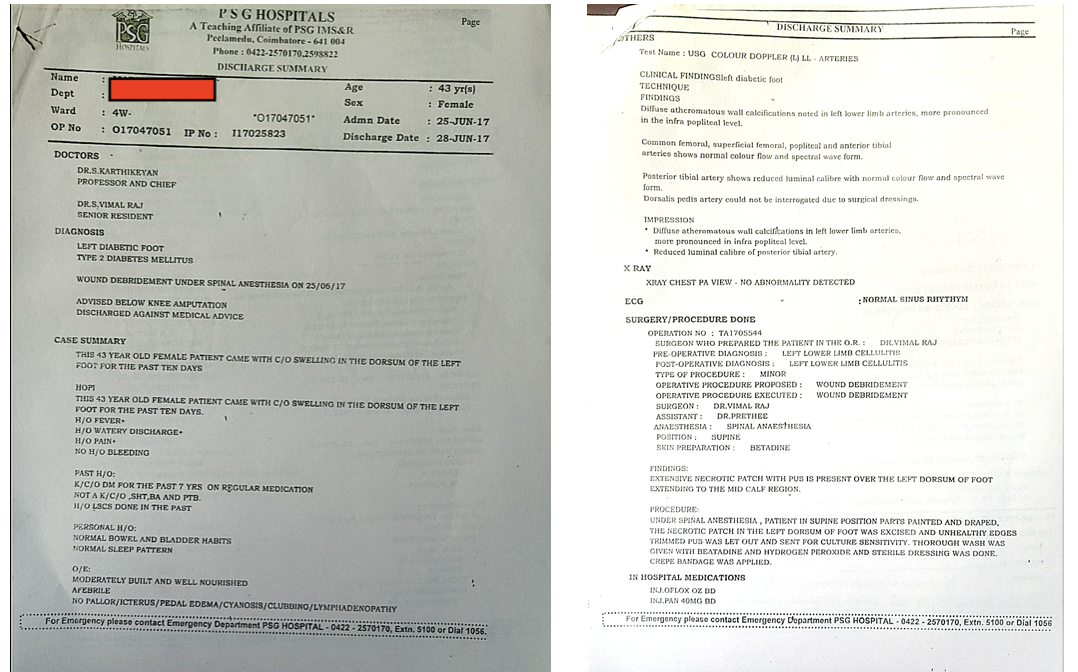
Image 2. Discharge summary confirming the diagnosis and the previous treatment done- 25.6.2017
Ayurvedic Assessment was done based on the presenting complaints and clinical evaluation. The treating physician confirmed the Ayurvedic diagnosis as Dusta vrana.
Image 3. Baseline photo taken of the diabetic foot ulcer dated 5.7.2017

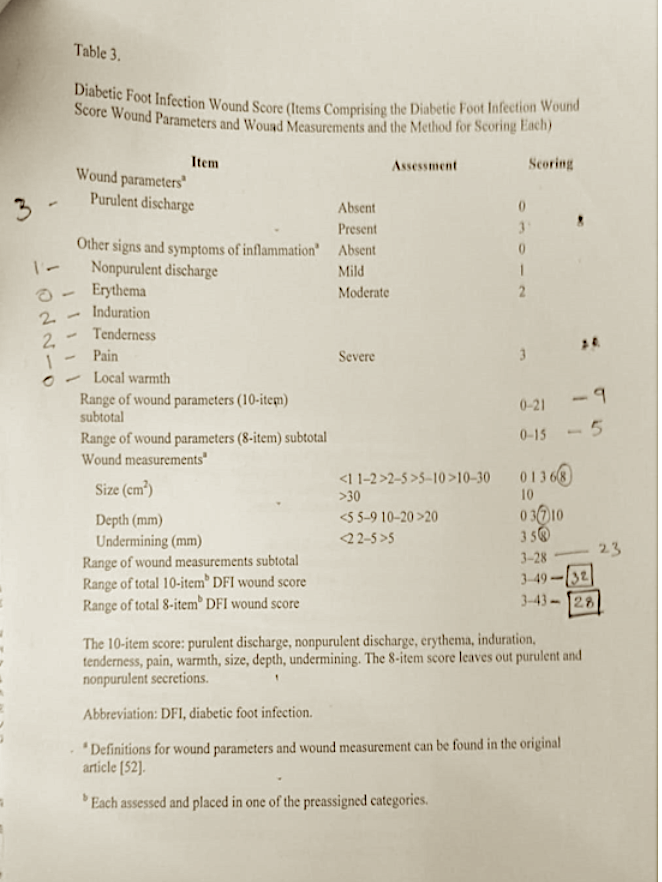
Image 4. Diabetic Foot Infection Wound Score assessed at baseline
Differential Diagnosis-
Blunt bone trauma: Bone tumour: Gas gangrene: Lyme arthritis: Osteomyelitis: Sarcoid arthritis: Sickle cell crisis: Squamous cell carcinoma: Superficial thrombophlebitis: Synergistic gangrene. The patient came in with a confirmed diagnosis.
Prognosis- The prognosis of diabetic ulcers is dependant on various factors such as strict diabetes control, patient education, a healthy lifestyle, and proper wound care. Poor blood supply, infection, prolonged duration, and recurrent ulcers are associated with poor prognosis. In this patient, inspite of taking the standard care and wound debridement, the condition of wound worsened and was suggested for below knee amputation. With Ayurvedic treatment, the wound healed completely and covered with healthy skin in around 5 months.
THERAPEUTIC INTERVENTION
Refer the tab ‘Treatment’ in the Portal.
FOLLOW-UP AND OUTCOMES
The patient had 6 follow ups in total.
The wound was assessed regularly and was tabulated.
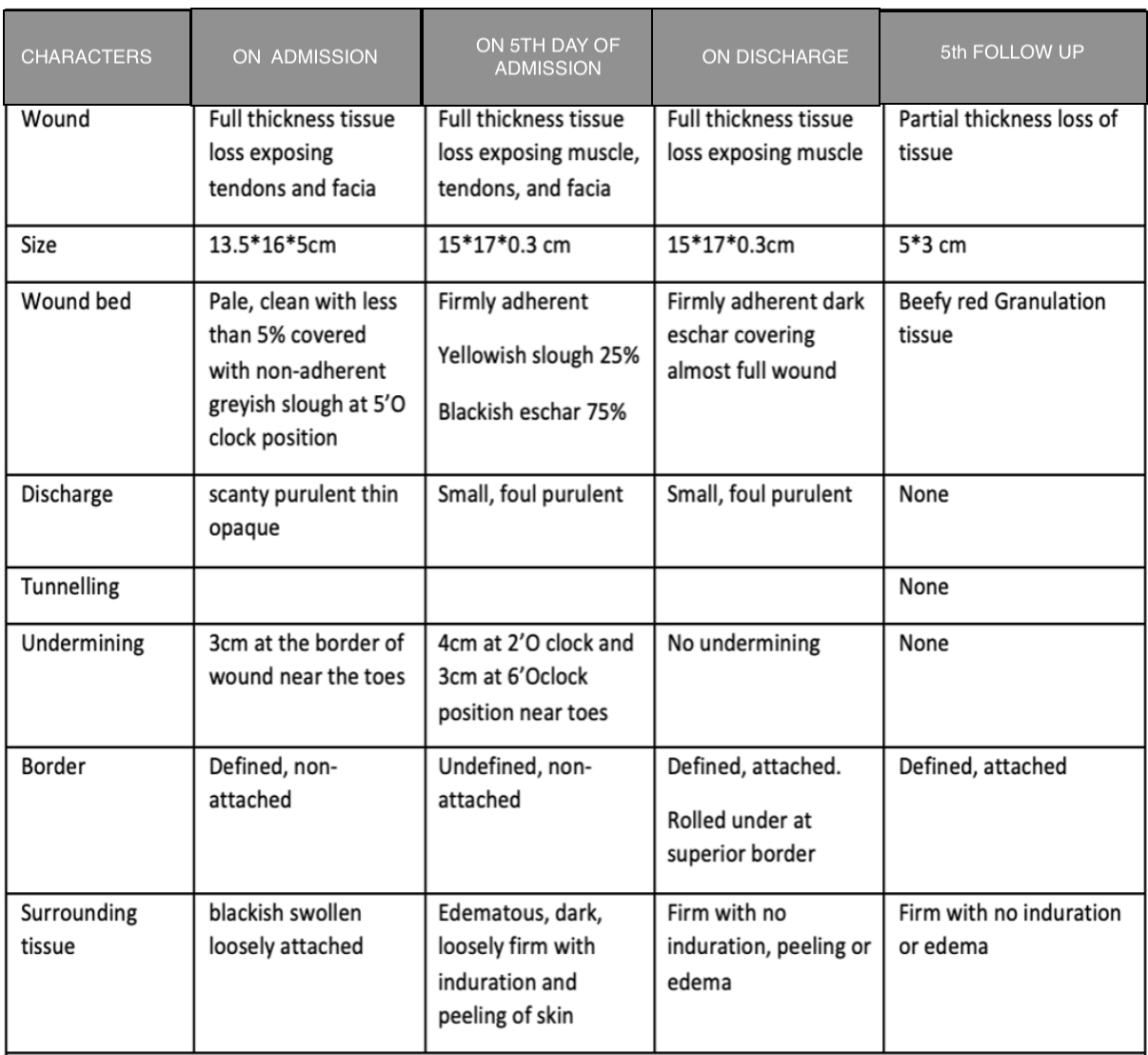
Table 1. Symptoms improvement -date wise observation
Clinician-based assessment; The patient was given treatment for duṣtavraṇa and was discharged after 38 days with better blood glucose control, tendons and facia covered with muscle, reduced induration, undermining and pedal oedema. With proper medications and regular follow ups the wound was healed and covered with healthy skin in around 5 months.
Patient-assessed; Not relevant
Images were taken during treatment to assess the outcome of the treatment.
Image 5. Wound appearance during treatment dated 21 and 26th July, 27th December 2017 in order

Image 6. Wound appearance after the treatment dated 4.3.2018 and 11.8.2018 in order


Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- Photographs taken before and after treatment were the primary assessment criteria.
Adverse and unanticipated events; None reported
DISCUSSION:
Diabetic foot ulcer has to be managed carefully, as there are many factors like the intensity of spread and sugar control that will affect ho the treatment works. In this case report, the patient was advised to do below knee amputation to save the limb, but she refused and opted for ayurveda. The physician followed the line of treatment of Vrana, Shopha and Vidradhi. Thus she could avoid amputation of her leg.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE HOME MESSAGES
In this case report, it was observed that DFI was treated successfully with ayurvedic intervention and below knee amputation could be avoided. Need of amputations, perioperative morbidity, mortality and socio-economic burden can be reduced with a proper multi-disciplinary approach in wound care management.
INFORMED CONSENT
Written consent obtained from patient for publishing of the case report in the Portal
ACKNOWLEDGEMENTS
None
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
- https://www.healthline.com/health/diabetic-foot-pain-and-ulcers-causes-treatments#causes
- https://www.uptodate.com/contents/management-of-diabetic-foot-ulcers
- https://my.clevelandclinic.org/health/diseases/21510-diabetic-feet#:~:text=Even with foot checks and careful blood glucose,and spreads too far, amputation may be necessary.
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Diabetic foot ulcer
ABOUT THE DISEASE:
Foot ulcers are a common complication of uncontrolled diabetes- improper diet and lifestyle. Ulcers are formed as a result of skin tissue breaking down and exposing the layers underneath. They’re most common under your big toes and the balls of your feet, and they can affect your feet down to the bones. All people with diabetes can develop foot ulcers, but good foot care can help prevent them. Treatment for diabetic foot ulcers varies depending on their causes.
The lifetime risk of a foot ulcer in patients with diabetes (type 1 or 2) may be as high as 34 percent. Diabetic foot ulcers are a major cause of morbidity, accounting for at least two-thirds of all nontraumatic amputations performed in the United States. Moreover, patients with diabetes with or without a diabetic foot ulcer have increased rates of depression, and expressing signs of depression is associated with an increased risk of diabetic foot ulcers. These observations illustrate the importance of prompt and appropriate treatment of foot ulcers in patients with diabetes.
Symptoms- One of the first signs of a foot ulcer is drainage from your foot that might stain your socks or leak out in your shoe. Unusual swelling, irritation, redness, and odors from one or both feet are also common early symptoms. The most visible sign of a serious foot ulcer is black tissue (called eschar) surrounding the ulcer. This forms because of an absence of healthy blood flow to the area around the ulcer. Partial or complete gangrene, which refers to tissue death due to infections, can appear around the ulcer. In this case, odorous discharge, pain, and numbness can occur. Signs of foot ulcers are not always obvious. Sometimes, you won’t even show symptoms of ulcers until the ulcer has become infected.
Causative factors:
Ulcers in people with diabetes are most commonly caused by:
- poor circulation
- high blood sugar (hyperglycemia)
- nerve damage
- irritated or wounded feet
Nerve damage is a long-term effect and can lead to a loss of feeling in your feet. Damaged nerves can feel tingly and painful. Nerve damage reduces sensitivity to foot pain and results in painless wounds that can cause ulcers.
Diagnostic criteria: Basically, the history taking and clinical evaluation are the important diagnostic tools. Blood tests and swab test can be done as supportive investigations. The University of Texas (UT, San Antonio) in the United States introduced a clinical classification system for diabetic foot wounds that evaluates wound depth, the presence of infection, and peripheral arterial occlusive disease for every category of the wound assessment. The UT system was the first diabetic foot ulcer classification to be validated [13]. This system updated the Wagner classification.
In this patient, the patient already came in with the confirmed diagnosis. As a part of diagnosis, Ulcer-grading - IDSA infection severity-severe/PEDIS Grade-4: Wagner classification-Grade 3: DFIWS 10 item score and 8 item score showed 32 and 28 respectively, were assessed and documented.
Image 1. Discharge summary confirming the diagnosis and the previous treatment done- 25.6.2017
Images were taken before, during and after treatment to assess the wound healing.
Image 2. Baseline photo taken of the diabetic foot ulcer dated 5.7.2017
Image 3. Diabetic Foot Infection Wound Score assessed at baseline.
Prognosis: This depends on factors like, how early the wound was found, presence and extent of spread of an infection, and efficacy of the treatment provided. If the infection has spread very far and deep, then amputation may be necessary. In this case report, the patient is a 43 year old house wife who is a known diabetic since 7 years. She complained of post debride, fresh, full thickness wound over the dorsum of left foot since 3 days. Tenderness was present over lower 1/4th of tibia and calf muscles since more than 7 years, aggravated since 2 weeks. Pain and tenderness over central plantar surface of foot since 2 weeks. She underwent, Wound debridement on spinal anesthesia and prescribed a course of medicines. But as the wound was not showing any signs of healing, she was advised for a below knee amputation to save the limb.
Treatment: The first step in managing diabetic foot ulcers is assessing, grading, and classifying the ulcer. Classification is based upon clinical evaluation of the extent and depth of the ulcer and the presence of infection or ischemia, which determine the nature and intensity of treatment. To assess for ischemia, all patients with diabetic foot ulcers should have ankle-brachial index and toe pressure measurements.The management of diabetic foot ulcers, including local wound care, use of mechanical offloading, treatment of infection, and indications for revascularization.
Reference
- https://www.healthline.com/health/diabetic-foot-pain-and-ulcers-causes-treatments#causes
- https://www.uptodate.com/contents/management-of-diabetic-foot-ulcers
- https://my.clevelandclinic.org/health/diseases/21510-diabetic-feet#:~:text=Even with foot checks and careful blood glucose,and spreads too far, amputation may be necessary.
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Dusta vrana
ABOUT THE DISEASE:
The definition of Vrana is:
व्रण गात्र विचूर्णने व्रणयति इति व्रणह….(AH.Utt.25.22)
There is a destruction, break, rupture or discontinuity in the body tissue, it is called as Vrana.
वृणोति यस्मात् रूढे'अपि व्रनवस्तु न नश्यति ।आदेह धारणात्तस्मत्व्रणैत्युच्च्यते ॥
Susruta explains Vrana as that which retains the scar even after complete healing of the wound, and the imprint remains the entire life. (Su.Ci.1.6)
दोषैरधिष्ठितो दुष्टः…..
When it becomes the seat of the vitiated dosa then it is called as Dushta Vrana.
In Dushta Vrana, there is severe pain, profuse discharge having putrified smell, and irregular base and margin.
पूतिगन्धान् विवर्णाञ्च बहुस्रावान्महारुजः॥८३॥
Dushta Vrana is difficult to heal and heals very slowly in spite of the best efforts by Cikitsa Chatuspada.
Lakshanas of Dushta Vrana
तत्रातिसंवृतोऽतिविवृतोऽतिकठिनोऽतिमृदुरुत्सन्नोऽवसन्नोऽतिशीतोऽत्युष्णः
नगन्धात्यर्थदाहपाकरागवेदनावानिति पित्तेन, शेषाः कफेन; उन्मार्गी मुखात् मुखान्तरवान्, उत्सङ्गः कोटरः’ इति चक्रः; कृष्णरक्तपीतशुक्लादीनांवर्णानामन्यतमवर्णो भैरवः पूतिपूयमांससिरास्नायुप्रभृतिभिः पूर्णःपूतिपूयास्राव्युन्मार्ग्युत्सङ्ग्यमनोज्ञदर्शनगन्धोऽत्यर्थंवेदनावान्दाहपाकरागकण्डूशोफपिडकोपद्रुतोऽत्यर्थं दुष्टशोणितास्रावी दीर्घकालानुबन्धी चेतिदुष्टव्रणलिङ्गानि | (Su.Su 22/7)In this case report, the patient is a 43 year old female, complaining of post debride, fresh, full thickness wound over the dorsum of left foot since 3 days. Tenderness over lower 1/4th of tibia and calf muscles since more than 7 years aggravated since 2 weeks pain and tenderness over central plantar surface of foot since 2 weeks. The biomedical diagnosis is Diabetic foot ulcer. Though there is no direct correlation to this condition in Ayurveda, taking into consideration the medical history and clinical evaluation, the ayurvedic diagnosis made was dusta vrana.
Management of Vrana
Treatment varies depending on the type of vrana and the management is given till the complete removal of scar tissue. In the treatment of nija vrana, i.e., those ulcers which recur due to aggravation of doshas, Sushruta explained the 60 upakrama, Charaka explained 36 upakrama and Vagbhata mentioned 26 upakramas. Seven modalities of Vrana Vimlapana, Avasecana, Upanaha, Patana kriya, Shodhana, Ropana, Vaikritapaham are explained by Acarya Sushruta. Sapta upkrama are a principal line of treatment which is explained in detail as Shashti upakrama.
The physician planned a treatment aimed at treating vraṇa, vidradhi, ṣopha hara. The medicines given were ruksa, to induce the alleviation of inflammation. Improving the blood circulation was also an important target.
Treatment rationale: It is a classical symptom of involvement of pitta, dhātupāka. Ama was considered and medicines were selected which were pitta recaka, ṣroto ṣodhaka, vraṇa, viṣha and jvara hara. External application was changed observing the improvement as the treatment proceeded. Purana ghṛtam is said to have qualities to heal the condition. Mutton soup was prepared according to the condition, aiming to improve the general strength and anaemia. Sudden positive results were observed.
Reference
- Vagabhata, Astangasangraha, Atridev Gupta,Krishnadas Academy, Varanasi UP Ed., 1993; 846:225.35.
- Madhavakara, Madhavanidan With MadhukoshaCommentary By Vijayarakshita And Srikant Data,Vinal Madhukar Hindi Commentary By Dr.Brahmanand Tripathi Choukhamba SanskritSansthan, Varanasi, 520:
3. Traditional and contemporary appraisal of dushta vrana w.s.r to venous ulcers. Available from: https://www.researchgate.net/publication/324156242_traditional_and_contemporary_appraisal_of_dushta_vrana_wsr_to_venous_ulcers#fulltextfilecontent [accessed apr 01 2023].
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Jatyadi Ghrtam+ Bhrhatchagaladi Ghrtam + Tiktaka Ghrtam Ghrtam Required Quantity Vrana lepana 2017-07-03 - 2017-07-05 Jatyadi Ghrtam- Ashtanga Hridayam, Uttara sthana 25/67, Bhrhatchagaladi Ghrtam- Bhaishajya Ratnavali. Vatavyadi adhikara 232 - 256, Tiktakam Gh?tam- AH. Ci. 19/ 2- 7 Jatyadi Ghrtam+ Purana Ghrtam Ghrtam Required Quantity Vrana lepana 2017-07-10 - 2017-07-15 Manjishtadi Kashaya, Guggulutiktakam Kashaya, Nimbadi Kashaya + Kaishora guggulu Samyoga 15 ml Mixed with 60m ml warm water and 1 tablet 2017-07-29 - 2017-08-02 Manjishtadi Kashaya/Nimbadi Kashaya- Sahasrayogam. Kashaya Prakarana. Guggulutiktakam Kashaya- AH.Ci.21.57-60: Kaishora guggulu - Bhaishajya Ratnavali. Vatarakta cikitsa. Mulakadi Kashaya+ Kokilakshakam Kashaya+ Varanadi Kashaya+ Tiktakam Kashaya+ Candraprabha Vati Kashayam 15 ml With 60 ml of luke warm water on empty stomach twice daily with the tablet 2017-07-29 - 2018-08-02 Mulakadi Kashaya- Sahasrayogam Kashaya Prakarana: Kokilakshakam Kashaya- Bhaishajya Ratnavali. Vatarakta rogadhikara 27/13: Varanadi Kashaya- AH.Su. 15/21- 22, Tiktakam Kashaya- AH.Ci.19/ 2- 7, Candraprabha Vati- Sharngadhara Samhita. Madhyama Khanda 7/ 40- 49. Trayantyadi Kashaya+ Patolakaturohinyadi Kashaya+ Gorocanadi gutika+ Vilvadi gutika Kashayam 15 ml With 60 ml of luke warm water on empty stomach twice daily, with 1 tablet each 2017-07-10 - 2017-07-15 Trayantyadi Kashaya-Trayantyadi Kashaya- AH. Ci. 13.11- 12: Patolakaturohinyadi Kashaya- AH Su 15.15: Gorocanadi gutika- Vaidya yoga ratnavali- Gutika prakarana 77: Vilvadi gutika- AH.Utt. 36/ 84- 85 Aragvadhadi Kashaya+ Nimbadi Kashaya+ Mulakadi Kashaya+ Candraprabha Vati Kashayam 15 ml With 60 ml of luke warm water on empty stomach twice daily, with 1 tablet each time 2017-07-10 - 2017-07-15 Aragvadhadi Kashaya- AH.Su 15.17 Nalpamara+ Kupilu Kashaya Kashayam Required Quantity Kashaya Dhara 2017-07-16 - 2018-07-31 Anubhuta Yoga Manjishtadi Kashaya+ Guggulutiktakam Kashaya+ Punarnavadi Kashaya+ Kaishora guggulu Kashayam 15 ml With 60 ml of luke warm water on empty stomach twice daily with the tablet 2017-08-01 - 2017-08-04 Punarnavadi Kashaya-Bhaishajya Ratnavali 42/13: kai?oraguggulu- Sharangdhara Madhayama khanda- 7/70-81 Manjishtadi Kashaya+ Punarnavadi Kashaya+ Guggulutiktakam Ghrtam Kashayam 15 ml With 60 ml of luke warm water on empty stomach twice daily with 1 tablet 2017-08-19 - 2017-12-26 Aragvadhadi Kashaya+ Nimbadi Kashaya+ Mulakadi Kashaya+ Kaishora guggulu Kashayam 15 ml With 60 ml of luke warm water on empty stomach twice daily, with 1 tablet each time 2017-08-19 - 2017-12-26 Manibhadra leham+ Madhusnuhi leham Leha 10 gms With warm water at bedtime 2017-08-19 - 2017-12-26 Manibhadra leham- AH.Ci. 19/31-32: Madhusnuhi leham- Sahasrayogam, Lehaprakarana Aragvadhadi Kashaya+ Manjishtadi Kashaya+ Mulakadi Kashaya+ Kaishora guggulu Kashayam 15 ml With 60 ml of luke warm water on empty stomach twice daily, with 1 tablet each time 2017-12-27 - 2018-01-17 -
Outcome Measures
OUTCOME MEASURES
The 43 year old female patient complained of post debride, fresh, full thickness wound over the dorsum of left foot since 3 days. Tenderness over lower 1/4th of tibia and calf muscles since more than 7 years aggravated since 2 weeks. There is pain and tenderness over central plantar surface of foot since 2 weeks. She had tried wound debridement under anaesthesia and took a course of medicines, but there was no signs of the wound healing. She was a known diabetic since 7 years and is on medication. She was advised for a below knee amputation to save the limb.
Assessment: Subjective and objective parameters were assessed to analyse the outcome of the treatment.
Subjective parameters: The symptoms as proceeding through the treatment were tabulated. The size of the wound, wound bed, discharge, tunnelling, undermining, border and surrounding tissue were all assessed and tabulated.
Image 1. Wound assessment done charted datewise
Images were taken during treatment to assess the outcome of the treatment.
Image 1. Wound appearance during treatment datewise
Image 2. Wound appearance after the treatment dated 4.3.2018 and 11.8.2018 in order
Objective parameters: None were done.
-