Featured Case
-
Abstract
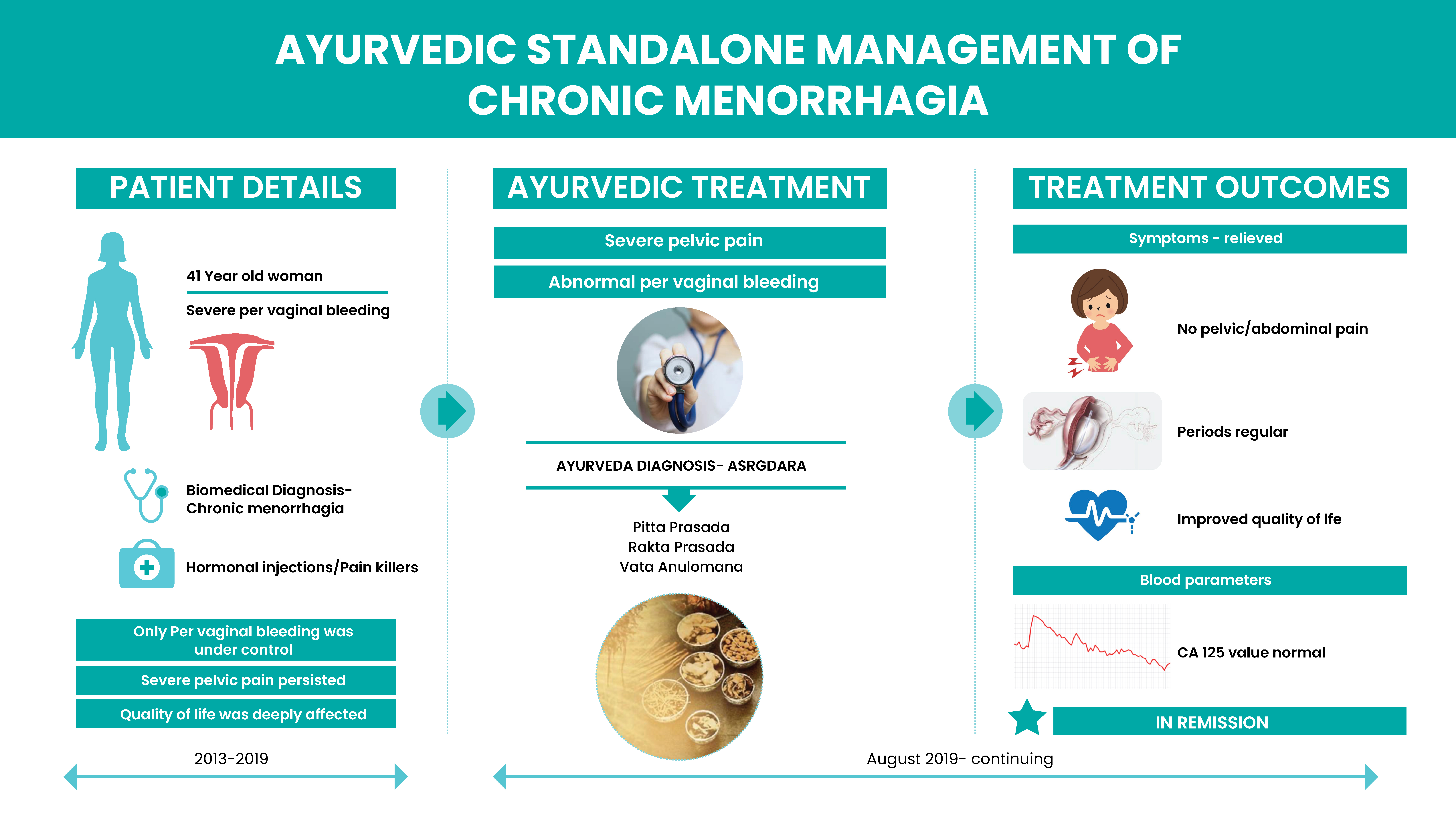
A Forty one year-old woman with menorrhagia and severe abdominal and pelvic pain for 5-6 years was nonresponsive to conventional medicine. Inspite of taking 5-6 pain killers /day and undergoing a course of Hormone injections, only her per vaginal bleeding could be controlled, but the pelvic pain persisted. Her allopathic doctor suggested hysterectomy, but she was not eligible due to internal organ adhesions. She stopped all alllopathic medicines and opted for Ayurveda. Dr Jyoti Joshi diagnosed this condition as Asrgdara and the treatment principle followed was that of Gulma cikitsa. To address the vayu apamarga, vasti was planned. On taking Ayurvedic medicines, the per vaginal bleeding is completely under control, and she got relief from the pelvic pain. Her quality of life significantly improved. She is still continuing the Ayurvedic medicines.
-
Summaries
-
Listen
-
Watch
-
View
-
Read

Menorrhagia can be defined as abnormally heavy or prolonged bleeding at menstruation. Menorrhagia is one of the most common gynaecologic complaints in women.
A Forty one year-old woman has been suffering from menorrhagia for 5-6 years. Since menarche at the age of 13, she always had a very painful menstruation. Now, there is heavy vaginal bleeding associated with severe abdominal and pelvic pain. Periods was always irregular, prolonged (sometimes lasted 15 days), frequent: sometimes 3-4 times in a month. Despite taking 5-6 pain killers/day and hormonal injections prescribed by her general physician, only her per vaginal bleeding could be kept under control, but the pelvic pain persisted. In 2018, as the vaginal bleeding increased, she was taken up for hysterectomy. During Exploratory laparotomy, adhesion of internal organs were diagnosed. So, hysterectomy could not be done. All the specialist she consulted in Mumbai and Hyderabad suggested that until menopause the condition must be managed with pain killers and hormonal injections. So, she decided to stop the allopathic medications and consulted Dr Jyoti Joshi who diagnosed this condition as Asrgdara. The treatment principle followed was that of Gulma Cikitsa. Vasti was administered to correct the Vayu Apamarga. The patient is on regular ayurvedic treatments since 2 years (22nd Aug 2019 onwards) and is still continuing them. Her period is regular and normal, with no abdominal or pelvic pain. This has boosted her up psychologically also. Her blood parameters are satisfactory.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Stand-alone Ayurvedic management of chronic menorrhagia associated with severe pelvic pain- A Case Report
ABSTRACT
A 41-year-old woman with menorrhagia1 and severe abdominal and pelvis pain for 5-6 years nonresponsive to conventional medicine, and not eligible for hysterectomy due to internal organ adhesions, opted for Ayurveda. Dr Jyoti Joshi diagnosed this condition as Asrgdara [2] and the treatment principle followed was that of Gulma cikitsa and to address the vayu apamarga, vasti was planned. Taking Ayurvedic medicines, the per vaginal bleeding is under control, and she got relief from the pelvic pain. She is continuing the Ayurvedic medicines.
KEYWORDS
Ayurveda, Chronic menorrhagia, Adhesions, Asrgdara
INTRODUCTION
Menorrhagia can be defined as abnormally heavy or prolonged bleeding at menstruation. Menorrhagia is one of the most common gynaecologic complaints. The causes of menorrhagia can be Hormone imbalance, Dysfunction of the ovaries, Uterine fibroids, Polyps, Adenomyosis, Intrauterine device, Pregnancy complications, Cancer, Inherited bleeding disorders, Medications, Other medical conditions. The clinical evaluation is the basic diagnostic criteria but to understand the underlying cause, blood investigations and imaging will be suggested. The prognosis varies depending upon the cause. A mere hormonal imbalance can be managed with medicines but underlying anatomical causes can be difficult to treat.
PATIENT INFORMATION
A 41-year-old female patient consulted Dr Jyoti Joshi with the presenting complaints of severe bleeding per vagina for 5-6 years, along with severe cervical and lower abdominal pain. The patient always felt very weak.
Medical History: The patient attended puberty at the age of 13. Since then, she always has very painful menstruation. For 5-6 years, there is heavy vaginal bleeding with severe abdominal and cervical pain. Her periods were always irregular, prolonged (sometimes lasted 15 days), sometimes 3-4 times in a month. She consulted a Specialist and was taking 5-6 painkillers/day to tolerate the pain. Despite taking pain killers, she did not get relief. In 2018, as the bleeding increased, she was taken up for hysterectomy. During open surgery, adhesions of internal organs were diagnosed. So, hysterectomy could not be done. All the specialist she consulted in Mumbai and Hyderabad believed until menopause the condition has to be managed with pain killers and hormonal injections. For 1 year, she tried allopathic medicines, the bleeding could be controlled, but severe abdominal and pelvic pain persisted, and the CA 125 value was increasing. Then she decided to stop the allopathic medications and consulted the Ayurvedic doctor and is taking regular ayurvedic treatments for 2 years (from 22nd Aug 2019). Past History- Married in 2001, 1 healthy male child C section (2002). Natural conception. Full term pregnancy. Surgical History: Gall bladder removed due to gall stones (2017); Exploratory laparotomy done 12/11/2018.
Psychosocial History: Mentally disturbed due to her illness.
PHYSICAL EXAMINATION
P/A - tenderness present at left iliac region. Patient is menstruating. PV- Uterus is bulky, fornix is clear.
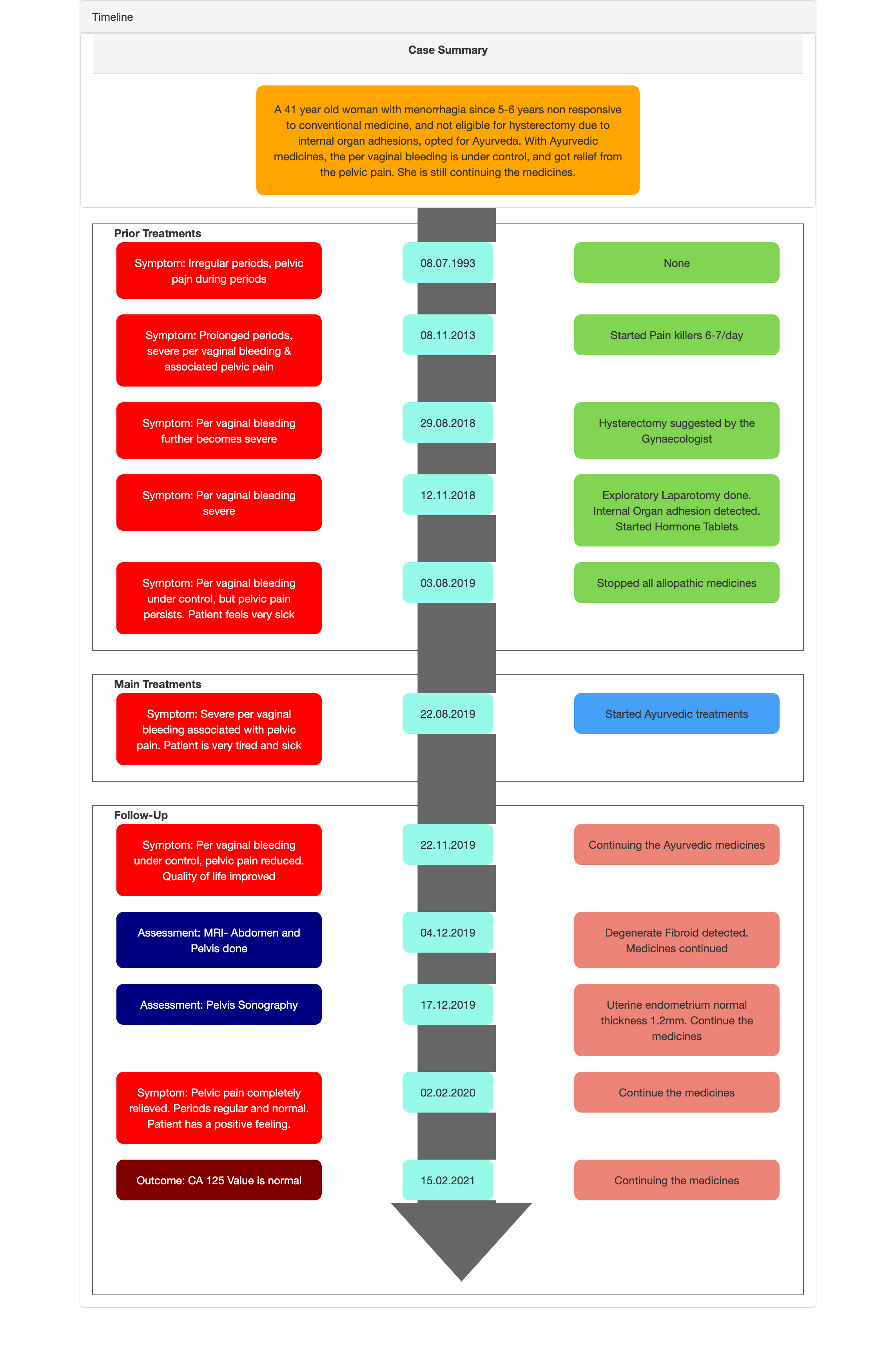
TIMELINE
Image 1. Timeline attached below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The clinical evaluation is the basic diagnostic criteria but to understand the underlying cause, blood investigations and imaging will be suggested. In this patient, the diagnosis was confirmed with imaging.
Date
Imaging done
Impression
8.11.18
USG abdomen & pelvis
Bulky uterus and uterine fibroid
12.11.18
Exploratory Laparotomy
Anteriorly: bladder stuck up to fundus, colon adhered to anterior fundal, posterior and broad ligament could not be separated. Small bowel adhered to right broad ligament.
17.11.18
Histopathology (Uterus)
No malignancy detected
June 2019
MRI Abdomen & Pelvis
Focal and diffuse adenomyosis of uterus
19.11.2019
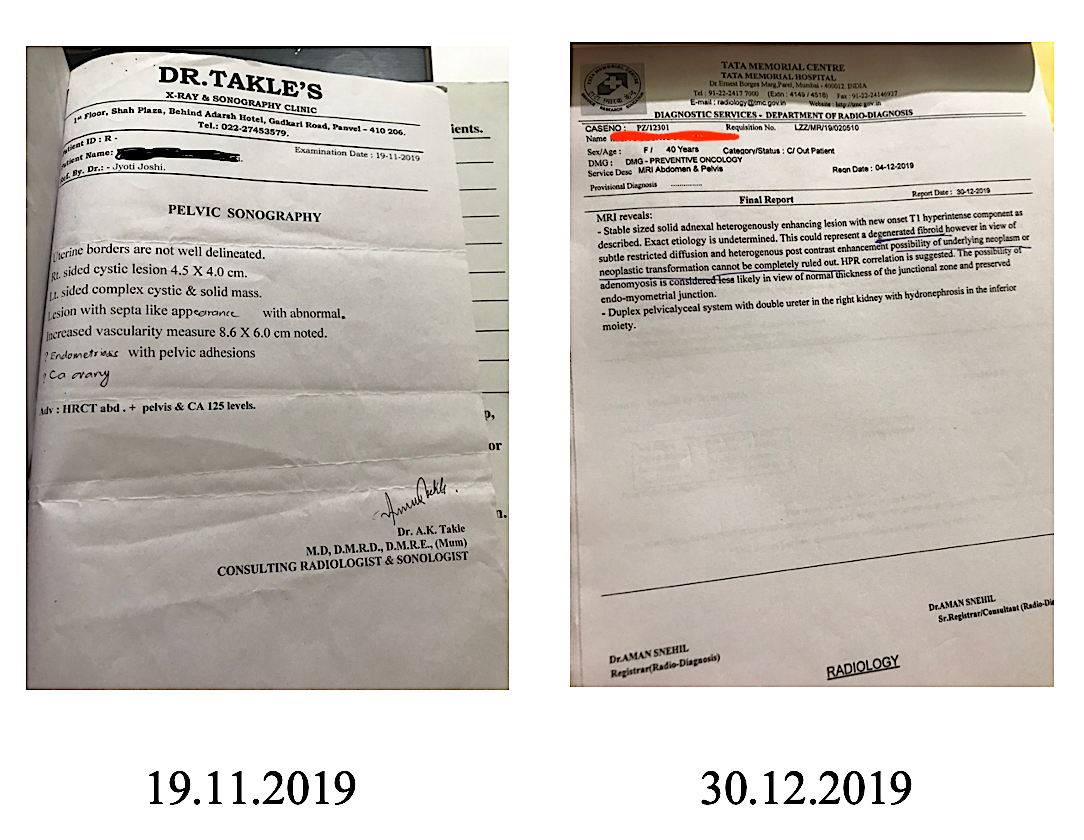
Pelvic sonography
Endometriosis. CA Ovary?
4/12/2019
MRI Abdomen & Pelvis
Degenerate fibroid
17.12.2019
MRI Abdomen & Pelvis
Uterine endometrium - normal thickness 1.2mm.
Reports confirming the diagnosis:
Image 2. Documents confirming the diagnosis. Exploratory Laparotomy 2018, follow up conventional medicines attached below
CA Values before starting the ayurvedic treatments:
Image 3. CA 125 value recorded in 2018 attached below
Ayurvedic Assessment was done based on the clinical evaluation by the ayurvedic physician.
Differential Diagnosis- This does not apply as the patient came in with a definite diagnosis.
Prognosis: The prognosis varies depending upon the cause. A mere hormonal imbalance can be managed with medicines but underlying anatomical causes can be difficult to treat. As this patient had internal organ adhesions, hysterectomy could not be done. The disease could only be managed symptomatically.
THERAPEUTIC INTERVENTION
See the Tab 'Treatment Details'
FOLLOW-UP AND OUTCOMES
The patient is still continuing the Ayurvedic medicines and the treatment.
Clinician-based assessment: Subjective and Objective parameters were analysed. The per vaginal bleeding is under control without the consumption of pain killers or hormonal injections. She got relief from the severe pelvic and abdominal pain. She is feeling energetic and confident now. The CA 125 (15/2/2021) reduced to 37U/ml, and the Hb is stable.
Image 4. CA 125 Values during and After Treatment attached below
Image 5. Images taken during Treatment- Pelvic Sonography and MRI Abdomen and Pelvis attached below
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By observation.
Adverse and unanticipated events: None reported
DISCUSSION:
Direct reference of Kasisa in gulma is mentioned in Rasaratna samucchayam. The uterus was bulky and resembled 8 weeks of pregnancy and was palpable at baseline. There was Vayu apam?rga, hence to correct this, vasti was decided. Vasti would also give relief from pain. Lodhra is basically stambhaka in nature. This along with sita jala is pittarakta prasadaka.
PATIENT’S PERSPECTIVE
Video of Patient narrative is available.
LEARNING POINTS/TAKE-HOME MESSAGES
The chronic case of menorrhagia associated with severe pelvic pain due to endometriosis/uterine adenomyosis, and increasing CA 125 value, hysterectomy was the suggested treatment of choice. But this could not be done due to internal organ adhesions and was suggested to manage the symptoms by taking pain killers and hormonal injections until menopause. With Ayurvedic treatments, she got relief from the symptoms, the blood parameters could also be normalized. The quality of life could be improved, and she stopped all the hormonal injections and pain killers. The patient is continuing the medicines.
In a condition like this, where surgery is the best treatment choice, but the patient is not eligible for surgery, Ayurveda can definitely be considered as an option.
INFORMED CONSENT
Written consent was obtained from the patient.
ACKNOWLEDGEMENTS
None
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
-
Nelson AL, Teal SB. Medical therapies for chronic menorrhagia. Obstet Gynecol Surv. 2007 Apr;62(4):272-81. doi: 10.1097/01.ogx.0000259228.70277.6f. PMID: 17371607.
-
Rathod Shweta N et.al. Review on ayurvedic management of asrgdara (menorrhagia): IJHSR. Vol 10. Issue 1.
Image 1. Timeline of events
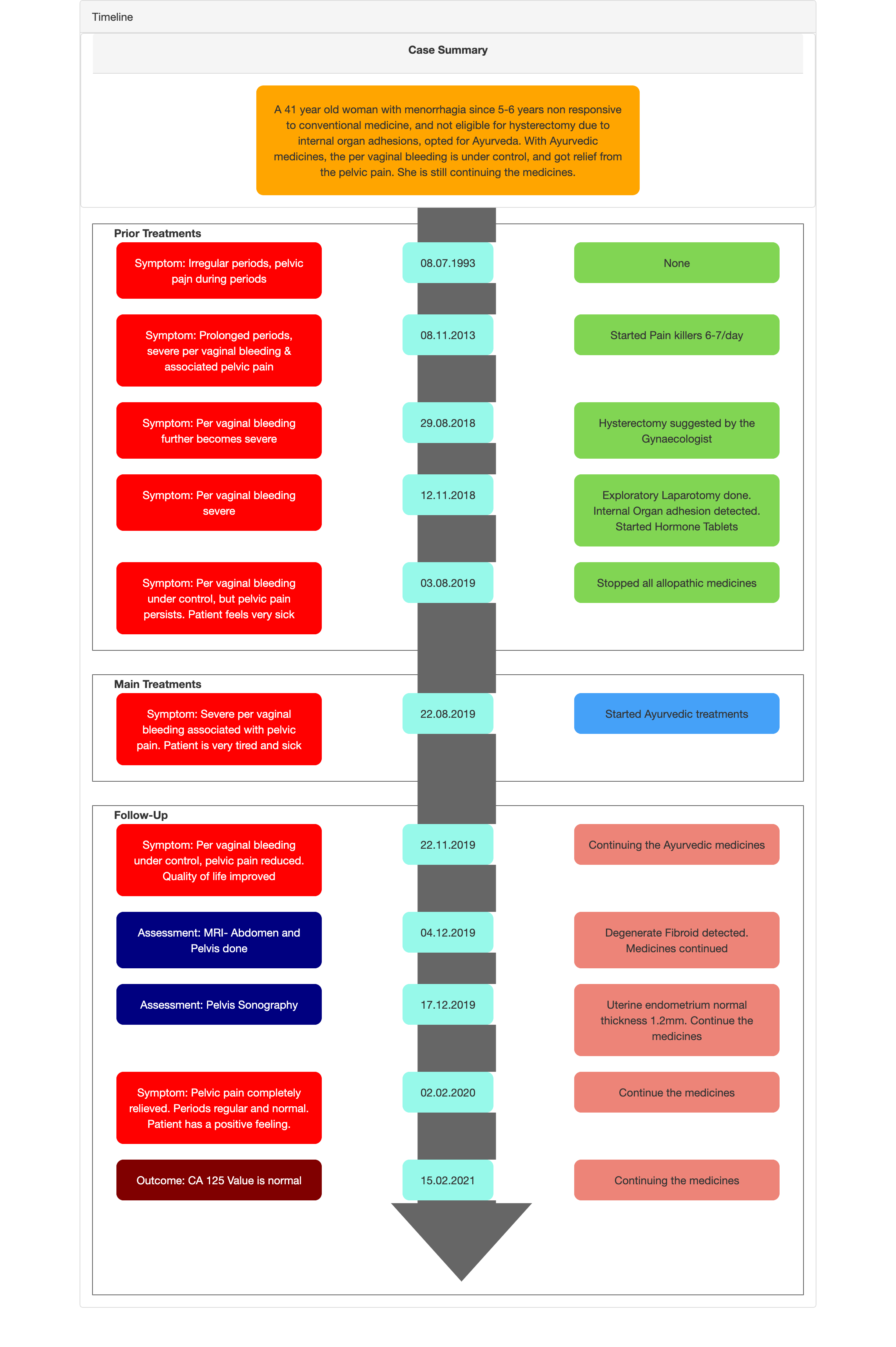
Image 2. Documents confirming the diagnosis. Exploratory Laparotomy 2018, follow up conventional medicines
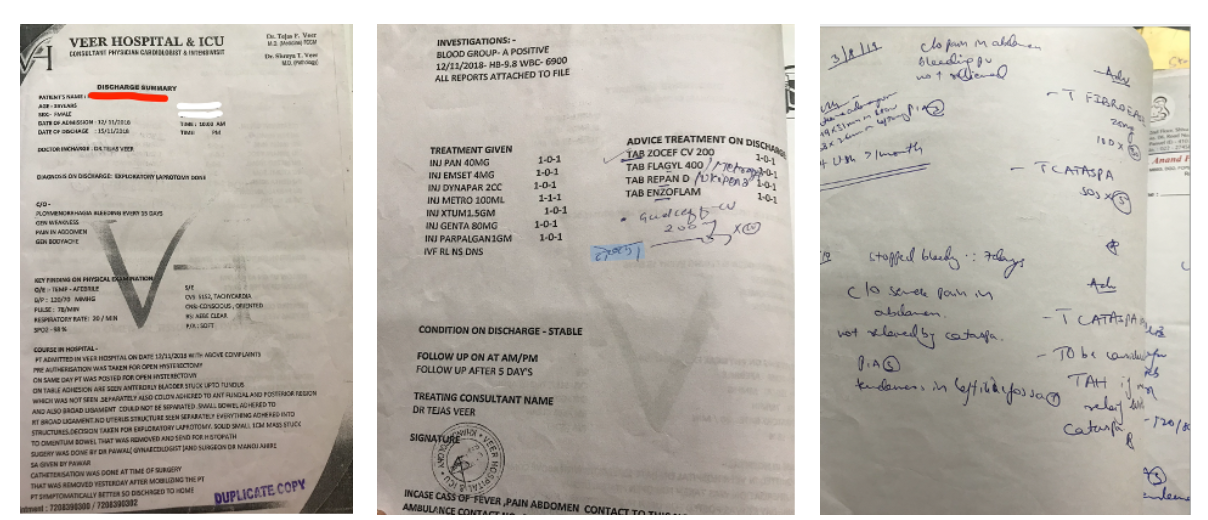
Image 3. CA 125 value recorded in 2018
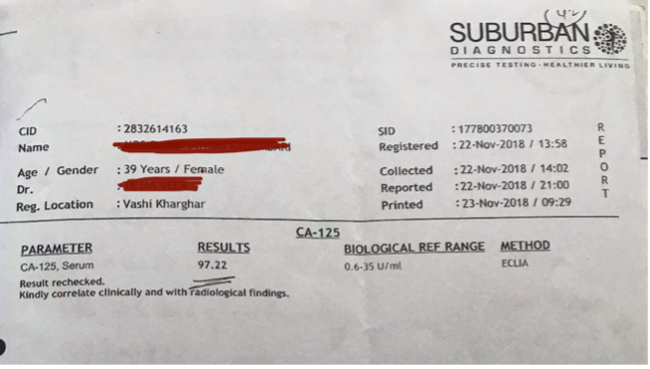
Image 4. CA 125 Values during and After Treatment
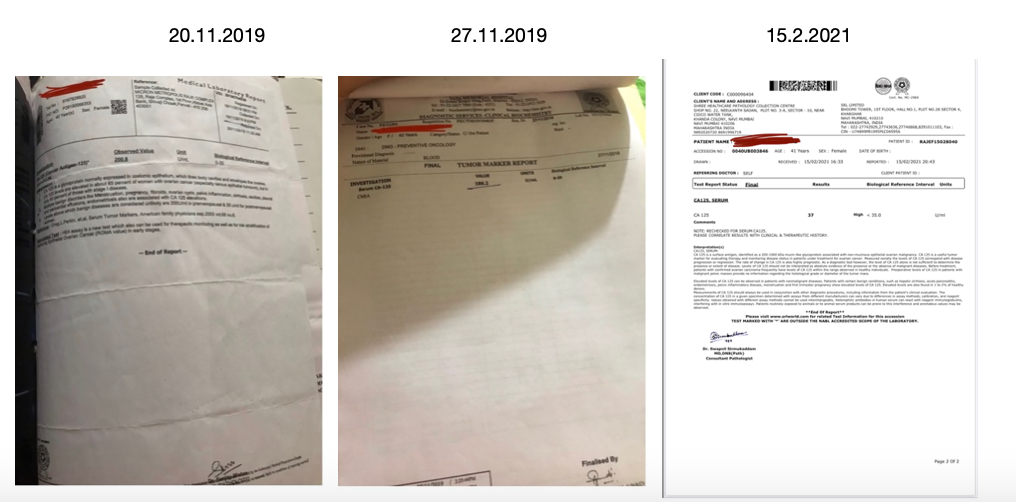
Image 5. Images taken during Treatment- Pelvic Sonography and MRI Abdomen and Pelvis
-
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Chronic menorrhagia
ABOUT THE DISEASE:
Menorrhagia can be defined as abnormally heavy or prolonged bleeding at menstruation. Menorrhagia is one of the most common gynaecologic complaints. The causes of menorrhagia can be Hormone imbalance, Dysfunction of the ovaries, Uterine fibroids, Polyps, Adenomyosis, Intrauterine device, Pregnancy complications, Cancer, Inherited bleeding disorders, Medications, Other medical conditions.
In this case report, Dr Jyoti Joshi treats a 41-year-old woman who has been suffering from chronic menorrhagia for 5-6 years. Since her menarche at the age of 13, she has always had a very painful menstruation. Her presenting symptoms were heavy vaginal bleeding with severe abdominal and cervical pain. On taking conventional medicines, the menstrual bleeding was under control, but the severe abdominal and cervical pain persisted. An exploratory laparotomy done revealed adhesions of internal organs, making it impossible to treat the condition. And her CA125 was constantly increasing, making it a health concern.
Diagnostic Criteria: The clinical evaluation is the basic diagnostic criteria but to understand the underlying cause, blood investigations and imaging will be suggested. In this patient, the diagnosis was confirmed with imaging.
Date
Imaging done
Impression
8.11.18
USG abdomen & pelvis
Bulky uterus and uterine fibroid
12.11.18
Exploratory Laparotomy
Anteriorly: bladder stuck up to fundus, colon adhered to anterior fundal, posterior and broad ligament could not be separated. Small bowel adhered to right broad ligament.
17.11.18
Histopathology (Uterus)
No malignancy detected
June 2019
MRI Abdomen & Pelvis
Focal and diffuse adenomyosis of uterus
19.11.2019
Pelvic sonography
Endometriosis. CA Ovary?
4/12/2019
MRI Abdomen & Pelvis
Degenerate fibroid
17.12.2019
MRI Abdomen & Pelvis
Uterine endometrium - normal thickness 1.2mm.
Diagnosis confirmation reports;
Image 1. Documents confirming the diagnosis- Exploratory Laprotomy , Follow up conventional medicine, Pelvic Sonography and MRI Abdomen and Pelvis attached below
CA 125 Values before starting the ayurvedic treatments:
Image 2. CA 125 Blood value attached below
Treatment: Normally, in this clinical condition the cause is addressed. In this patient, as she was not responding to the conventional medicines and even hormonal injections, hysterectomy was the final option. But she was not eligible for the procedure and was suggested to manage the symptoms until menopause by taking pain killers and hormonal injections.
Prognosis: The prognosis varies depending upon the cause. A mere hormonal imbalance can be managed with medicines but underlying anatomical causes can be difficult to treat. As this patient had internal organ adhesions, hysterectomy could not be done. The disease could only be managed symptomatically.
Image 1. Discharge Summary- Exploratory Laparotomy 2018. Follow up of conventional medicines
Image 2. CA 125 Blood value dated 22.11.2018
Pelvic Sonography dated 19.11.2019 and MRI Abdomen and Pelvis dated 30.12.2019
-
Ayurveda Diagnosis
AYURVEDIC DIAGNOSIS: Asrgdara
ABOUT THE DISEASE:
Any abnormality in the menstrual cycle that leads to excessive and prolonged uterine bleeding can be correlated as Asrgdara in Ayurveda. The word Asrgdara is made up of two words ie. asrg and dara. ‘Asrg’ means ‘rakta/raj’ and ‘dara’ means continuous/excessive flow. According to Caraka, the disease in which there is an excessive flow of raja is called ‘asrigdara’. Acarya Sushruta and Madhava have mentioned general bodyache, weakness, giddiness, mental confusion, feeling of darkness, dyspnoea, thirst, burning sensation, delirium, anaemia, drowsiness and convulsion, disorders of vata are symptoms associated with excessive per vaginal bleeding. The causative factors of asrgdara are psychological, improper food and activities. Caraka describes primarily food habits that cause emaciation or obesity and pelvic congestion as causative factors. Madhava, Bhavprakasha and Yogratnakar included psychological and viharajanya causes, which produce vasomotor disturbances, and chronic inflammation that can lead to abnormal uterine bleeding.
In this case report, Dr Jyoti Joshi treats a 41-year-old woman who has been suffering from chronic menorrhagia for 5-6 years. Since her menarche at the age of 13, she has always had a very painful menstruation. Her presenting symptoms were heavy vaginal bleeding with severe abdominal and cervical pain. On taking conventional medicines, the menstrual bleeding was under control, but the severe abdominal and cervical pain persisted. An exploratory laparotomy done revealed adhesions of internal organs, making it impossible to treat the condition. And her CA125 was constantly increasing, making it a health concern.
Diagnostic Criteria: Diagnosis is based on clinical evaluation by the physician and the previous reports pertaining to the clinical condition.
Treatment: Asrgdara is one of the diseases affecting the garbhashaya. Normal menstrual flow can be attributed to the proper movement of apanavayu. Apanavayu in its normal form performs the function of excretion of body constituents like vit, mutra, shukra and artava in the downward direction. The vitiated apanavayu will also cause vitiation in the artava. There are lots of single drugs and formulations in Ayurveda that are very effective in normalising the apanavayu and controlling the menstrual bleeding. Vasti is an good choice of treatment, ie Uttara vasti as it pacifies vata and can thus gives relief from symptoms like cervical and abdominal pain.
Treatment rationale and principle of the physician: Direct reference of kasisa in gulma is mentioned in Rasaratna samucchayam. The uterus was bulky like 8 weeks and palpable at baseline. Vayu apamarga was identified as the causative factor, so vasti was decided. Lodhra is basically stambhaka in nature. This combined along with sita jala is pittarakta pras?daka.
Prognosis: Tridoshaja and presence of associated symptoms like Trushna, Daha, Jwara, Daurbalyata, Swasa and Vataja rogas are considered as asadhya. In this patient, the disease was chronic and severe, making it asadhya. But with appropriate treatments, the physician was able to manage the condition.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Lodhra Curna Required Internal 2019-08-22 - 2021-02-02 Bhishak Yukti Lodhra Curna Required External application as Lepa on the vagina and lower abdomen 2019-08-22 - 2021-02-02 Bhishak Yukti Kasisadi Tailam 50 Anuvasana 2019-08-22 - 2021-02-02 Susruta Samhita.Cikitsa.6.12 -
Outcome Measures
OUTCOME MEASURES:
This 41-year-old female patient, had been suffering from chronic menorrhagia since her menarche, but is very severe for 5-6 years. In spite of trying conventional medicine for years, she did not get relief from her symptoms: irregular bleeding per vagina, severe cervical and abdominal pain, fatigue and being worried all the time. Hysterectomy was suggested but could not be done, due to internal organ adhesions. She was advised to continue the pain killers and hormonal injections to manage her symptoms until her menopause. So she stopped all the modern medicines and opted for Ayurveda.
The outcomes were measured by assessing the subjective and objective parameters. Subjective assessment: she got complete relief from severe cervical and abdominal pain. Even after stopping her pain killers and hormonal therapies, she has no abnormal menstrual bleeding. She is emotionally stable now and feels energetic and happy.
Objective parameter: During treatment, the CA 125 value was monitored, and repeated scans were taken to assess the condition. High CA 125 values are associated with many pathological conditions, but since this patient has endometriosis, this is a concern and is at risk for cancer. At baseline, the value was high. The patient is continuing the medications.
Image 1. CA 125 values - During and after Ayurvedic Treatment attached below
Image 2. Pelvic Sonography and MRI Abdomen and Pelvis during Ayurvedic Treatment attached below.
DISEASE MODIFYING EFFECT- In remission: The patient must continue the ayurvedic medicines because endometriosis could not be directly managed due to the internal organ adhesion. Diet and lifestyle restrictions are advised to be strictly followed.
Image 1. CA 125 Values recorded during and after treatment
Image 2. Pelvic Sonography and MRI Abdomen and Pelvis during and after treatment
-