Featured Case
-
Abstract
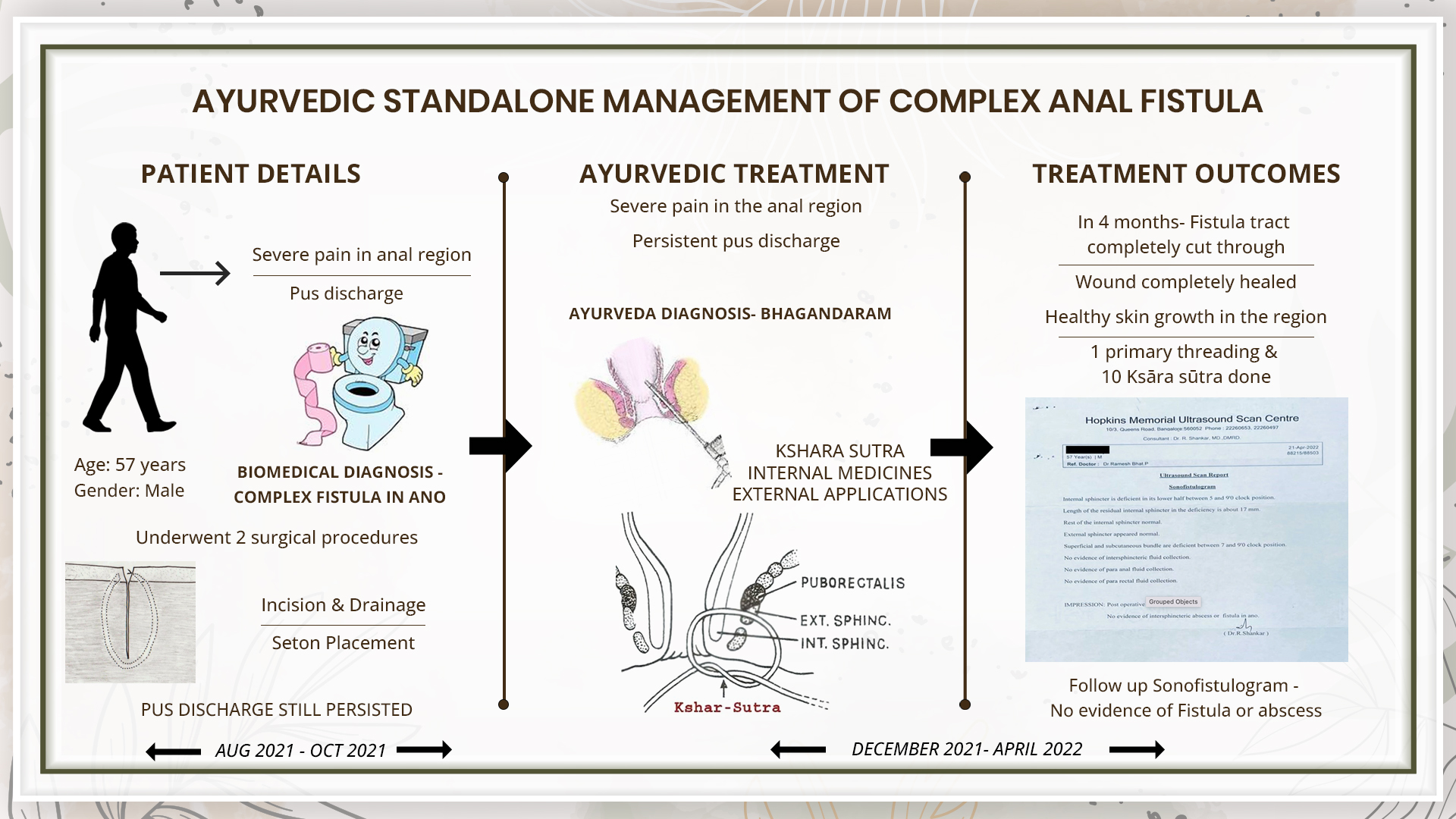
A 57-year-old male patient presented with complaints of severe pain in anal region associated with pus discharge for 2 years. He consulted an allopathic doctor and based on the MRI fistulogram, the biomedical diagnosis was made as posterior complex anal fistula. He underwent two surgical procedures the first procedure was Incision and drainage of ischiorectal abscess, and the second procedure was Seton replacement. The patient did not get satisfactory outcome. So he consulted Dr Ramesh Bhat for ayurvedic management. This was diagnosed as Bhagandara. The primary treatment followed was Ksharasutra supported by internal medications. After undergoing Ksharasutra treatment for 4 months- the thread changed once 1 week, the pus discharge completely stopped and a repeat sonofistulogram showed no evidence of fistula in ano. The patient got complete relief from his symptoms and the medicines were stopped. This case report narrates the successful standalone ayurvedic management of a case of complex anal fistula in a patient who had already tried 2 surgical procedures but did not get complete relief.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 57-year-old male patient presented with complaints of severe pain in anal region associated with pus discharge for 2 years. He consulted an allopathic doctor and based on the MRI fistulogram, the biomedical diagnosis was made as posterior complex anal fistula. He underwent two surgical procedures the first procedure was Incision and drainage of ischiorectal abscess, and the second procedure was Seton replacement. The patient did not get satisfactory outcome. So he consulted Dr Ramesh Bhat for ayurvedic management. This was diagnosed as Bhagandara. The primary treatment followed was Ksharasutra supported by internal medications. After undergoing Ksharasutra treatment for 4 months- the thread changed once 1 week, the pus discharge completely stopped and a repeat sonofistulogram showed no evidence of fistula in ano. The patient got complete relief from his symptoms and the medicines were stopped. This case report narrates the successful standalone ayurvedic management of a case of complex anal fistula in a patient who had already tried 2 surgical procedures but did not get complete relief.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Ayurvedic management of Complex anal fistula with rectal communication - A case report
Dr Ramesh Bhat
ABSTRACT
A 57-year-old male patient presented with complaints of severe pain in anal region associated with pus discharge for 2 years. He is a known case of type 2 diabetes mellitus and is under medication for the same. He had undergone two surgical procedures for his complaints. The first Procedure was Incision and drainage of ischiorectal abscess, and the second procedure was Seton replacement. The patient did not get complete relief from his symptoms. So he consulted Dr Ramesh Bhatt, who diagnosed this condition as Bhagandara. The primary treatment followed was Ksharasutra supported by internal medications. After undergoing Ksharasutra treatment for 4 months- the thread changed once every week, the pus discharge completely stopped and a repeat sonofistulogram showed no evidence of fistula in ano. The patient got complete relief from his symptoms and the medicines were stopped.
KEYWORDS
Fistula, ksharasutra, bhagandara, standalone, case report, ayurveda, primary threading
INTRODUCTION
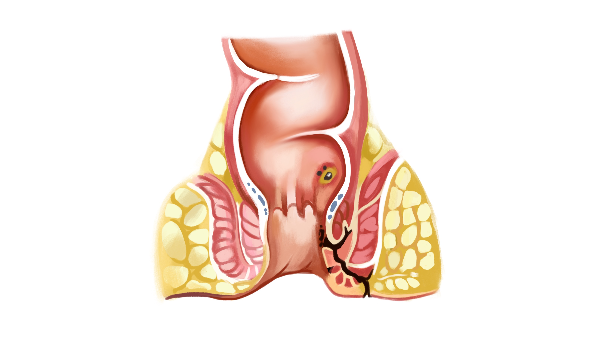
A fistula-in-ano or an Anal Fistula is an abnormal tract that is hollow or a cavity lined with granulation tissue connecting a primary opening located inside the anal canal to another opening called a secondary opening located in the perianal skin. These secondary tracts can be multiple and may have their origin from the primary opening. This is a painful condition that can disrupt the normal activities of an individual. The symptoms are pus or blood exudation from the non-healing abscess, painful defecation, signs of infection like fever may also be present.
Diagnostic criteria: Physical examination and medical history are the primary diagnostic criteria. If the pain is too severe or it is a high-level fistula, then investigations like endoscopic ultrasound or MRI will be prescribed to identify the fistula tract. Internal fistulas may be evaluated using barium contrast X-ray, MRI or CT scan. The internal opening of the fistula can be identified with a Fistula probe, Anoscope, Flexible sigmoidoscopy or Colonoscopy, or an injected dye solution. In this patient, the diagnosis was confirmed with clinical examination and with a MRI Fistulogram.
Prognosis & Treatment:
There are surgical and non-surgical options of treatment. Fistulotomy, Endorectal advancement flap and Ligation of the intersphincteric fistula tract are the most commonly followed surgical procedure in the treatment of Fistula. The non-surgical procedures include seton placement, fibrin glue and collagen plug. But these procedures may cause complications like sphincter muscle damage leading to the incontinence of the sphincter, rectal prolapse, faecal soiling, and anal stenosis. Even after complete excision of the tract, the chances of recurrence are still present.
PATIENT INFORMATION
A 57 year old male patient presented with complaints of severe pain over the anal region associated with pus discharge since 2 years. Patient consulted modern hospital and was advised for MRI fistulogram. The MRI findings reveals posterior complex anal fistula. He is a known diabetic and is on anti-diabetic medication.
Surgical History- Two surgical procedures in USA. First Procedure - Incision and drainage of ischiorectal abscess (12/8/2021). Second procedure – setons placement (21/10/2021).
No significant family/genetic/psychosocial history.
CLINICAL FINDINGS
Peri anus examination revealed induration over the right posterolateral region and two rubber setons were in situ. Digital rectal examination revealed induration and tenderness of anal mucosa at 6’O clock position at above the level of the anal valve. Peri anus skin exfoliation, edematous, chronic skin inflammation with active discharge through the external opening was observed.
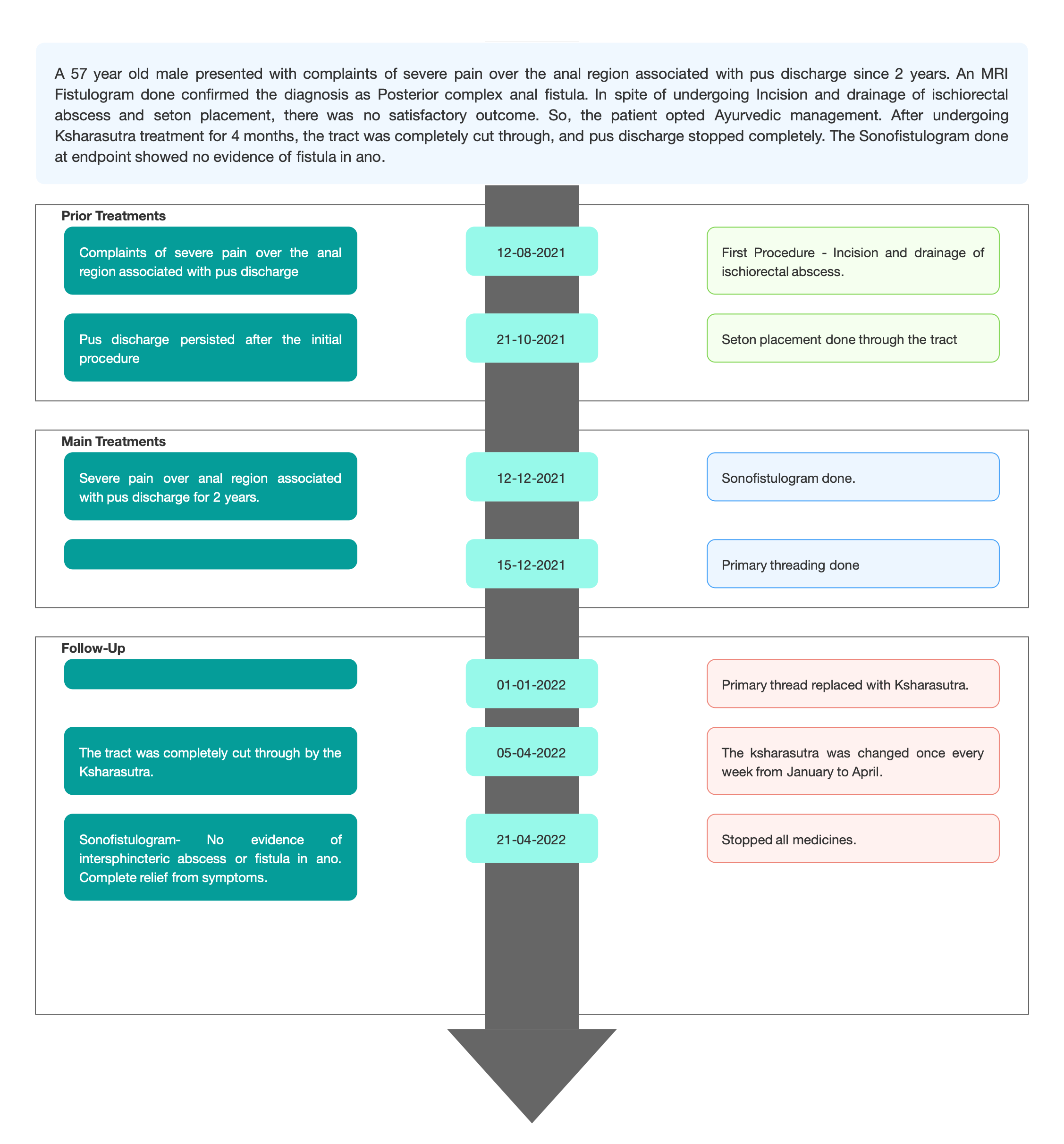
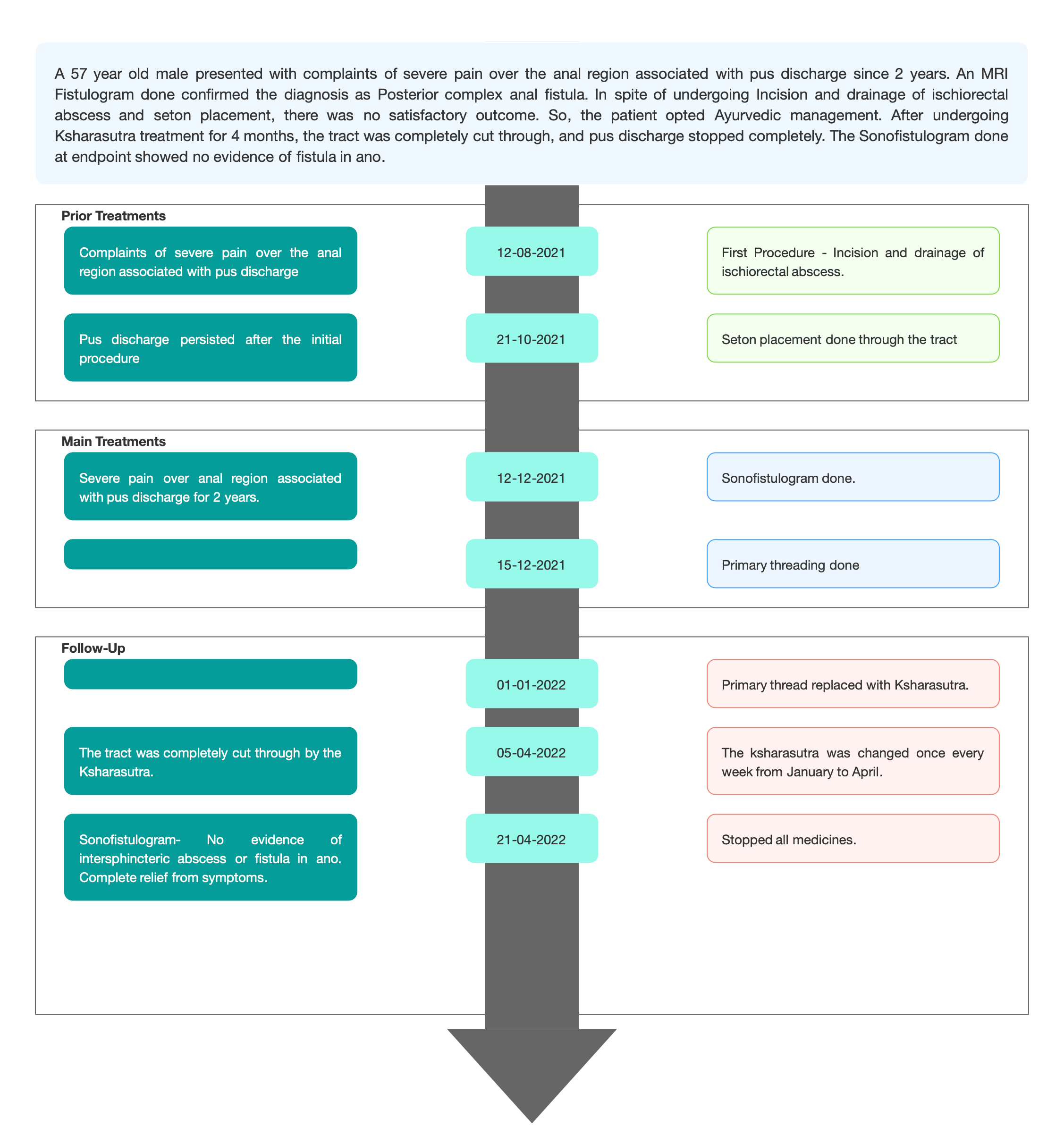
TIMELINE
Image 1. Timeline of events added below
DIAGNOSTIC ASSESSMENT
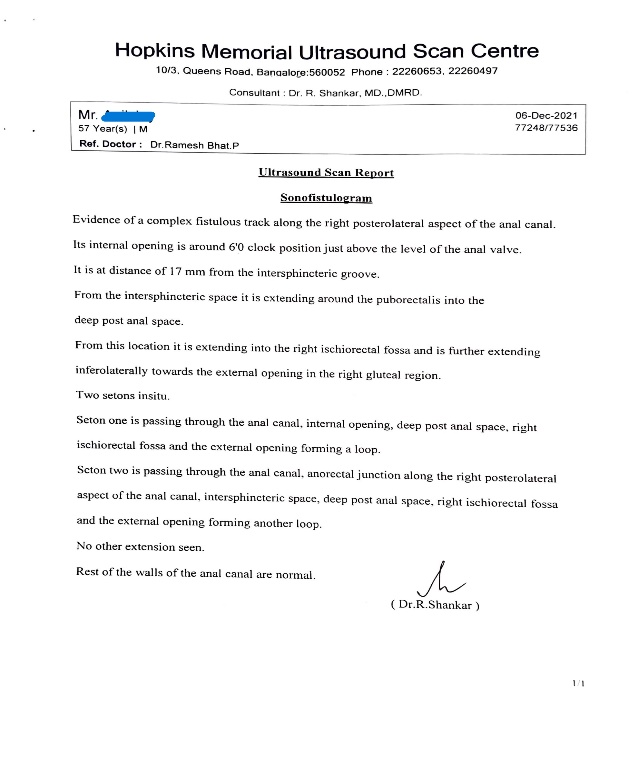
Modern Diagnostic parameter; The biomedical diagnosis was confirmed as Complex anal fistula with an MRI Fistulogram done in August 2021. (Reports not submitted). But on Ayurvedic consultation, December 2021, Sonofistulogram was done to confirm the diagnosis.
Image 2. Baseline Sonofistulogram dated December 2021 added below
Ayurvedic Assessment was done based on the presenting complaints and clinical evaluation. The treating physician confirmed the Ayurvedic diagnosis as Bhagandaram.
Differential Diagnosis- Vidradhi.
On the basis of previous treatment records and special Investigations, the physician diagnosed the condition as bhagandara.
Prognosis- There are surgical and non-surgical options of treatment. Fistulotomy, Endorectal advancement flap and Ligation of the intersphincteric fistula tract are the most commonly followed surgical procedure in the treatment of Fistula. The non-surgical procedures include seton placement, fibrin glue and collagen plug. But these procedures may cause complications like sphincter muscle damage leading to the incontinence of the sphincter, rectal prolapse, faecal soiling, and anal stenosis. Even after complete excision of the tract, the chances of recurrence are still present.
This patient had already undergone two surgical procedures in USA. First Procedure - Incision and drainage of ischiorectal abscess (12/8/2021). Second procedure – setons placement (21/10/2021). But the symptoms persisted and hence he opted for Ayurvedic management.
THERAPEUTIC INTERVENTION
Refer the tab ‘Treatment’ in the Portal.
FOLLOW-UP AND OUTCOMES
The patient had 15 follow ups, once every week to change the Kshama sutra and also for examination by the physician. One primary threading and 13 Ksharasutra were applied before the patient got a complete relief from his condition.
Clinician-based assessment; On examination, the wound had healed completely. There is no pain or pus discharge.
Patient-assessed; Not relevant
After undergoing one and half months of Ayurvedic treatment, there was a significant reduction in the symptoms- itching followed by bleeding observed rarely. After 5 months, the patient is completely free from all the symptoms. On examination, the skin is normal. There is no scaling or swelling. She is still continuing the Ayurvedic medicines.
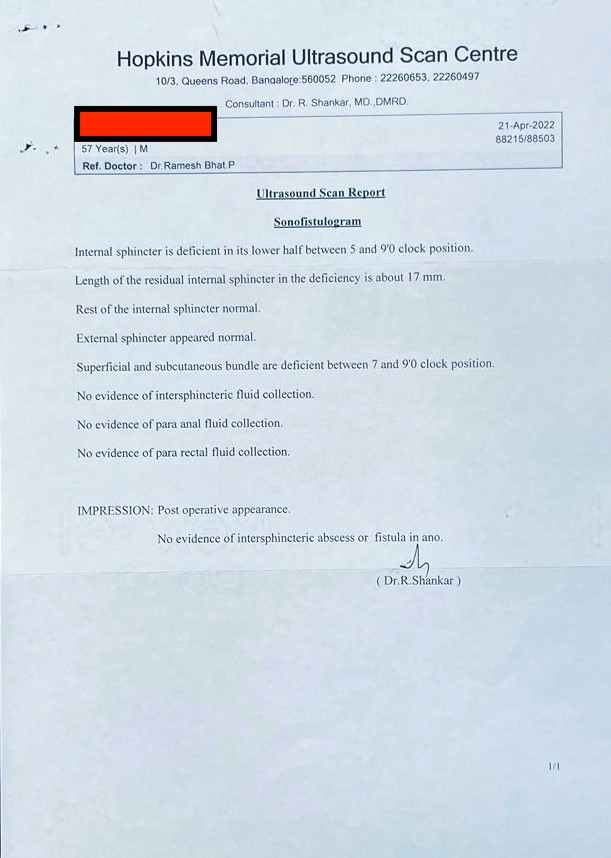
Image 3. Endpoint Sonofistulogram dated April 2022 added below
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- Sonofistulogram before and after ayurvedic treatment were the primary methods of assessment.
Adverse and unanticipated events; None reported
DISCUSSION ;
The patient had been suffering from complaints since 2 years. He had undergone 2 surgical procedures - Incision and drainage and Seton replacement 4 months back, but the pus discharge persisted. After undergoing Ksharasutra treatment for 4 months, pus discharge completely stopped. The primary treatment modality Ksharasutra helped in draining the tract and healing the wound completely. Internal medicines like Triphala guggulu and Gandhaka Rasayana were given to help the healing process.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE HOME MESSAGES
This case report narrates the successful management of a case of complex anal fistula in a patient who had already tried 2 surgical procedures but did not get complete relief. With 1 primary threading and 13 kshara supported with Ayurvedic medicines, the tract was completely cut through and healed. A follow-up Sonofistulogram revealed no evidence of fistula or intersphincteric abscess.
INFORMED CONSENT
Written consent obtained from patient.
ACKNOWLEDGEMENTS
None
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
1. Seow-Choen F, Nicholls RJ. Anal fistula. Br J Surg. 1992 Mar;79(3):197-205. doi: 10.1002/bjs.1800790304. PMID: 1555083.
2. Ahmad Mir, *Shaheen, & Kumar, P. H. (2017). Bhagandara and its management in Ayurveda: A conceptual study. International Journal of Ayurveda and Pharma Research, 5(8). Retrieved from http://ijaprs.com/index.php/ijapr/article/view/753
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Complex Fistula in Ano with rectal communication
About the Disease:
A fistula-in-ano or an Anal Fistula is an abnormal tract that is hollow or a cavity lined with granulation tissue connecting a primary opening located inside the anal canal to another opening called a secondary opening located in the perianal skin. These secondary tracts can be multiple and may have their origin from the primary opening. This is a painful condition that can disrupt the normal activities of an individual. The symptoms are pus or blood exudation from the non-healing abscess, painful defecation, signs of infection like fever may also be present.
Diagnostic criteria: Physical examination and medical history are the primary diagnostic criteria. If the pain is too severe or it is a high-level fistula, then investigations like endoscopic ultrasound or MRI will be prescribed to identify the fistula tract. Internal fistulas may be evaluated using barium contrast X-ray, MRI or CT scan. The internal opening of the fistula can be identified with a Fistula probe, Anoscope, Flexible sigmoidoscopy or Colonoscopy, or an injected dye solution. In this patient, the diagnosis was confirmed with clinical examination and with a MRI Fistulogram.
In this case report, a 57 year old male patient presented with complaints of severe pain over the anal region associated with pus discharge since 2 years. Patient consulted modern hospital and was advised for MRI fistulogram. The MRI findings reveals posterior complex anal fistula.
Image 1. Baseline Sonofistulogram dated 6th December 2021
Prognosis & Treatment:
There are surgical and non-surgical options of treatment. Fistulotomy, Endorectal advancement flap and Ligation of the intersphincteric fistula tract are the most commonly followed surgical procedure in the treatment of Fistula. The non-surgical procedures include seton placement, fibrin glue and collagen plug. But these procedures may cause complications like sphincter muscle damage leading to the incontinence of the sphincter, rectal prolapse, faecal soiling, and anal stenosis. Even after complete excision of the tract, the chances of recurrence are still present. Cryptoglandular anal fistula communicating secondarily to the rectum is a rare clinical condition. It is a challenge to treat such fistula without recurrence and without compromising anal function.
This patient had already undergone two surgical procedures in USA. First Procedure - Incision and drainage of ischiorectal abscess (12/8/2021). Second procedure – setons placement (21/10/2021). But the symptoms persisted and hence he opted for Ayurvedic management.
Reference
1. Seow-Choen F, Nicholls RJ. Anal fistula. Br J Surg. 1992 Mar;79(3):197-205. doi: 10.1002/bjs.1800790304. PMID: 1555083.
2. Ahmad Mir, *Shaheen, & Kumar, P. H. (2017). Bhagandara and its management in Ayurveda: A conceptual study. International Journal of Ayurveda and Pharma Research, 5(8). Retrieved from http://ijaprs.com/index.php/ijapr/article/view/753
-
Ayurveda Diagnosis
AYURVEDIC DIAGNOSIS: Bhagandaram
About the Disease:
Taking into consideration the clinical presentation, fistula-in-ano or an Anal Fistula can be correlated to Bhagandara in the Ayurvedic texts.
Acarya Susruta, explains the presence of a deep-rooted apakva pidaka within two angular circumferences of Guda pradesha associated with pain and fever is called Bhagandara pidaka. When it suppurates and burst open, then it is called Bhagandara. This is listed as one amongst the Ashtamahagada. The word ‘Bhaga’ relates to all the structures around the guda, including the vasti and yoni. The Dharana (discontinuity) in the region of Bhaga, Guda and Vasti with surrounding skin surface is called Bhagandara. Vaghbhata mentions the formation of a Vrana to the size of a pidika, 1 or 2 angula from the anus or inside the anus (Utt.28/12-14). Rakta and mamsa are the vitiated dushyas. This results in the formation of a sinus, associated with pus discharge in the region of anus, perineum and bladder.
गुदस्य हि अग़्गुले क्षेत्रेपार्श्वतः पिडकार्तिकृत् ।
भिन्ना भगन्दरो ञेय स च पञ्चविधो मतः ॥Ma.Ni.46.1Susruta explains 5 types of Bhagandara, but Vaghbhata has mentioned 8 types of Bhagandara. Depending upon the dos?a responsible for the pathology, the respective symptoms will be produced. Here, the physician has not identified the type of Bhagandara. The colour of the skin around the anus is recorded as normal and there is no inflammation observed. The type of pain - whether toda, bheda, or sphurana are also not specified. So, the exact type of Bhagandara cannot be pointed out.
Prognosis: All the types of Bhagandara are painful and troublesome and are Krcchrasadhya. The incurable types are sannipataja, agantuja, bhagandara located in pravahini and sevani layer of the guda, and sataponaka in the kshina.
In this case report, the 57 year old male patient presented with complaints of severe pain over the anal region associated with pus discharge since 2 years. Though he had undergone two surgical procedures 4 months back, the symptoms persisted and hence he opted for Ayurvedic management.
Treatment:
Gada Nigraha (Utt.7/10-14) mentions different types of treatment depending on the avastha. They are:
- Bhagandara Pidika Cikitsa (Apakvavastha)
- Bhagandara Cikitsa (Pakvavastha)
In Bhagandara Pidika Cikitsa, the treatment modalities specifically mentioned are Apatarpana, Alepa, Parisheka, Abhyanga, Swedana, Vimlapana, Upanaha, Pachana, Vishravana, Snehana, Vamana and Virechana (Su.Ci.8.4). Rakta Mokshana, Kshara Karma and Agni Karma are the most common parasurgical procedures done in Bhagandara. Out of these, the Kshara sutra is a very successful treatment widely practised by Ayurvedic physicians for rapid healing, with no recurrence of the fistulous tract.
In this patient, Kshara sutra was the primary treatment modality, supported by internal and external therapies. 1 primary threading and 13 Ksharasutra were applied before the patient got a complete relief from his condition.
Treatment rationale of the physician:
The Ayurvedic parasurgical procedure Kshara sutra is the best treatment option for Bhagandaram. The recurrence of a fistulous tract treated with Kshara sutra is not yet reported. Hence this treatment was chosen supported by internal medication and external applications. The rationale for the specific treatment plan was tabulated as follows.Table 1. The medicine/therapy and the specific rationale for this treatment.
Medicines/Procedure
Rationale
Triphala guggulu
Anti inflammatory
Gandaka rasayanam
Enhances wound healing.
Fistulotomy and primary threading
Preparatory for the Kshara sutra application
Kshara Sutra Changing
Helped in gradual cutting and healing of the track.
Jatyadi Taila
Enhances wound healing.
Table 2. The dates of Kshara sutra application tabulated
DATE
KSHARA SUTRA APPLICATION
12/12/2021
Ayurvedic consultation
15/12/2021
Limited fistulotomy and primary threading
Second seton which was placed at the level of rectal mucosa was removed.1/1/22
Kshara sutra applied
8/1/22
Kshara sutra change
16/1/22
Kshara sutra change
24/1/22
Kshara sutra change
1/2/22
Kshara sutra change
9/2/22
Kshara sutra change
17/2/22
Kshara sutra change
25/2/22
Kshara sutra change
5/3/22
Kshara sutra change
13/3/22
Kshara sutra change
21/3/22
Kshara sutra change
29/3/22
Kshara sutra change
5/4/22
Kshara sutra change
21/4/22
Stopped all medicines
Reference
1. Ahmad Mir, *Shaheen, & Kumar, P. H. (2017). Bhagandara and its management in Ayurveda: A conceptual study. International Journal of Ayurveda and Pharma Research, 5(8). Retrieved from http://ijaprs.com/index.php/ijapr/article/view/753
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Triphala guggulu Tablet 2 Oral- with warm water once daily before food 2021-12-15 - 2022-04-20 Sharngadhara Samhita. Madhyama khanda.7/ 82- 83 Gandhaka rasayanam Tablet 2 Oral- with warm water before food, twice daily 2021-12-15 - 2022-04-20 Rasatarangini. 8/ 81 - 86 -
Outcome Measures
OUTCOME MEASURES
The 57 year old male patient presented with complaints of severe pain over the anal region associated with pus discharge since 2 years. Patient consulted modern hospital and was advised for MRI fistulogram. The MRI findings revealed posterior complex anal fistula. He underwent 2 surgical procedures 4 months back, but the condition persisted. So he opted for Ayurvedic management.
Assessment: Subjective and objective parameters were assessed to analyse the outcome of the treatment.
Subjective parameters: After 2 weeks of starting the treatment, the pain subsided. After 4 weeks, the pus discharge reduced. After 4 and half months, the Ksharasutra was removed laying open the remnant track. At this point, patient was completely relieved of pain and pus discharge. In the last follow up, the wound had healed completely.
Objective parameters: An endpoint Sonofistulogram was done that revealed- No evidence of intersphincteric abscess or fistula in ano.
Image 1. Endpoint Sonofistulogram dated 1.4.2022
-