Featured Case
-
Abstract
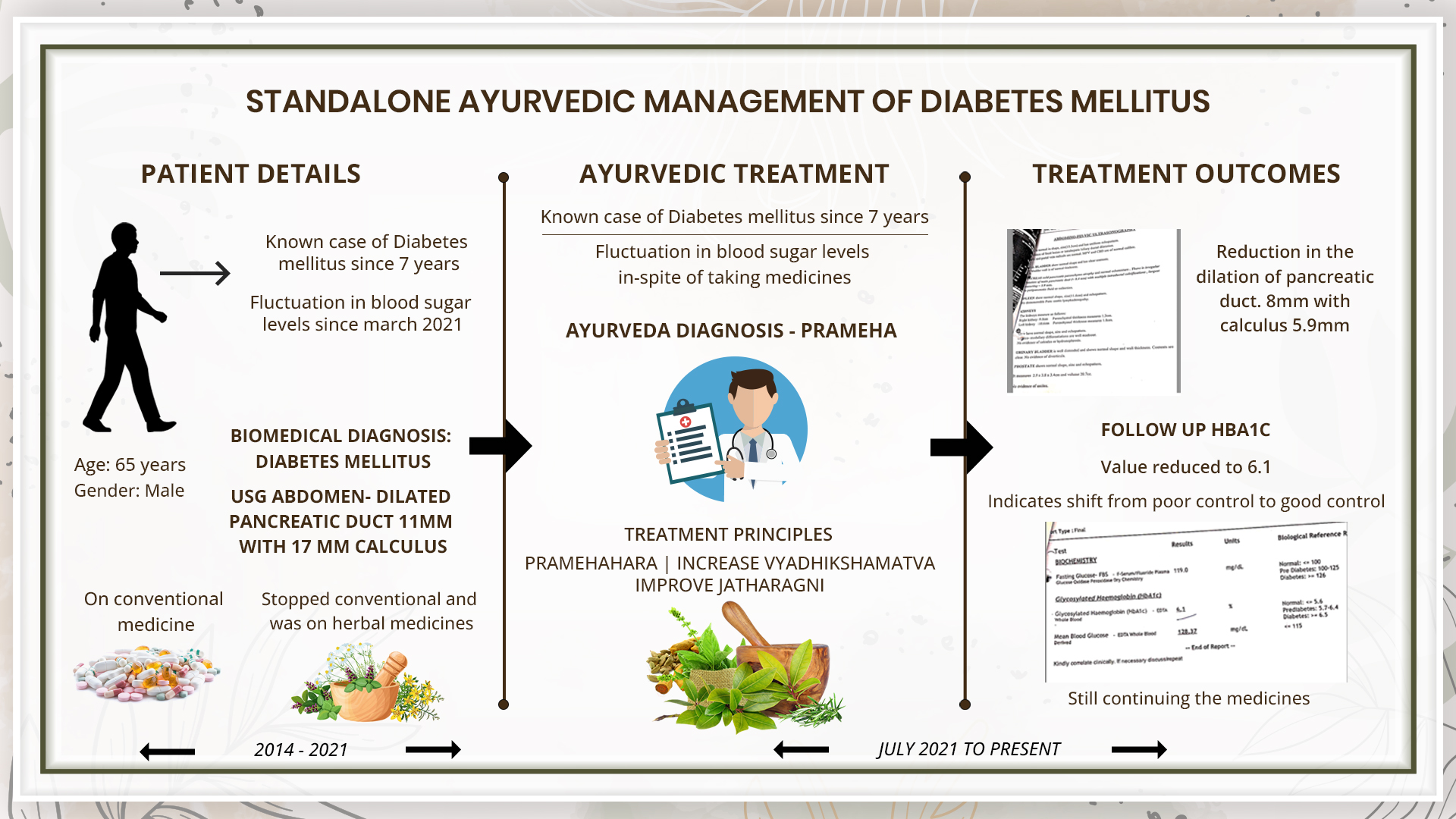
A 65-year-old male patient complained of fluctuation in blood sugar levels since March 2021. He is a known diabetic since past 7 years. Initially, he took allopathic medicines, but as there was no significant change in the sugar levels, he stopped allopathic medicine and started ayurvedic medicines. The blood sugar was well under control, until March 2021. The patient had a history of chronic calcific pancreatitis since 2011, for which he had taken allopathic treatment and got relief. Now he is not taking any medication for the same. He now consulted Dr G G Gangadharan and the Ayurvedic diagnosis was made as Prameha. The line of treatment was pramehara cikitsa, to increase the vyadhi kshamata and to normalise jataragni. USG Abdomen done on 25.8.2021 revealed dilated pancreatic duct measuring 11mm with calculus measuring 17 mm. With standalone ayurveda treatment, diet and lifestyle modification, the blood sugar values showed a significant reduction within 4 months’ time. The HbA1c which was recorded as 8.6 at baseline, reduced to 6.5 % which demonstrates the shift from poor control to good control. A repeat USG showed the size of the pancreatic duct dilation and calculus remarkably reduced to 8.4mm and 5.9 mm.
-
Summaries
-
Listen
-
Watch
-
View
-
Read

A 65-year-old male patient complained of fluctuation in blood sugar levels since March 2021. He is a known diabetic since past 7 years. Initially, he took allopathic medicines, but as there was no significant change in the sugar levels, he stopped allopathic medicine and started ayurvedic medicines. The blood sugar was well under control, until March 2021. The patient had a history of chronic calcific pancreatitis since 2011, for which he had taken allopathic treatment and got relief. Now he is not taking any medication for the same. He now consulted Dr G G Gangadharan and the Ayurvedic diagnosis was made as Prameha. The line of treatment was pramehara cikitsa, to increase the vyadhi kshamata and to normalise jataragni. USG Abdomen done on 25.8.2021 revealed dilated pancreatic duct measuring 11mm with calculus measuring 17 mm. With standalone ayurveda treatment, diet and lifestyle modification, the blood sugar values showed a significant reduction within 4 months’ time. The HbA1c which was recorded as 8.6 at baseline, reduced to 6.5 % which demonstrates the shift from poor control to good control. A repeat USG showed the size of the pancreatic duct dilation and calculus remarkably reduced to 8.4mm and 5.9 mm.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Standalone successful ayurvedic management of Diabetes Mellitus with a history of chronic calcific pancreatitis - A case report.
Dr G G Gangadharan
ABSTRACT
A 65-year-old male patient complained of fluctuation in blood sugar levels since March 2021. He is a known diabetic since past 7 years. Initially, he took allopathic medicines, but as there was no significant change in the sugar levels, he stopped allopathic medicine and started ayurvedic medicines. The blood sugar was well under control, until March 2021. The patient had a history of chronic calcific pancreatitis since 2011, for which he had taken allopathic treatment and got relief. Now he is not taking any medication for the same. He now consulted Dr G G Gangadharan and the Ayurvedic diagnosis was made as Prameha. The line of treatment was pramehara cikitsa ,to increase the vyadhi kshamata and to normalise jataragni. USG Abdomen done on 25.8.2021 revealed dilated pancreatic duct measuring 11mm with calculus measuring 17 mm. With standalone ayurveda treatment, diet and lifestyle modification, the blood sugar values showed a significant reduction within 4 months’ time. The HbA1c which was recorded as 8.6 at baseline, reduced to 6.5 which demonstrates the shift from poor control to good control. A repeat USG showed the size of the pancreatic duct dilation and calculus remarkably reduced to 8.4mm and 5.9 mm.
KEYWORDS
Prameha, diabetes mellitus, ayurveda, case report, standalone
INTRODUCTION
Diabetes mellitus (DM) is a metabolic disease, involving elevated blood glucose levels. DM has several categories, including type 1, type 2, maturity-onset diabetes of the young (MODY), gestational diabetes, neonatal diabetes, and secondary causes due to endocrinopathies, steroid use, etc. The main subtypes of DM are Type 1 diabetes mellitus (T1DM) and Type 2 diabetes mellitus (T2DM), which classically results from defective insulin secretion (T1DM) and/or action (T2DM). T1DM presents in children or adolescents, while T2DM is thought to affect middle-aged and older adults who have prolonged hyperglycemia due to poor lifestyle and dietary choices. The pathogenesis for T1DM and T2DM is drastically different, and therefore each type has various etiologies, presentations, and treatments.
Prognosis: Diabetes mellitus was the seventh leading cause of death in the United States in 2015. The prognosis of DM gets significantly influenced by the degree of glucose management. Chronic hyperglycemia significantly increases the risk of DM complications. The Diabetes Control and Complications Trial and the United Kingdom Prospective Diabetes Study found that individuals with T1DM and T2DM respectively had increased microvascular complications with chronic hyperglycemia. Patients who can revert to normal glucose during the progression of pre-diabetes to DM had a good prognosis and may be able to slow disease progression.
Treatment: The physiology and treatment of diabetes are complex and require a multitude of interventions for successful disease management. Diabetic education and patient engagement are critical in management. Patients have better outcomes if they can manage their diet (carbohydrate and overall caloric restriction), exercise regularly (more than 150 minutes weekly), and independently monitor glucose. Lifelong treatment is often necessary to prevent unwanted complications. Ideally, glucose levels should be maintained at 90 to 130 mg/dL and HbA1c at less than 7%. While glucose control is critical, excessively aggressive management may lead to hypoglycemia, which can have adverse or fatal outcomes.
Diagnostic Criteria : The diagnosis of T1DM is usually through a characteristic history supported by elevated serum glucose levels (fasting glucose greater than 126 mg/dL, random glucose over 200 mg/dL, or hemoglobin A1C (HbA1c exceeding 6.5%) with or without antibodies to glutamic acid decarboxylase (GAD) and insulin.
PATIENT INFORMATION
A 65-year-old male patient complained of fluctuation in blood sugar levels since March 2021. He is a known diabetic since past 7 years.
Medical History: Initially, he took allopathic medicines, but as there was no significant change in the sugar levels, he stopped allopathic medicine and started ayurvedic medicines. The blood sugar was well under control, until March 2021. The patient had a history of chronic calcific pancreatitis since 2011, for which he had taken allopathic treatment and got relief. Now he is not taking any medication for the same. He now consulted Dr G G Gangadharan and the Ayurvedic diagnosis was made as Prameha.
CLINICAL FINDINGS/PHYSICAL EXAMINATION
BP - 130/80mm/Hg, Weight - 73 kg
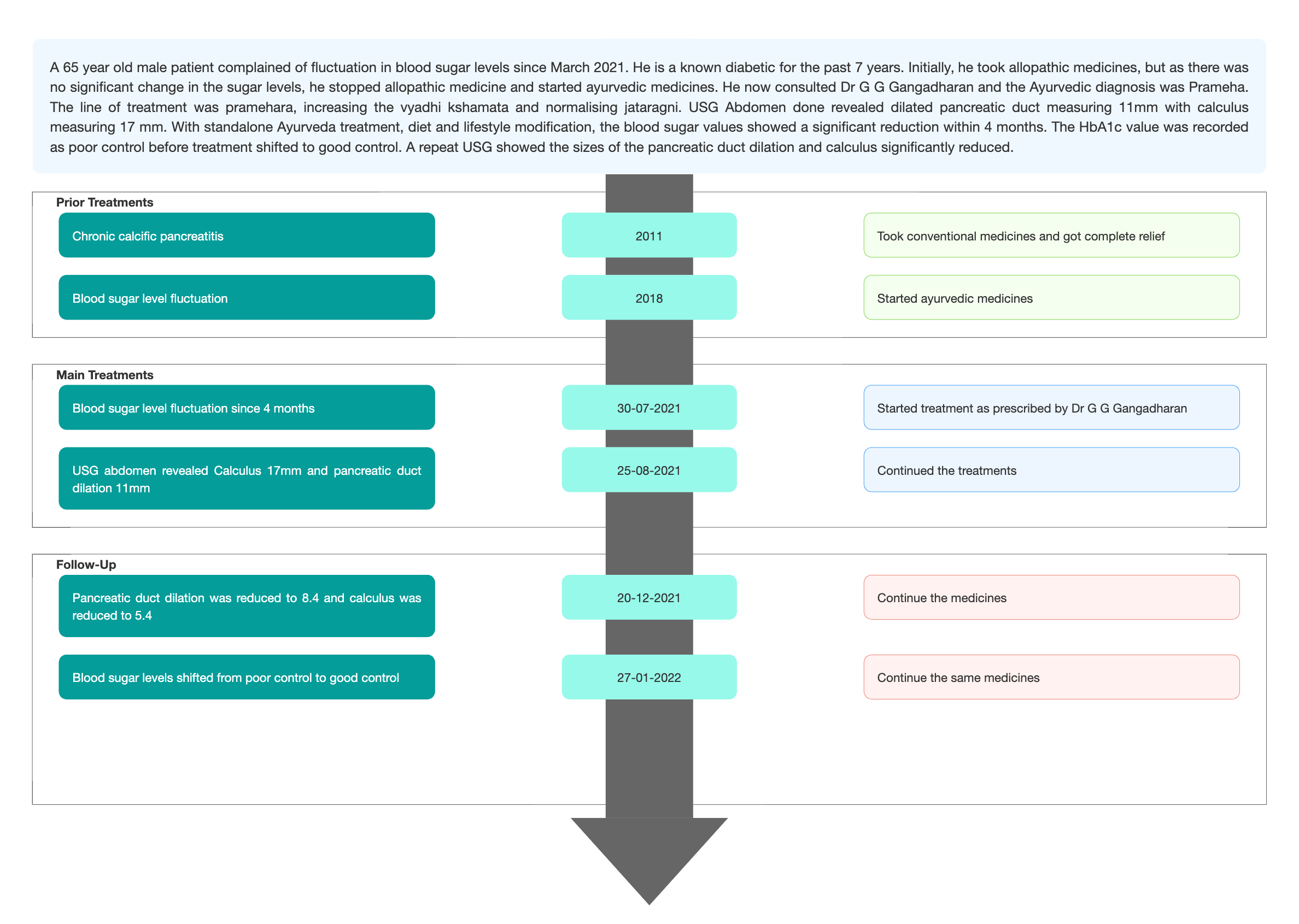
TIMELINE
Image 1. Timeline of events added as an attachment
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The patient was a known diabetic since 7 years.
Image 2. Baseline evaluation. Diagnosis confirmation report added below
Image 3. Blood sugar report dated 18.1.2021 added below
Image 4. USG abdomen dated 25.8.2021 with the pancreatic calculus and duct measurement added below
Ayurvedic Assessment was done based on the clinical evaluation by the ayurvedic physician.
Differential Diagnosis- This does not apply as the patient came in with a definite diagnosis.
Prognosis- The patient had a history of chronic calcific pancreatitis in 2011, which got cured with the allopathic treatment. On account of that, the patient is susceptible to type 3c diabetes mellitus as its complication. The management suggested standard medical care is glycemic control, lifestyle modification, nutrition, anti glycemic agents etc. The patient may be dependent on insulin lifelong in the majority of the cases.
THERAPEUTIC INTERVENTION
See the tab ‘Treatment details’
FOLLOW-UP AND OUTCOMES
Blood parameters and repeat USG abdomen to monitor the pancreatic duct calculus were done to assess the outcome of the treatment.
Image 5. Repeat USG abdomen dated 20.12.2021 added below.
This scan reveals, a reduction in the dilation of the pancreatic duct - ~8.4mm size and Calculus - ~5.9mm size.
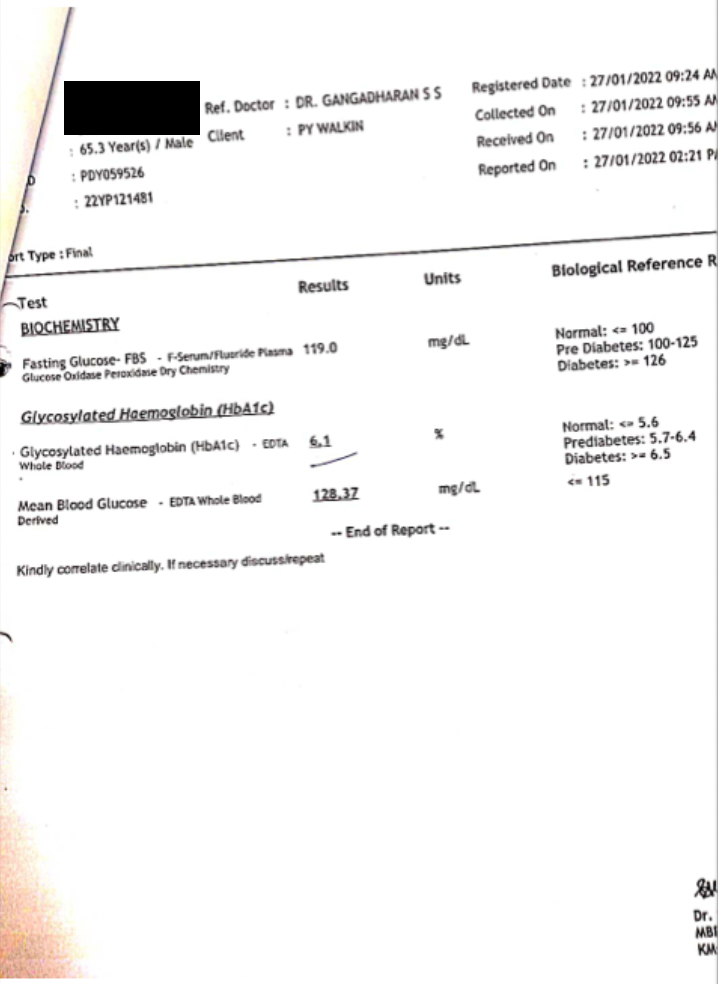
Image 6. The blood sugar levels report dated 27.1.2022 is added below
Clinician-based assessment; The first ayurvedic consultation was in July 2021. After 3 months of Ayurvedic medicines, HbA1c recorded was 6.5 in contrary to 8. 36 at baseline. After 5 months of ayurvedic treatment, a repeat USG abdomen done revealed the size of the pancreatic duct dilation reduced to 8.4mm and size of the calculus reduced to 5.9mm.
Patient-assessed: Not relevant.
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported.
DISCUSSION ;
Aim of the treatment - Pramehara chikitsa, increase the vyadhi kshamata and normalise the jataragni. Salacia tab, mehanil syrup, madhumeha kusumakara rasa, diajith powder acts as prameha hara, shugreek tab acts as immunomodulator and normalises jataragni. Acinutra syrup acts as an antacid.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
The patient had a history of chronic calcific pancreatitis, which was managed successfully with conventional medicines. Although Diabetes mellitus can be considered a complication of calcified pancreatitis, it can be managed with glycaemic control, but the consequences expected are lifelong insulin dependency and poor fat digestion. But in this case report, with standalone Ayurveda treatment, in 4 months, the fluctuating blood sugar level, which was in poor control, changed to good control. The pancreatic duct and calculus measurement also significantly reduced. The patient is still continuing the medicines.
INFORMED CONSENT
Written consent was obtained from the patient to publish the case report.
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
- Sapra A, Bhandari P. Diabetes Mellitus. In: StatPearls. Treasure Island (FL): StatPearls Publishing; June 26, 2022.
- Ashtanga Hrdaya. Cikitsa sthana. 12th Chapter.
Image 1. Timeline
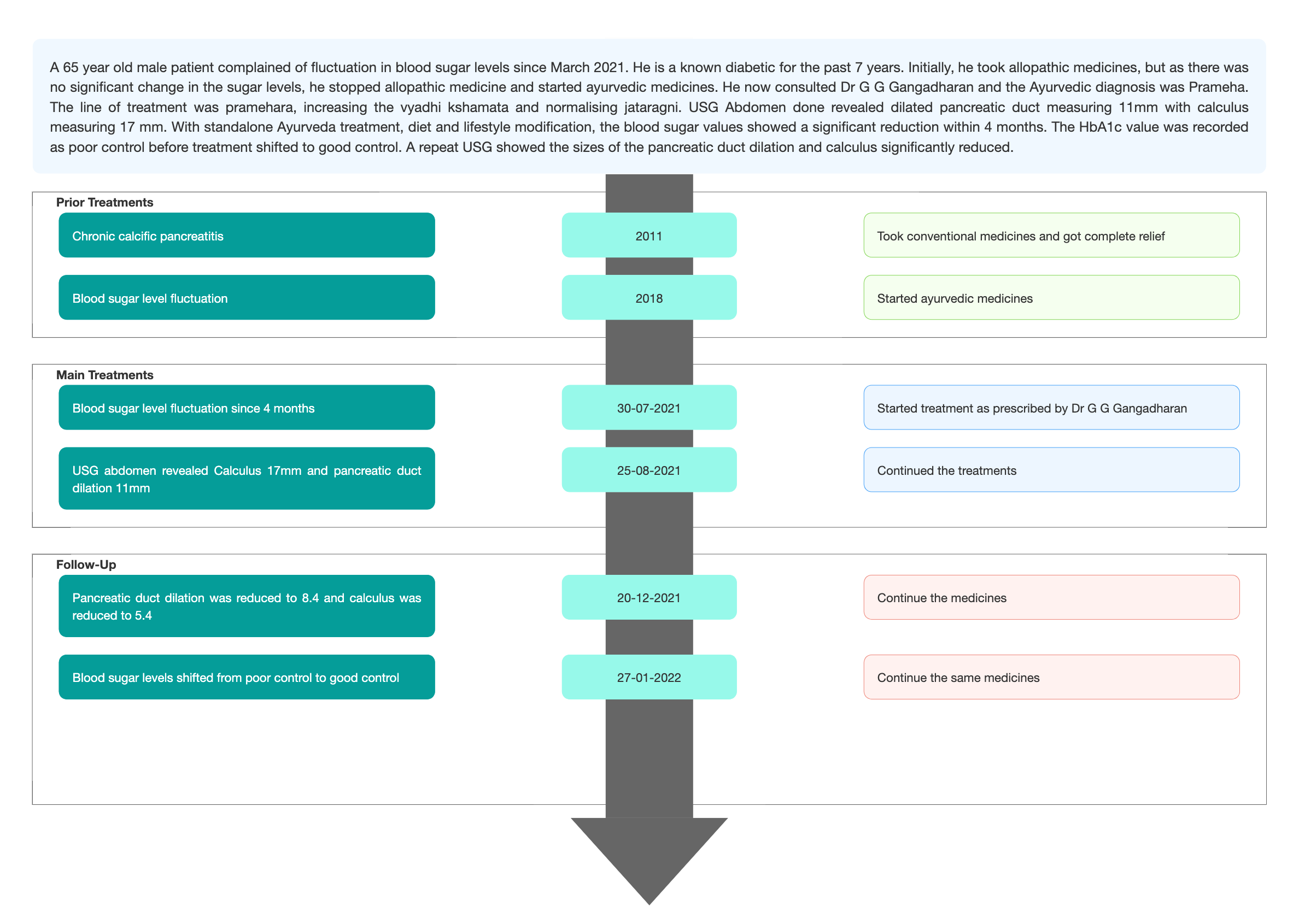
Image 2. Baseline evaluation. Diagnosis confirmation document
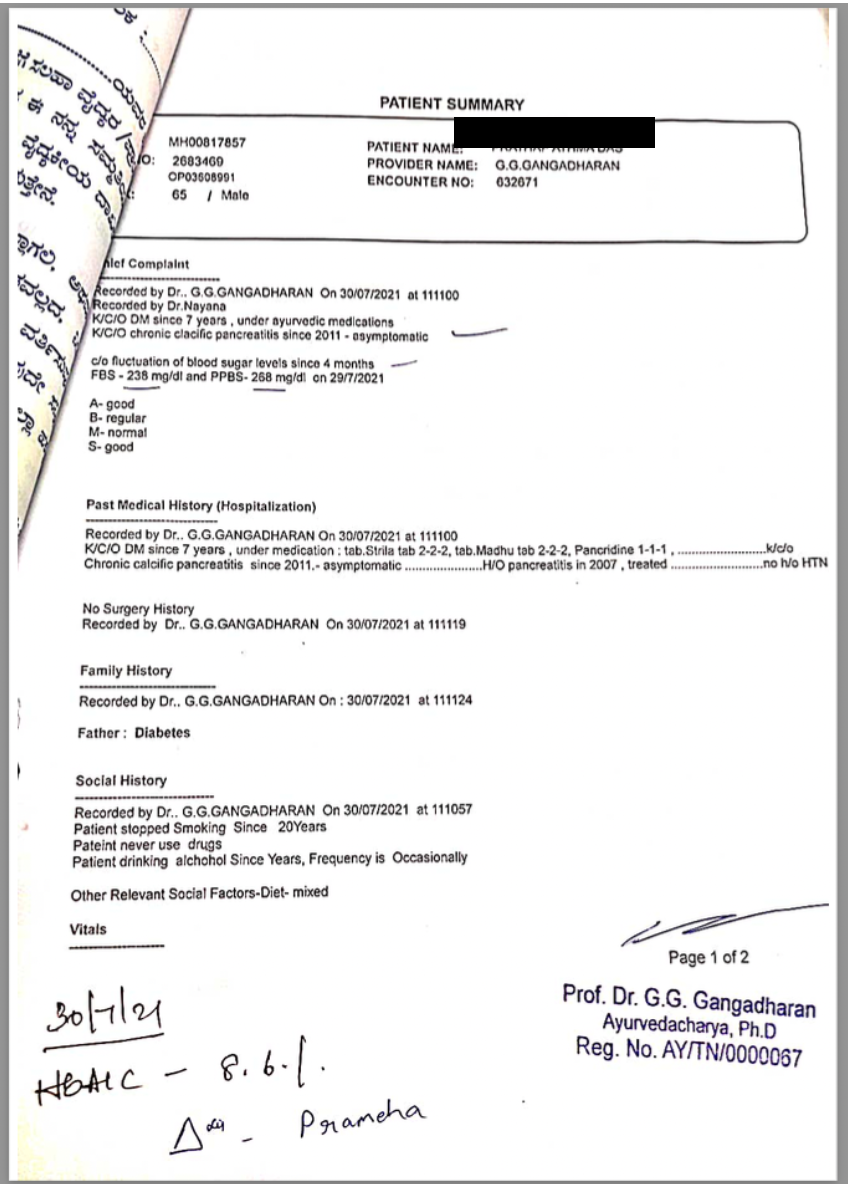
Image 3. Blood sugar report dated 18.1.2021
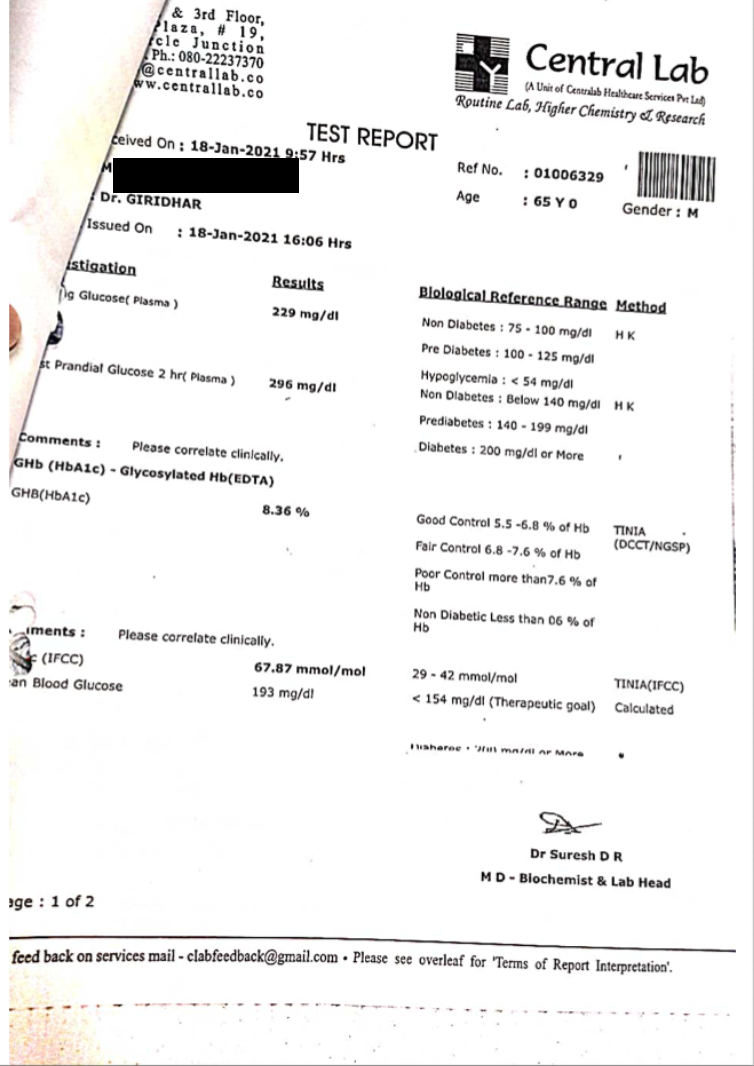
Image 4. USG abdomen dated 25.8.2021
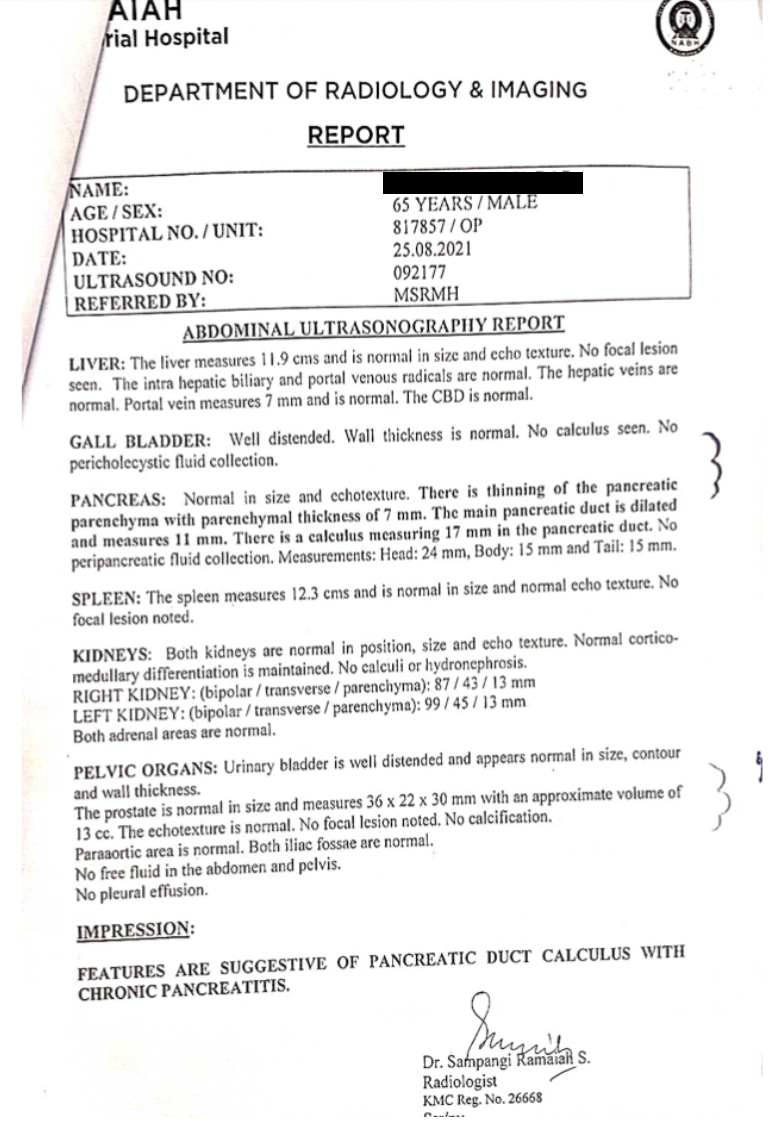
Image 5. Repeat USG abdomen dated 20.12.2021
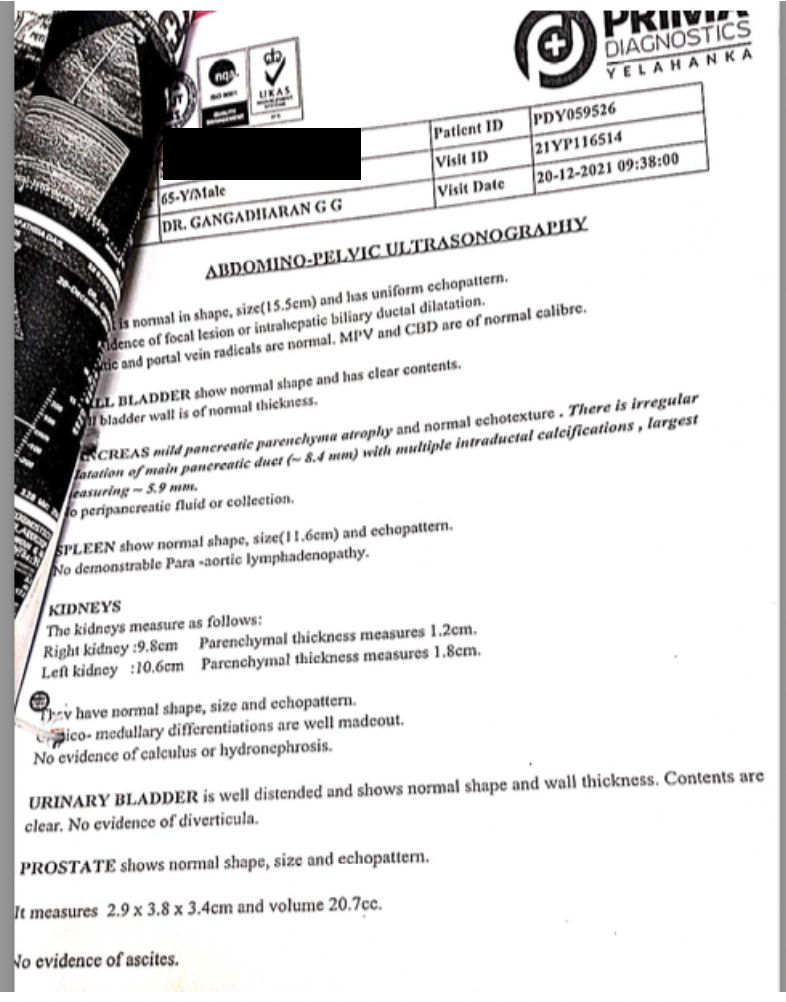
Image 6. The blood sugar levels report dated 27.1.2022
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Diabetes Mellitus (DM)
ABOUT THE DISEASE:
Diabetes mellitus (DM) is a metabolic disease, involving elevated blood glucose levels. DM has several categories, including type 1, type 2, maturity-onset diabetes of the young (MODY), gestational diabetes, neonatal diabetes, and secondary causes due to endocrinopathies, steroid use, etc. The main subtypes of DM are Type 1 diabetes mellitus (T1DM) and Type 2 diabetes mellitus (T2DM), which classically result from defective insulin secretion (T1DM) and/or action (T2DM). T1DM presents in children or adolescents, while T2DM is thought to affect middle-aged and older adults who have prolonged hyperglycemia due to poor lifestyle and dietary choices. The pathogenesis for T1DM and T2DM is drastically different, and therefore each type has various etiologies, presentations, and treatments.
Prognosis: Diabetes mellitus was the seventh leading cause of death in the United States in 2015. The prognosis of DM gets significantly influenced by the degree of glucose management. Chronic hyperglycemia significantly increases the risk of DM complications. The Diabetes Control and Complications Trial and the United Kingdom Prospective Diabetes Study found that individuals with T1DM and T2DM respectively had increased microvascular complications with chronic hyperglycemia. Patients who can revert to normal glucose during the progression from pre-diabetes to frank DM had a good prognosis and may be able to slow disease progression.
In this patient, as he was having a history of chronic calcific pancreatitis that was treated and managed, was more susceptible for further complications. The diagnosis was made based on the clinical evaluation and blood parameters. Therefore, a careful treatment plan has to be adopted. Glycemic control, diet and lifestyle modification has to be monitored.
Treatment: The physiology and treatment of diabetes are complex and require a multitude of interventions for successful disease management. Diabetic education and patient engagement are critical in management. Patients have better outcomes if they can manage their diet (carbohydrate and overall caloric restriction), exercise regularly (more than 150 minutes weekly), and independently monitor glucose. Lifelong treatment is often necessary to prevent unwanted complications. Ideally, glucose levels should be maintained at 90 to 130 mg/dL and HbA1c at less than 7%. While glucose control is critical, excessively aggressive management may lead to hypoglycemia, which can have adverse or fatal outcomes.
Diagnostic Criteria : The diagnosis of T1DM is usually through a characteristic history supported by elevated serum glucose levels (fasting glucose greater than 126 mg/dL, random glucose over 200 mg/dL, or hemoglobin A1C (HbA1c exceeding 6.5%) with or without antibodies to glutamic acid decarboxylase (GAD) and insulin.
Image 1. Baseline evaluation. Diagnosis confirmation document
Image 2. Blood sugar report dated 18.1.2021 added below
Image 3. USG abdomen dated 25.8.2021 with the pancreatic calculus duct measurement
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Prameha
ABOUT THE DISEASE:
Prameha is correlated with Diabetes taking into consideration the similarity in the symptoms. This is a metabolic syndrome which includes all those clinical conditions which are characterized by the increased quantity of urine associated with or without the increased frequency of micturition. Poly urea and Turbidity of the urine are the two characteristic symptoms of Prameha.
Samprapti: By the favorable combination of all the three specific factors viz., etiology, dosas and dhatus, Kapha gets immediately aggravated because of the vriddhi already attained and initiates the process of manifestation of prameha because of the shaithilya developed in the body. The aggravated kapha spreads all over the body and while spreading it first gets mixed with medas because there is an increase in Medas which is also unbound (Bahu and Abaddha). Kapha and Medas share identical qualities like heaviness, coldness etc. these two mix with mamsa and liquid dhatus of the body. The vitiation of mamsa leads to prameha-pidaka, the vitiated liquid dhatus convert into mutra. The mutravaha srotas are obstructed by medas and kapha thus giving rise to prameha.
LAKSHANA:
स्वेदोऽङ्गगन्धः शिथिलाङ्गता च शय्यासनस्वप्नसुखे रतिश्च|
हृन्नेत्रजिह्वाश्रवणोपदेहो घनाङ्गता केशनखातिवृद्धिः||१३||
शीतप्रियत्वं गलतालुशोषो माधुर्यमास्ये करपाददाहः|
भविष्यतो मेहगदस्य रूपं मूत्रेऽभिधावन्ति पिपीलिकाश्च||१४|| (CS. Ci. 6.13-14)
Excessive sweating with fetid odor, flabbiness of body, inclination to lie down, sedentary habits, excessive mucosal discharge, obesity, excess growth of hairs and nails, thirst, the sweetness of mouth, burning sensation in hands and feet, swarming of ants on the urine are the symptoms of Prameha.
Prognosis: Out of the different types of Prameha- Madhumeha (Vataja) is said to be asadhya.
Treatment: The patient is administered Snehana – oleation treatment. Then, Vamana, Virecana recipes, described in Charaka Kalpa sthana are administered. After Dosha is eliminated, the patient is given Santarpana or nourishing therapy because Apatarpana (fasting) therapy in this condition may produce gulma, kshaya, meha, vastishoola, and mutragraha. Hence, based on the state of Agni (digestion strength), Prameha patient should be given santarpana (nourishing therapy), after shodhana.
If the patient of prameha who needs shodhana or elimination therapy is not eligible for it, then he is given shamana treatment (with oral medicines)
Ayurvedic Assessment and Diagnosis in this case report; This patient is a confirmed case of Diabetes mellitus. Based on the Lakshanas, and lab investigations Ayurvedic diagnosis was made.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Salacia Tab Tablet 2 tablets, twice daily Oral, 15 minutes before food 2021-07-30 - 2022-07-31 Ayurvedic proprietary medicine Pramehanil Syrup Syrup 10ml + 30 ml of water, twice daily Oral, 15 minutes after food 2021-07-30 - 2022-01-30 Ayurvedic proprietary medicine Madhumehakusumakara rasa Tablet 1 tablet, twice daily Oral, 15 minutes after food 2021-07-30 - 2022-02-25 Ayurvedic proprietary medicine Diajith churna Churna 1 tsp, once daily Oral, with water - at bed time 2021-07-30 - 2022-01-30 Ayurvedic proprietary medicine Shugreek tab Tablet 2 tablets, once daily Oral, at bed time 2021-07-30 - 2022-01-27 Ayurvedic proprietary medicine Ksheerabala taila Tailam As required External application on head 2021-07-30 - 2022-01-30 Sahasrayogam, Taila prakaranam Acinutra syrup Syrup 10ml Oral, when needed 2021-07-30 - 2022-01-30 Ayurvedic proprietary medicine -
Outcome Measures
Clinical outcome
A 65-year-old male patient has been a known case of diabetes mellitus for seven years. He was on Ayurveda treatment in the past years but recently observed fluctuations in his blood sugar level. He adopted the current treatment for better care. With the standalone ayurveda treatment, diet and lifestyle modification, the patient attained a better result in 4 months' time. The HbA1c was brought to 6.5 % which indicated good control, contrary to the poor control at baseline.
Image 1. Repeat USG abdomen dated 20.12.2021 added below.
This scan reveals, a reduction in the dilation of the pancreatic duct - ~8.4mm size and Calculus - ~5.9mm size.
Image 2. Blood sugar levels report dated 27.1.2022 is added below
Disease Modifying Effect: Blood sugar level changed to good control from poor control at baseline. Ayurvedic medicines with diet and lifestyle modification helped improve the quality of life of the patient who was a chronic diabetic.
Image 1. Repeat USG abdomen dated 20.12.2021
Image 2. Blood sugar levels report dated 27.1.2022
-