Featured Case
-
Abstract
A 44-year-old male patient complained of abdominal distention, pitting oedema of both lower limbs and yellowish discolouration of eyes and urine for 2 weeks. At the onset of symptoms, he consulted a gastroenterologist who diagnosed him with Decompensated Chronic Liver disease on 29/5/21 (severe liver cirrhosis stage 3) based on the CECT abdomen. As his CHILD C CTP was 11/15 and MELD was 25, he was advised for a liver transplant. As the patient was not willing to have surgery, he consulted Dr G G Gangadharan. The ayurvedic diagnosis was made as yakrutodara. During Ayurvedic treatments, his regular conventional medicine was also continued. The ascetic fluid tapping was done under aseptic conditions 3 times within 2 weeks. Fluid analysis was done regularly. At the time of discharge, after 2 weeks, yellowish discolouration of eyes and urine resolved, abdominal distention and pitting oedema in lower limbs reduced. The elevated blood parameters were also reduced to near normal limits. Monthly follow-up was done and routine blood investigations like CBC, ESR, LFT, INR were done. After discharge, the patient continued the internal medicines, and the frequency of fluid tapping was reduced to once a week. There was a reduction in swelling of legs, yellowish discolouration of eyes completely resolved. The patient is continuing the medicines and is requested to come for regular follow ups.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 44-year-old male patient complained of abdominal distention, pitting oedema of both lower limbs and yellowish discolouration of eyes and urine for 2 weeks. At the onset of symptoms, he consulted a gastroenterologist who diagnosed him with Decompensated Chronic Liver disease on 29/5/21 (severe liver cirrhosis stage 3) based on the CECT abdomen. As his CHILD C CTP was 11/15 and MELD was 25, he was advised for a liver transplant. As the patient was not willing to have surgery, he consulted Dr G G Gangadharan. The ayurvedic diagnosis was made as yakrutodara. During Ayurvedic treatments, his regular conventional medicine was also continued. The ascetic fluid tapping was done under aseptic conditions 3 times within 2 weeks. Fluid analysis was done regularly. At the time of discharge, after 2 weeks, yellowish discolouration of eyes and urine resolved, abdominal distention and pitting oedema in lower limbs reduced. The elevated blood parameters were also reduced to near normal limits. Monthly follow-up was done and routine blood investigations like CBC, ESR, LFT, INR were done. After discharge, the patient continued the internal medicines, and the frequency of fluid tapping was reduced to once a week. There was a reduction in swelling of legs, yellowish discolouration of eyes completely resolved. The patient is continuing the medicines and is requested to come for regular follow ups.
-
-
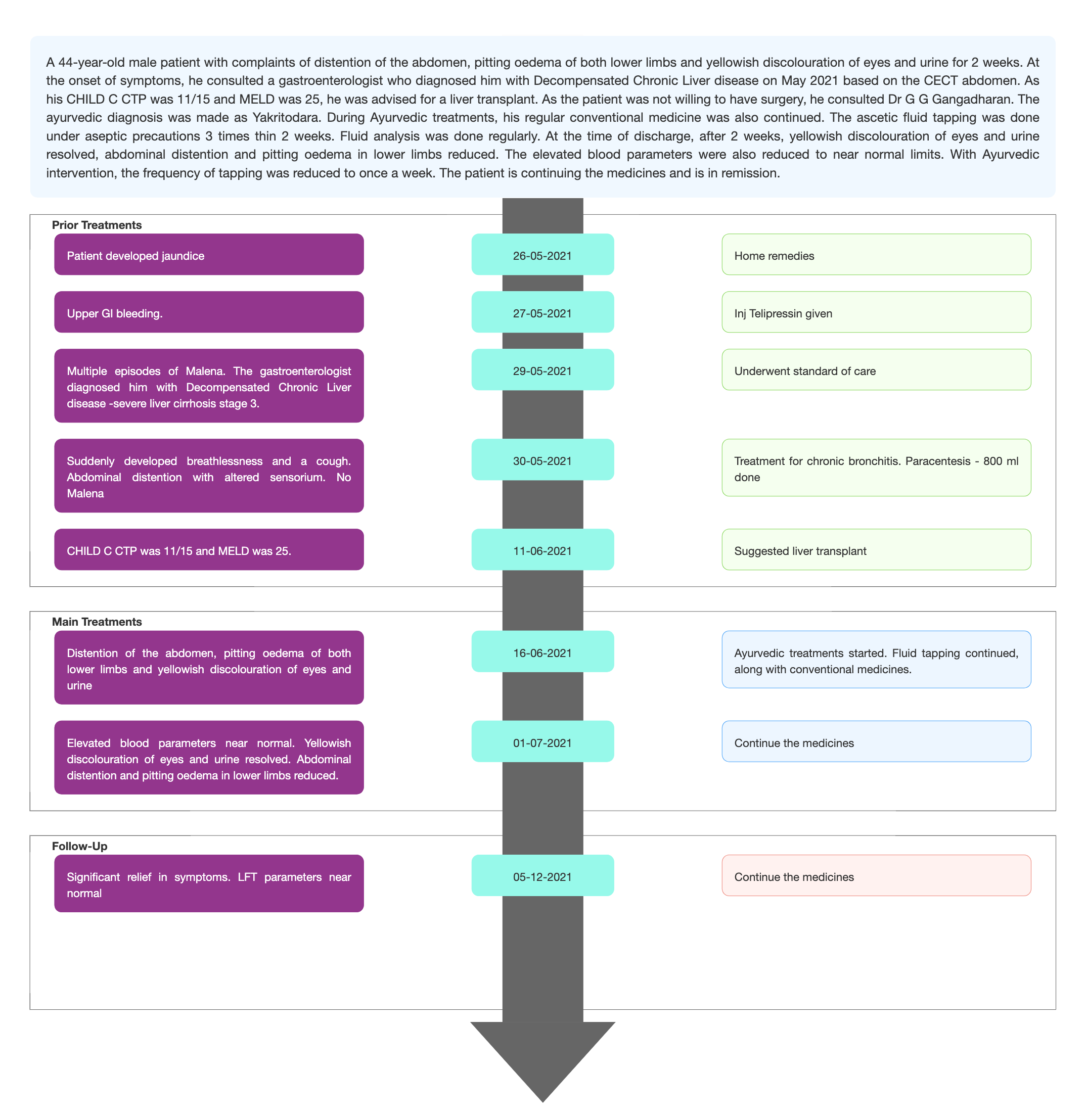
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Integrative management of decompensated chronic liver disease- a case report
Dr G G Gangadharan
ABSTRACT
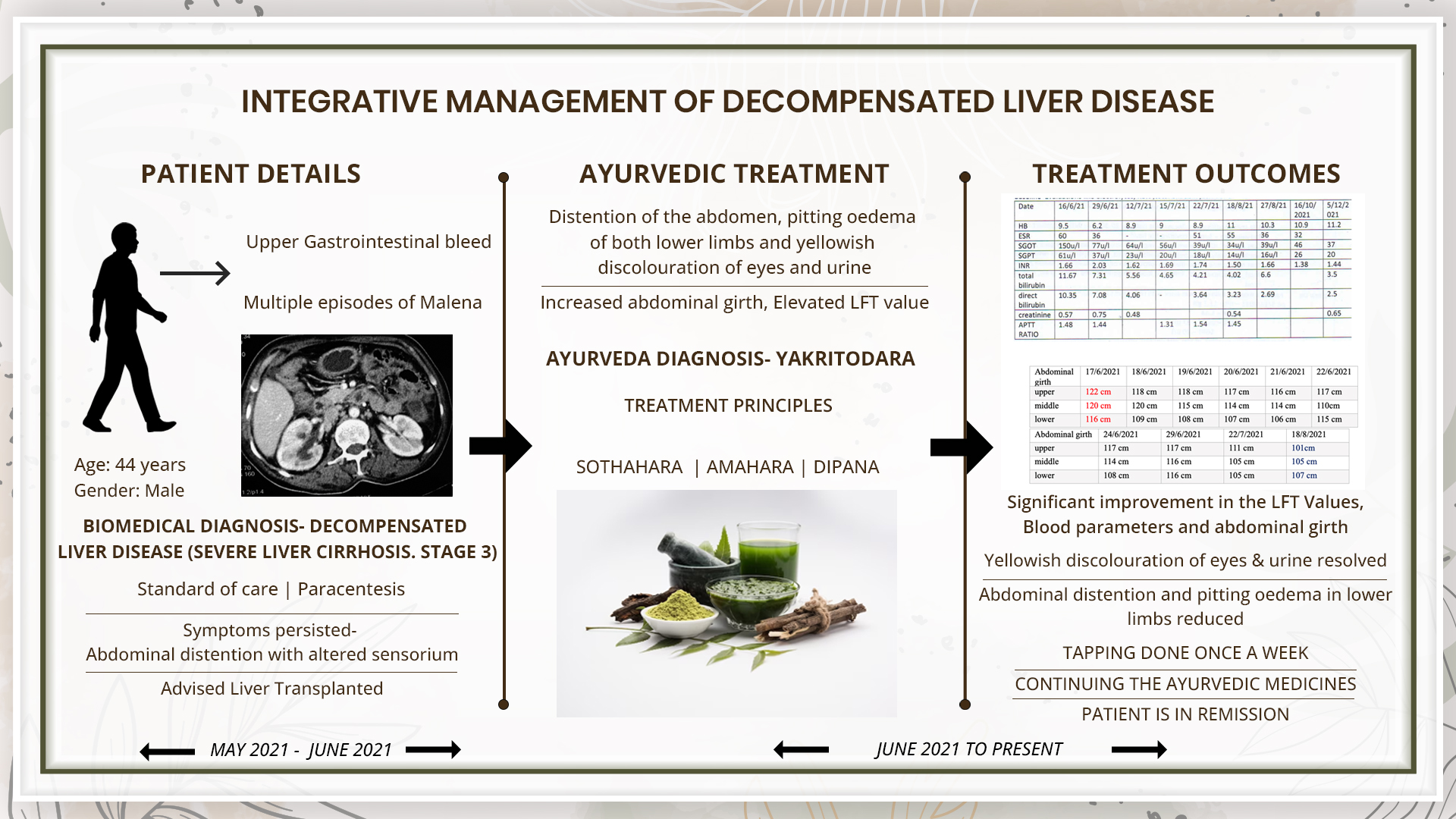
A 44-year-old male patient with complaints of distention of the abdomen, pitting oedema of both lower limbs and yellowish discolouration of eyes and urine for 2 weeks. At the onset of symptoms, he consulted a gastroenterologist who diagnosed him with Decompensated Chronic Liver disease on 29/5/21 (severe liver cirrhosis stage 3) based on the CECT abdomen. As his CHILD C CTP was 11/15 and MELD was 25, he was advised for a liver transplant. As the patient was not willing to have surgery, he consulted Dr G G Gangadharan. The ayurvedic diagnosis was made as yakritodara. During Ayurvedic treatments, his regular conventional medicine was also continued. The ascetic fluid tapping was done under aseptic precautions 3 times thin 2 weeks. Fluid analysis was done regularly. At the time of discharge, after 2 weeks, yellowish discolouration of eyes and urine resolved, abdominal distention and pitting oedema in lower limbs reduced. The elevated blood parameters were also reduced to near normal limits. Monthly follow-up was done and routine blood investigations like CBC, ESR, LFT, INR were done. After discharge, the patient continued the internal medicines, and the frequency of fluid tapping was reduced. With Ayurvedic intervention, the frequency of tapping was reduced to once a week. There was a reduction in swelling of legs, yellowish discolouration of eyes completely resolved. The patient is continuing the medicines and is in remission.
KEYWORDS
Yakrutodara, cirrhosis, case report, CLD, decompensated liver disease, CHILD C, MELD, integrative
INTRODUCTION
About 35 % of alcohol drinkers, are affected with advanced liver disease, while the rest handle the clinical condition with medical help. There are still no pharmacological or nutritional therapies that are FDA-approved to be used in the treatment of alcoholic liver disease. Excessive and chronic consumption of alcohol results in a range of hepatic lesions, like steatosis, hepatitis, and fibrosis/cirrhosis. This is a progressive disorder and requires medical intervention immediately. Cessation of drinking (i.e., abstinence) is an integral part of therapy. Liver transplantation remains the life-saving strategy for patients with end-stage alcoholic liver disease (Osna NA, Donohue TM Jr, Kharbanda KK. Alcoholic Liver Disease: Pathogenesis and Current Management. Alcohol Res. 2017;38(2):147-161. PMID: 28988570; PMCID: PMC5513682)
Prognosis: In the initial stages, the condition can be reversed like fatty changes. But when fibrosis and cirrhosis set in, it becomes irreversible. Alcohol abstinence is a mandatory rule as a part of therapy. The target of the treatment is to try and normalise the blood parameters and help maintain the quality of life. If the patient is nonresponsive to treatment and the condition worsens, then liver transplantation is suggested.
Treatment options: Medical and surgical interventions are available depending on the extent of liver damage. Liver transplantation is the last option suggested if the patient is nonresponsive to the treatments, causing clinical deterioration.
PATIENT INFORMATION
A 44 year old male patient suffered from distention of the abdomen, pitting oedema of both lower limbs and yellowish discolouration of eyes and urine since 3 weeks.
Medical History: At the onset of symptoms, he consulted a gastroenterologist who diagnosed him with Decompensated Chronic Liver disease on 29/5/21 (severe liver cirrhosis stage 3) based on the CECT abdomen. As his CHILD C CTP was 11/15 and MELD was 25, he was advised for a liver transplant. As the patient was not willing to have surgery, he consulted Dr G G Gangadharan. The ayurvedic diagnosis was made as yakritodara
CLINICAL FINDINGS/PHYSICAL EXAMINATION
BP – 130/90 mmhg , PR- 74 bpm, SpO2 – 97 % in RA, Temperature – Afebrile
Abdominal girth : upper- 122cm, middle- 120cm, lower- 116cm
TIMELINE
Image 1. Timeline of events attached below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The biomedical diagnosis was made based on clinical evaluation and discharge summary from the Modern hospital.
Image 2. Diagnosis proof document dated 11.6.2021
Image 3. CRP value dated 4.6.2021 and 9.06.2021
Image 4. Serum sodium value and eGFR dated 8.6.2021 were added below
Ayurvedic Assessment was done based on the clinical evaluation by the Ayurvedic physician.
Differential Diagnosis- The patient came in with a confirmed diagnosis.
Prognosis- Compensated chronic liver disease (who has not developed significant complications) usually carry a better prognosis than decompensated liver cirrhosis. Decompensated liver cirrhosis patients (who have developed variceal bleeding, ascites, HCC, SBP, and hepatorenal syndrome) have a poor prognosis. Mean survival is of about six months if the Child-Pugh score of 12 or greater or the MELD score of 21 or higher. In this case, the patient has CHILD-11 and MELD-25, which indicates a poor prognosis. With Ayurvedic treatment along with modern medicines, the clinical condition of the patient improved and elevated blood parameters were reduced to near-normal limits
THERAPEUTIC INTERVENTION
See the tab ‘Treatment details’
FOLLOW-UP AND OUTCOMES
Clinician-based assessment; At the time of discharge, after 2 weeks, yellowish discolouration of eyes and urine resolved, and abdominal distention and pitting oedema in lower limbs reduced. Blood parameters were nearing normal.
After discharge, the patient continued the internal medicines and the tapping was continued but the frequency of tapping was reduced. There was a significant reduction in the abdominal girth.
Table 1. The blood values documented through the treatment are added below
Table 2. The abdominal girth was continuously monitored before, during and after treatment added below.
Image 5. The ascetic fluid analysis done before, during and after treatment is added below.
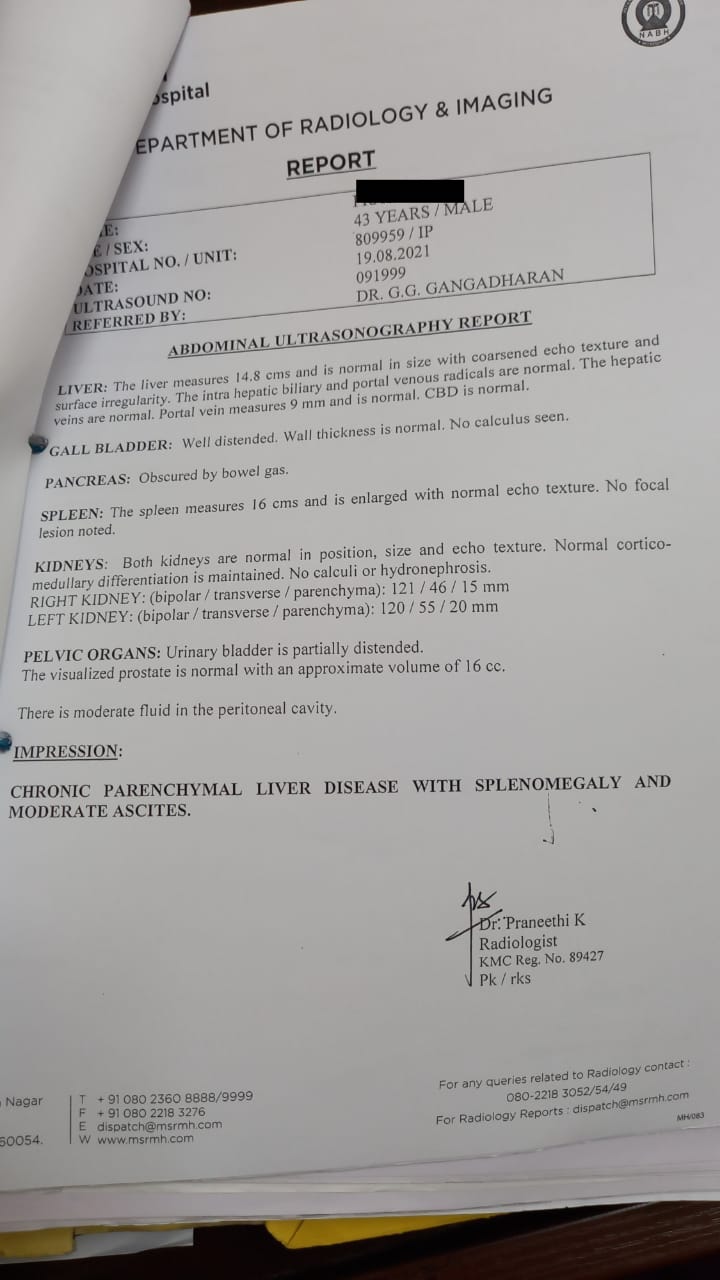
Image 6. USG abdomen dated 19.8.2021 added below
Patient based assessment: Not relevant
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported.
DISCUSSION ;
++++++++++
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
This case report demonstrates the successful Ayurvedic intervention in improving the quality of life, reducing the frequency of abdominal tapping, and normalising the elevated blood parameters of a 44-year-old male patient, suffering from decompensated liver disease.
INFORMED CONSENT
Written consent was obtained from the patient to publish the case report.
CONFLICT OF INTEREST
None declared.
FUNDING
None
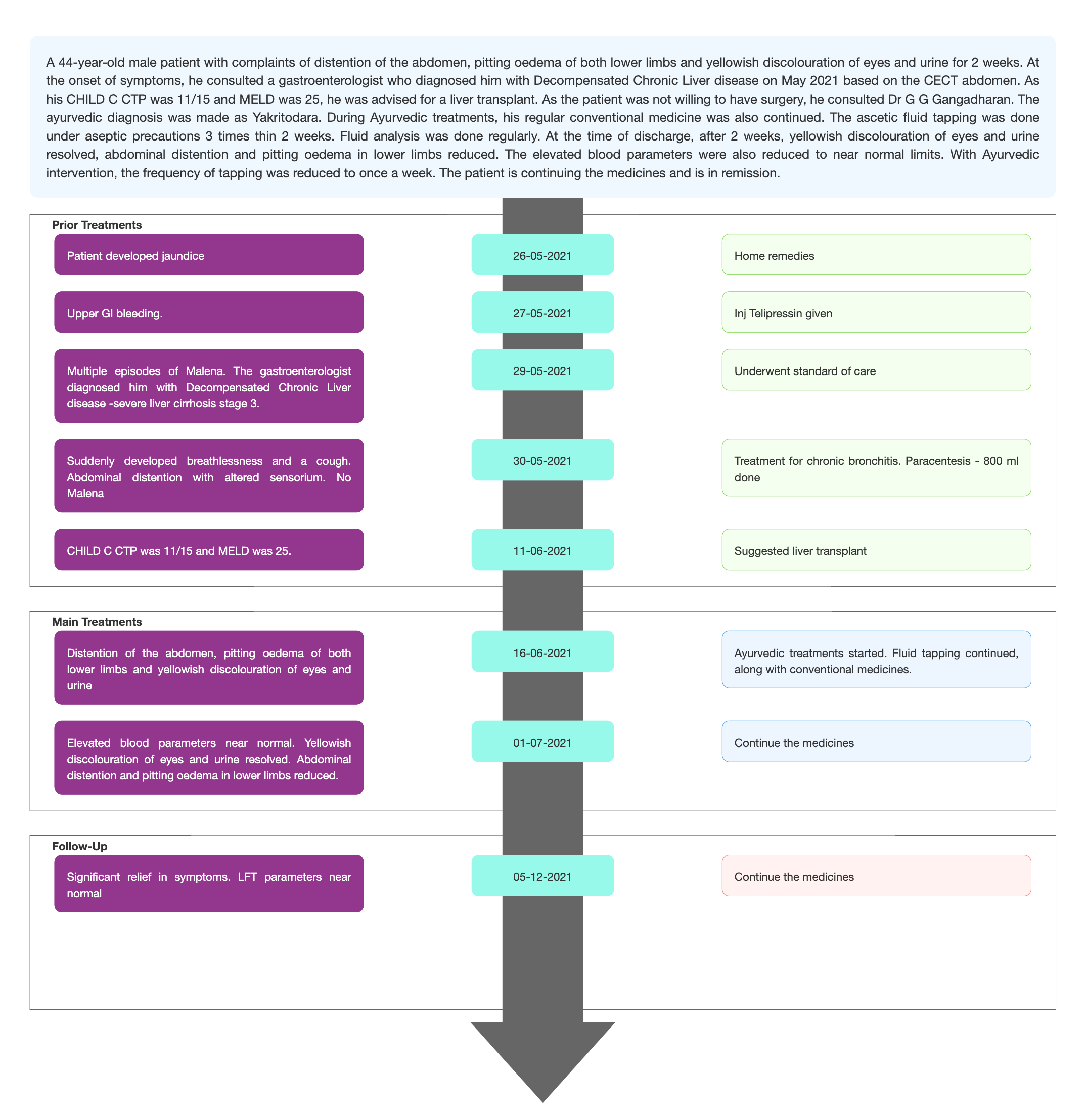
Image 2. Diagnosis proof document dated 11.6.2021

Image 3. CRP value dated 4.6.2021 and 9.06.2021
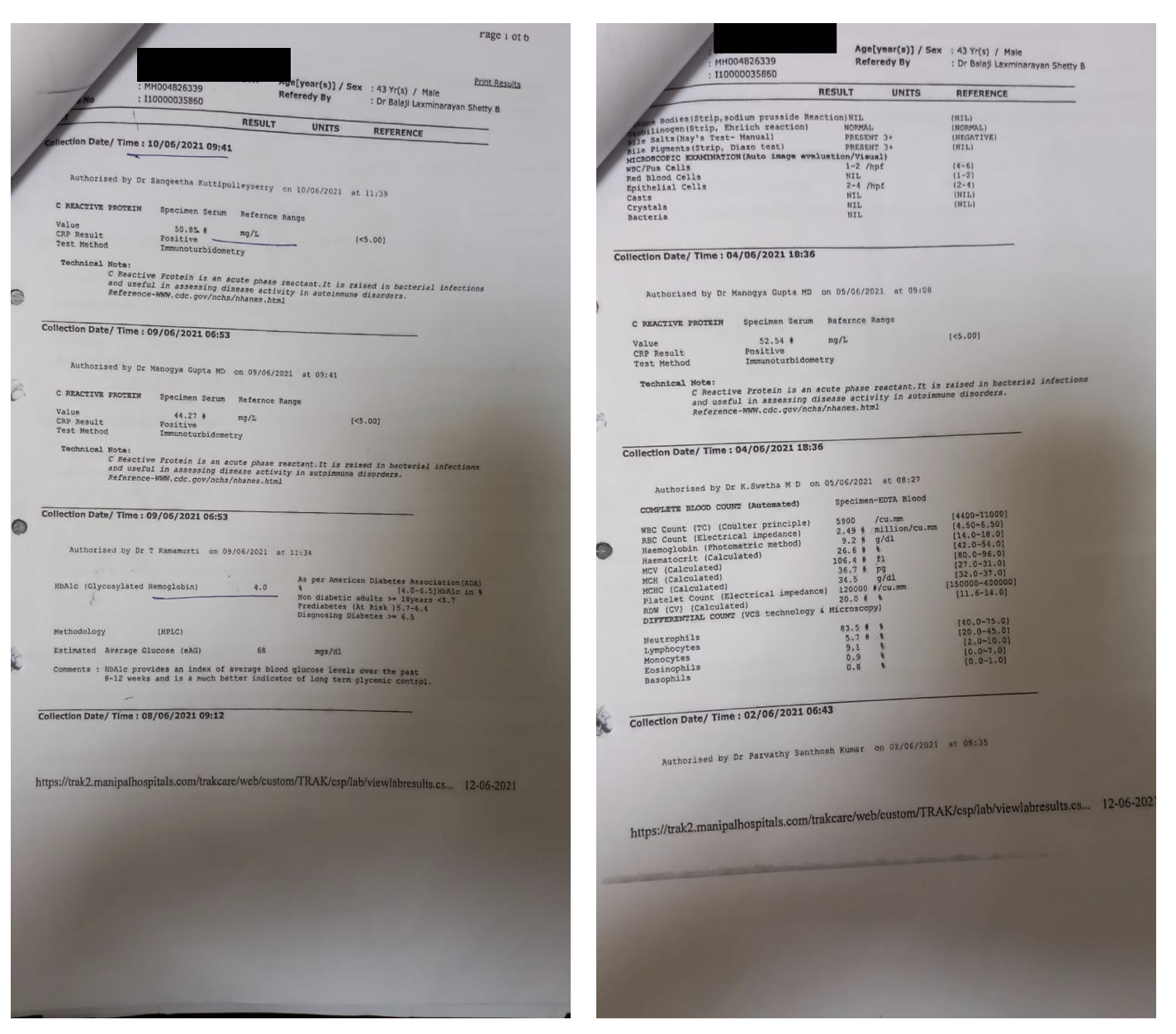
Image 4. Serum sodium value and eGFR dated 8.6.2021
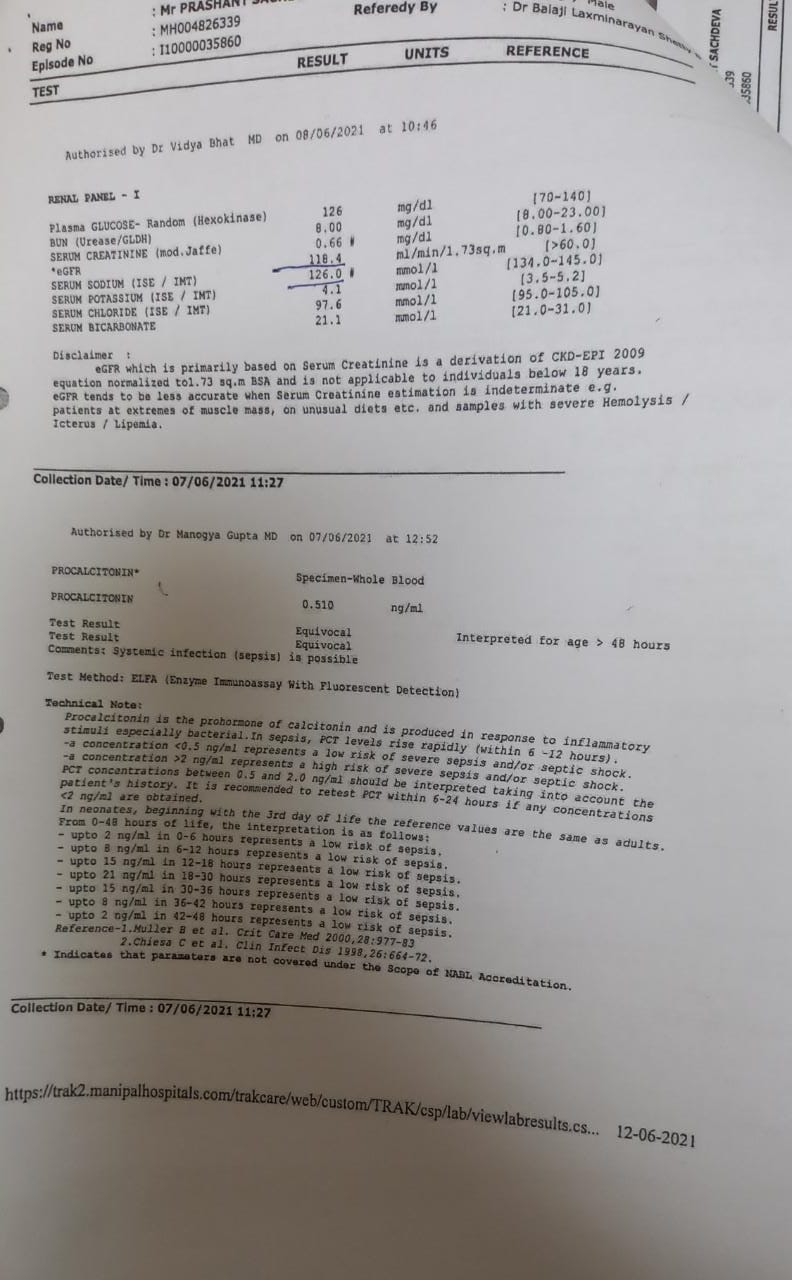
Table 1. The blood values documented through the treatment
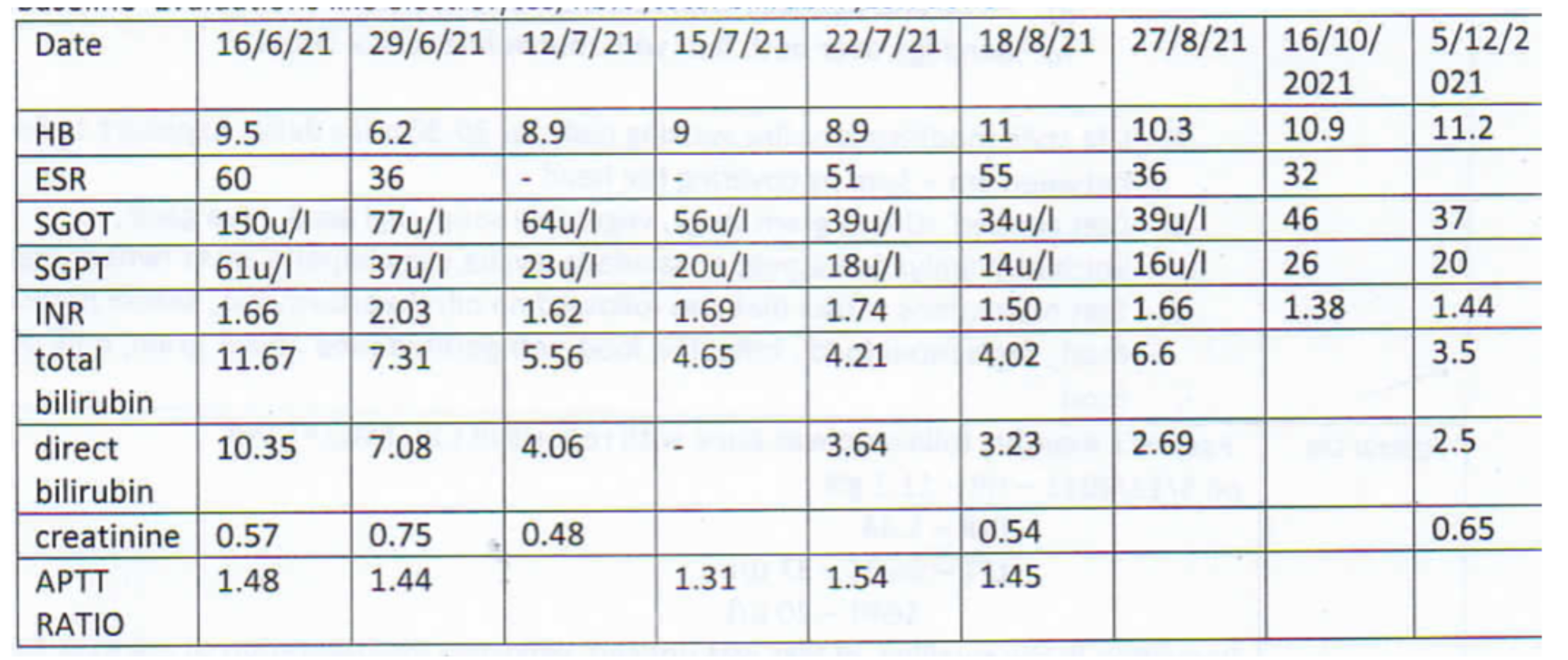
Table 2. The abdominal girth monitored before, during and after the treatment

Image 5. The ascetic fluid analysis done before, during and after treatment
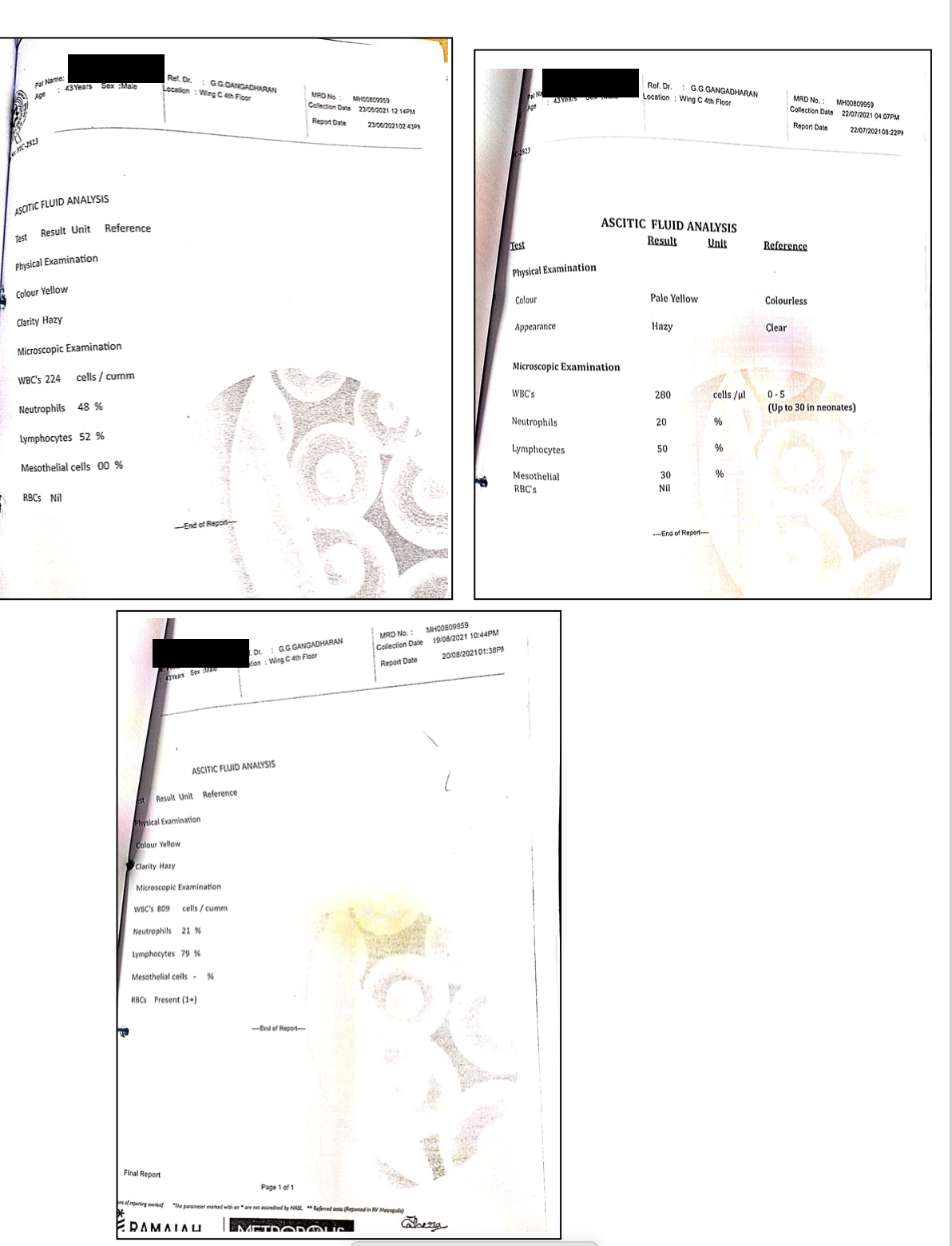
Image 6. USG abdomen dated 19.8.2021
-
Immersive Learning
-
Modern Diagnosis
Modern Diagnosis: Chronic Liver Disease- Decompensated liver disease
About the disease:
About 35 % of alcohol drinkers, are affected with advanced liver disease, while the rest handle the clinical condition with medical help. There are still no pharmacological or nutritional therapies that are FDA-approved to be used in the treatment of alcoholic liver disease. Excessive and chronic consumption of alcohol results in a range of hepatic lesions, like steatosis, hepatitis, and fibrosis/cirrhosis. This is a progressive disorder and requires medical intervention immediately. Cessation of drinking (i.e., abstinence) is an integral part of therapy. Liver transplantation remains the life-saving strategy for patients with end-stage alcoholic liver disease (Osna NA, Donohue TM Jr, Kharbanda KK. Alcoholic Liver Disease: Pathogenesis and Current Management. Alcohol Res. 2017;38(2):147-161. PMID: 28988570; PMCID: PMC5513682)
Prognosis: In the initial stages, like fatty changes the condition can be reversed. But when fibrosis and cirrhosis set in, it becomes irreversible. Alcohol abstinence is a mandatory rule as a part of therapy. The target of the treatment is to try and normalise the blood parameters and help maintain the quality of life. If the patient is nonresponsive to treatment and the condition worsens, then liver transplantation is suggested.
A 44-year-old male patient with complaints of distention of the abdomen, pitting oedema of both lower limbs and yellowish discolouration of eyes and urine for 2 weeks. At the onset of symptoms, he consulted a gastroenterologist who diagnosed him with Decompensated Chronic Liver disease on 29/5/21 (severe liver cirrhosis stage 3) based on the CECT abdomen. As his CHILD C CTP was 11/15 and MELD was 25, he was advised for a liver transplant.
Image 1. Diagnosis proof document dated 11.6.2021 added below
Image 2. CRP value dated 4.6.2021 and 9.06.2021 added below
Image 3. Serum sodium value and eGFR dated 8.6.2021 added below
Treatment options: Medical and surgical interventions are available depending on the extent of liver damage. Liver transplantation is the last option suggested if the patient is nonresponsive to the treatments, causing clinical deterioration.
Image 1. Diagnosis proof document dated 11.6.2021 added below
Image 2. CRP value dated 4.6.2021 and 9.06.2021
Image 3. Serum sodium value and eGFR dated 8.6.2021
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Yakritodara
About the Disease:
The term ‘Yakrt Vikara’ was first expounded by Bhavamishra in his treatise along with a detailed classification. ‘Ya’ stands for activity and ‘krt’ indicates disintegration or breaking down. So ‘Yakrt’ can be defined as an organ that breaks down various factors inside the body. The term ‘Vikara’ means disease. Yakrit is the mula of raktavaha srotas. It is the ashaya of pitta and agni. When the yakrt is affected, the metabolism of rasa and rakta dhatu are affected, thus manifesting in kamala. This also matches with the modern concept of derangement of bile pigments thus causing the yellow discolouration. Udara is generally used to indicate abnormal enlargement of the organ due to accumulation of fluid. Yakrtodara can be correlated to Ascites. Madhava Nidana mentions 13 different types of udara, and yakrtodara is one among them. Mala sancaya and Vata vrddhi can be considered as the main causative factors. Mala sancaya is the main causative factor for all the udara rogas.
Samprapti- This is basically a tridoshaja vyadhi, but pitta is the main aggravated dosa, as yakrit is pittasthana. Rasa, Rakta and Medas are the dushyas involved. The srotas affected are rasavaha, raktavaha, medovaha, annavaha, and purishavaha. Vyaktasthana is udara and it is a krcchra sadhya vyadhi.
The classical texts mention the symptoms of Yakrtodara as folllows;
लक्षण-
क्रमेण कुक्षिं जठरमग्न्यधिष्ठानं च परिक्षिपन्नुदरमभिनिर्वर्तयति॥३७॥
तस्यरूपाणि-दौर्बल्यारोचकाविपाकवर्चोमूत्रग्रहतमःप्रवेशापिपासाग़्गमर्दच्छर्दिमूर्च्छाग़्गसाद- कासश्वासमृदुज्वरानाहाग्निनाशकार्श्यास्यवैरस्यपर्वभेदकोष्ठवातशूलानि, अपि चोदरमरुणवर्णं विवर्णं वा नीलहरितहारिद्रराजिमद्भवति; एवमेवयकृदपि दक्षिणपार्श्वस्थं कुर्यात्, तुल्यहेतुलिग़्गौषधत्वात्तस्य प्लीहजठर एवावरोध इति; एतत् प्लीहोदरमिति विद्यात्। ||38|| (CS.Ci.13).
Acarya mentions that the symptoms of plihodara and yakrtodara are identical in features and can be managed in a similar way. Daurbalya, arocaka, avipaka, mutraghatam, pipasa, angamarda, chardi, murccha, angasada, kasa, shvasa etc are the symptoms. All or some of the symptoms may manifest in a patient suffering from this condition. In this patient, the symptoms were icterus, yellow discolouration of the skin, pedal oedema, and abdominal distention.
In this case report, a 44-year-old male patient presented with complaints of distention of the abdomen, pitting oedema of both lower limbs and yellowish discolouration of eyes and urine for 2 weeks. At the onset of symptoms, he consulted a gastroenterologist who diagnosed him with Decompensated Chronic Liver disease on 29/5/21 (severe liver cirrhosis stage 3) based on the CECT abdomen. As his CHILD C CTP was 11/15 and MELD was 25, he was advised for a liver transplant. As the patient was not willing to undergo surgery, he consulted Dr G G Gangadharan. The ayurvedic diagnosis was made as yakritodara.
Prognosis- Kricchrasadhya vyadhi
Treatment- Vatanulomana is the main target in udara rogas. In pittadhishthana rogas, like yakrit, virecana is the best treatment option to pacify the aggravated pitta. Virecana is also indicated in bahudoshavastha and srotorodha. As pitta gets pacified, there is also a direct pacifying effect on rakta. (CS. Si.6.9).
In this patient, the rationale of treatment is yet to be recieved from the treating physician.
Ayurvedic Assessment and Diagnosis: This patient is a confirmed case of Acute Liver Disease. Based on the lakshanas, clinical evaluation and the confirmed biomedical diagnosis, the Ayurvedic diagnosis was made.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Punarnava kalka Kalka 30gm 30gm with milk - empty stomach 2021-07-13 - 2021-07-23 Anubhuta Dravya prayoga Punarnavadi kashayam Kashayam 60ml- 60ml-0-60ml 15min before food 2021-06-16 - 2021-08-28 Bh. Rat 42/13 Trivrut lehya Lehya 1 tsp 1 tsp at 8pm 2021-06-16 - 2021-08-28 AH. Uth. 7 Sharapunka kashayam Kashayam 60ml 60ml-0-60ml 15min after food 2021-06-16 - 2022-05-01 AH. Uth. 27 Forestica Syrup 25ml 25ml 11am-0-5pm 2021-06-16 - 2022-05-01 Ayurvedic Proprietary Medicine Patolakaturohinyadi kashayam Kashayam 15ml-0-15ml + 45ml water at 11 am & 5 pm Oral 2021-07-13 - 2022-05-01 AH. Su. 15/15 Vasaguluchyadi kashayam Kashayam 15ml-0-15ml + 45ml water Oral 2021-06-16 - 2021-07-01 AH. Uth. 12 Arogyavardini vati Tablet 2-0-2 at 10am and 4pm Oral 2021-06-16 - 2021-07-01 Bh.Rat. Kashudrarogadhikara. 9 Gomutrahareetaki choornam Churnam 1.2 tsp + 1/2 tsp honey at 10am and 7 pm Oral 2021-06-16 - 2021-08-28 Bh.Rat. Krimirogadhikara. 31 Bhoomiamalaki Powder 5gm + seed of Mustaka paste by warm milk swallow on empty stomach followed by 100ml milk Oral 2021-06-16 - 2021-07-23 Anubhuta Dravya Prayoga Yellow bringaraja paste Kalka 5gm + warm jeera water at 11am Oral 2021-07-18 - 2021-08-23 Anubhuta dravya prayoga Tab Salacia Tablet 2-0-2 Oral 2021-08-17 - 2021-08-19 Ayurvedic proprietary medicine Markkava Rasayana Rasayana I tsp - bedtime followed by hot jeera water Oral 2021-07-18 - 2021-07-23 AH. Chi 20/8 Tab Gomutrahareetaki Tablet 2-0-2 at 11am and 5pm Oral 2021-08-19 - 2022-07-01 Ayurvedic proprietary medicine Pranada Tablet 2 at bedtime Oral 2021-08-17 - 2021-08-28 Ayurvedic proprietary medicine -
Outcome Measures
OUTCOME MEASURES
A 44-year-old male patient with complaints of distention of the abdomen, pitting oedema of both lower limbs and yellowish discolouration of eyes and urine for 2 weeks. At the onset of symptoms, he consulted a gastroenterologist who diagnosed him with Decompensated Chronic Liver disease on 29/5/21 (severe liver cirrhosis stage 3) based on the CECT abdomen. As his CHILD C CTP was 11/15 and MELD was 25, he was advised for a liver transplant. As the patient was not willing to have surgery, he consulted Dr G G Gangadharan. The ayurvedic diagnosis was made as yakritodara.
Assessment criteria: Both subjective and objective parameters were taken into consideration for assessing the outcomes.
Subjective parameters: At the time of discharge, after 2 weeks, yellowish discolouration of eyes and urine resolved, and abdominal distention and pitting oedema in lower limbs reduced.
Objective parameters: The blood parameters were constantly monitored before, during and after the treatment.
Table 1. The blood values documented throughout the treatment are added below
Table 2. The abdominal girth continuously monitored before, during and after treatment added below.
Image 1. The ascetic fluid analysis done before, during and after treatment is added below.
Image 2. USG abdomen dated 19.8.2021 added below
Disease-modifying effect: The patient is free from symptoms and requested to come for regular follow ups.
Abdominal girth
17/6/2021
18/6/2021
19/6/2021
20/6/2021
21/6/2021
22/6/2021
upper
122 cm
118 cm
118 cm
117 cm
116 cm
117 cm
middle
120 cm
120 cm
115 cm
114 cm
114 cm
110cm
lower
116 cm
109 cm
108 cm
107 cm
106 cm
115 cm
Abdominal girth
24/6/2021
29/6/2021
22/7/2021
18/8/2021
upper
117 cm
117 cm
111 cm
101cm
middle
114 cm
116 cm
105 cm
105 cm
lower
108 cm
116 cm
105 cm
107 cm
Table 1. The blood values documented throughout the treatment
Table 2. The abdominal girth monitored before, during and after treatment
Image 1. The ascetic fluid analysis done before, during and after treatment
Image 2. USG abdomen dated 19.8.2021
-