Featured Case
-
Abstract
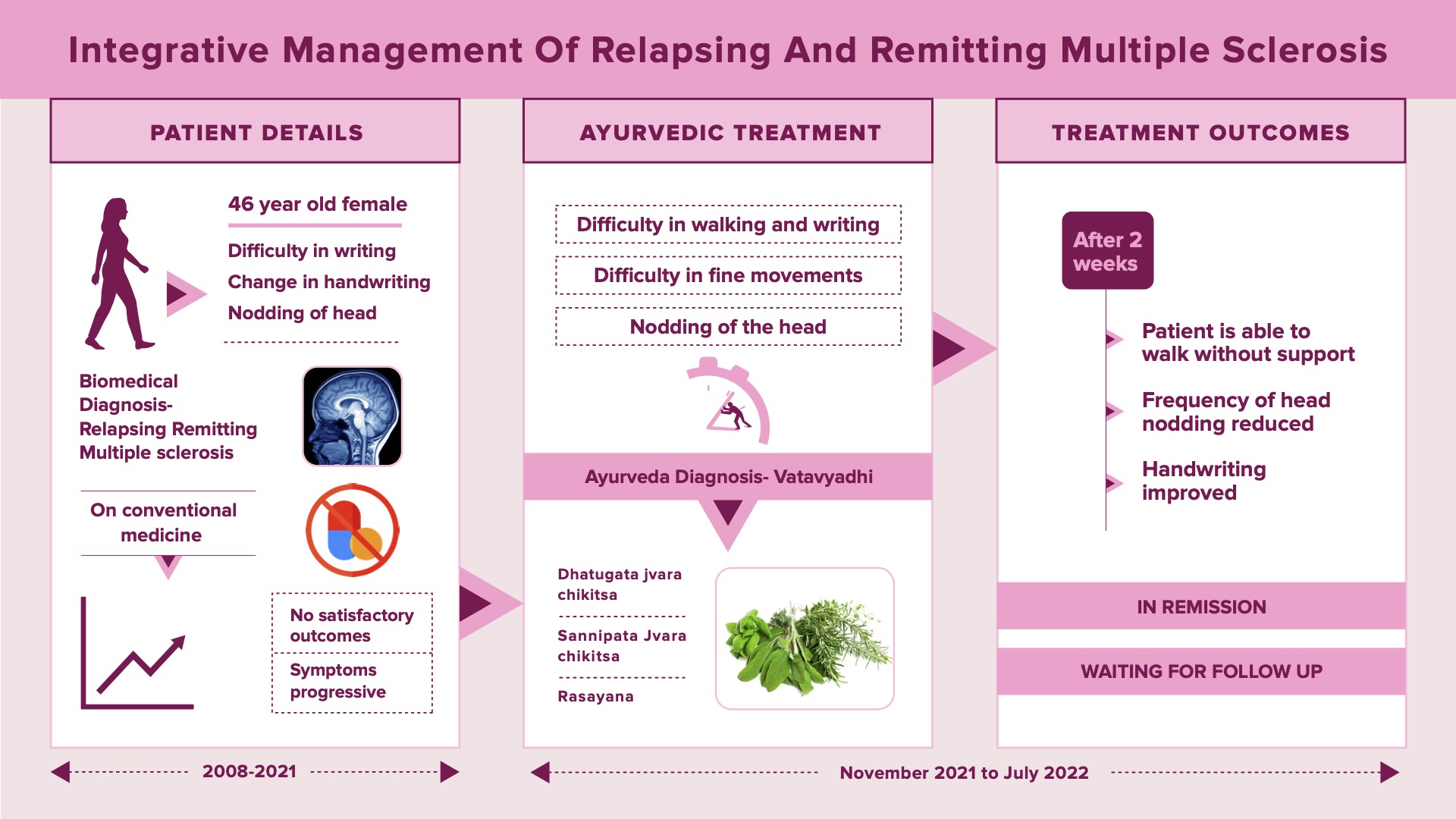
A 46-year-old female, diagnosed with Multiple sclerosis presented with difficulty in walking, writing, and fine movements asoociated with involuntary nodding of the head since 2 years. The patient was normal until 14 years back. In 2008, she developed a sudden blurring of vision for which she took the standard of care. She was diagnosed with Retrobulbar neuritis. Etiological workup was done, and she was discharged. Based on MRI findings, she was provisionally diagnosed as Multiple Sclerosis. Her vision was recovered but had fatigue that she managed with home remedies. In 2009, the condition relapsed. The biomedical diagnosis was confirmed as Relapsing-remitting Multiple sclerosis with Brain MRI. By 2014, the patient developed difficulty in writing, she noticed that her handwriting started changing. By 2019, the symptoms worsened, and she developed nodding of head, an inability to walk and repeated episodes of tremors. In spite of taking conventional medicines, the outcome was not satisfactory. In 2021, she consulted Dr Shibu Varghese. The ayurvedic diagnosis was Vatavyadhi. The line of treatment followed was to correct dhatvagni, adopt dhatugata and sannipata jvara cikitsa, use of tikta rasa followed by madhura rasa and rasayana cikitsa. The outcomes were assessed based on EDS Scale, Ambulation Index, and Neurologic physical examination. After 2 weeks of treatment, patient could walk without support. The frequency of head nodding reduced, handwriting of the patient has improved. The EDS scale that was 7 before treatment became 2 after ayurvedic treatment. The ambulation index was recorded 2 pre-treatments became 0 after treatment. The patient is continuing the medicines and advised to come for regular follow ups.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 46-year-old female, diagnosed with Multiple sclerosis presented with difficulty in walking, writing, and fine movements asoociated with involuntary nodding of the head since 2 years. The patient was normal until 14 years back. In 2008, she developed a sudden blurring of vision for which she took the standard of care. She was diagnosed with Retrobulbar neuritis. Etiological workup was done, and she was discharged. Based on MRI findings, she was provisionally diagnosed as Multiple Sclerosis. Her vision was recovered but had fatigue that she managed with home remedies. In 2009, the condition relapsed. The biomedical diagnosis was confirmed as Relapsing-remitting Multiple sclerosis with Brain MRI. By 2014, the patient developed difficulty in writing, she noticed that her handwriting started changing. By 2019, the symptoms worsened, and she developed nodding of head, an inability to walk and repeated episodes of tremors. In spite of taking conventional medicines, the outcome was not satisfactory. In 2021, she consulted Dr Shibu Varghese. The ayurvedic diagnosis was Vatavyadhi. The line of treatment followed was to correct dhatvagni, adopt dhatugata and sannipata jvara cikitsa, use of tikta rasa followed by madhura rasa and rasayana cikitsa. The outcomes were assessed based on EDS Scale, Ambulation Index, and Neurologic physical examination. After 2 weeks of treatment, patient could walk without support. The frequency of head nodding reduced, handwriting of the patient has improved. The EDS scale that was 7 before treatment became 2 after ayurvedic treatment. The ambulation index was recorded 2 pre-treatments became 0 after treatment. The patient is continuing the medicines and advised to come for regular follow ups.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Integrative successful treatment of Multiple Sclerosis
Dr Shibu Varghese
ABSTRACT
A 46-year-old female, diagnosed with Multiple sclerosis presented with difficulty in walking, writing, fine movements and involuntary nodding of the head since 2 years. The patient was normal until 14 years back. In 2008, she developed a sudden blurring of vision for which she took the standard of care. She was diagnosed with Retrobulbar neuritis. Etiological workup was done, and she was discharged. Based on MRI findings, she was provisionally diagnosed as Multiple Sclerosis. Her vision became normal but she developed fatigue that was managed with home remedies. In 2009, the condition relapsed. The biomedical diagnosis was confirmed as Relapsing-remitting Multiple sclerosis with Brain MRI. By 2014, the patient developed difficulty in writing, she noticed that her handwriting started changing. By 2019, the symptoms worsened, and she developed nodding of head, inability to walk and repeated episodes of tremors. In spite of taking conventional medicines, the outcome was not satisfactory. In 2021, she consulted Dr Shibu Varghese, for ayurvedic supportive management. The ayurvedic diagnosis was Vatavyadhi. The line of treatment was to correct dhatvagni, adopt dhatugata and sannipata jvara cikitsa, tikta rasa followed by madhura rasa prayoga and rasayana cikitsa. The outcomes were assessed based on EDS Scale, Ambulation Index, and Neurologic physical examination. After 2 weeks of treatment, patient could walk without support. The frequency of head nodding reduced, handwriting of the patient has improved. The EDS scale that was 7 before treatment became 2 after 2 weeks of ayurvedic treatment. Ambulation index was recorded 2 pre-treatment became 0 after treatment. The patient is continuing the medicines and advised to come for regular follow ups.
KEYWORDS
Multiple Sclerosis, Vata vyadhi, Ayurveda, Case report, Integrative
INTRODUCTION
Multiple sclerosis (MS) is a potentially disabling disease of the brain and spinal cord (central nervous system). In MS, the immune system attacks the protective sheath (myelin) that covers nerve fibres and causes communication problems between your brain and the rest of your body. Eventually, the disease can cause permanent damage or deterioration of the nerve fibres.
Signs and symptoms of MS vary widely between patients and depend on the location and severity of nerve fibre damage in the central nervous system. Some people with severe MS may lose the ability to walk independently or ambulate at all. Other individuals may experience long periods of remission without any new symptoms depending on the type of MS they have. The common symptoms are Numbness or weakness in one or more limbs that typically occurs on one side of your body at a time, Tingling, Electric-shock sensations, Lack of coordination, Unsteady gait or inability to walk, Partial or complete loss of vision, usually in one eye at a time, often with pain during eye movement, Prolonged double vision, Blurry vision, Vertigo and mood disturbances.
Disease course: Most people with MS have a relapsing-remitting disease course. They experience periods of new symptoms or relapses that develop over days or weeks and usually improve partially or completely. These relapses are followed by quiet periods of disease remission that can last months or even years. Some people with MS experience a gradual onset and steady progression of signs and symptoms without any relapses, known as primary-progressive MS.
Diagnosis: There are no specific tests for MS. Instead, a diagnosis of multiple sclerosis often relies on ruling out other conditions that might produce similar signs and symptoms, known as a differential diagnosis. Blood tests, MRI and spinal tap will help ruling out other major pathologies.
PATIENT INFORMATION
A 46-year-old female, diagnosed with Multiple sclerosis presented with difficulty in walking, writing, fine movements and nodding of the head since 2 years.
Medical History: The patient was normal until 14 years back. In 2008, she developed a sudden blurring of vision for which she took the standard of care. She was diagnosed with Retrobulbar neuritis. Etiological workup was done, and she was discharged. Based on MRI findings, she was provisionally diagnosed as Multiple Sclerosis. Her vision was recovered but developed fatigue that she managed with home remedies. In 2009, the condition relapsed. The biomedical diagnosis was confirmed as Relapsing-remitting Multiple sclerosis with Brain MRI. By 2014, the patient developed difficulty in writing, she noticed that her handwriting started changing. By 2019, the symptoms worsened, and she developed nodding of head, an inability to walk and repeated episodes of tremors. In spite of taking conventional medicines, the outcome was not satisfactory. In 2021, she consulted Dr Shibu Varghese for trying supportive ayurvedic treatments. The ayurvedic diagnosis was Vatavyadhi. The line of treatment was to correct dhatvagni, adopt dhatugata and sannipata jvara cikitsa, tikta rasa followed by madhura rasa prayoga and rasayana cikitsa
CLINICAL FINDINGS/PHYSICAL EXAMINATION
General examination: PR - 68 bpm, HR- 68 bpm, BP-110/70 mm/Hg
Table 1. Nervous system examination at baseline added below
Reflex
Right side
Left side
Biceps
3
3
Triceps
3
3
Knee
4
4
Ankle
3
3
Supinator
3
3
Babinski reflex
Positive
Positive
Cortical
Tactile localisation: Intact
Graphesthesia: Not able to identify some letters like M, S, N etc
Cerebellar
Tandem Walking- Slightly possible
Heel walking- Not possible
Toe walking - Not possible
Sensory: Superficial, touch, temperature and pain intact
Deep: Crude touch, vibration, joint sense and position – present
EDSS/EDS Expanded Disability Status Scale:
At baseline documented as 7 (More severe disability impairing one's daily activity and requiring assistance )
Ambulation Index (A1)
At baseline – Left hand 2, Right hand 3.
Shrugging of shoulders- Possible
Turning the neck- With a slight tremor
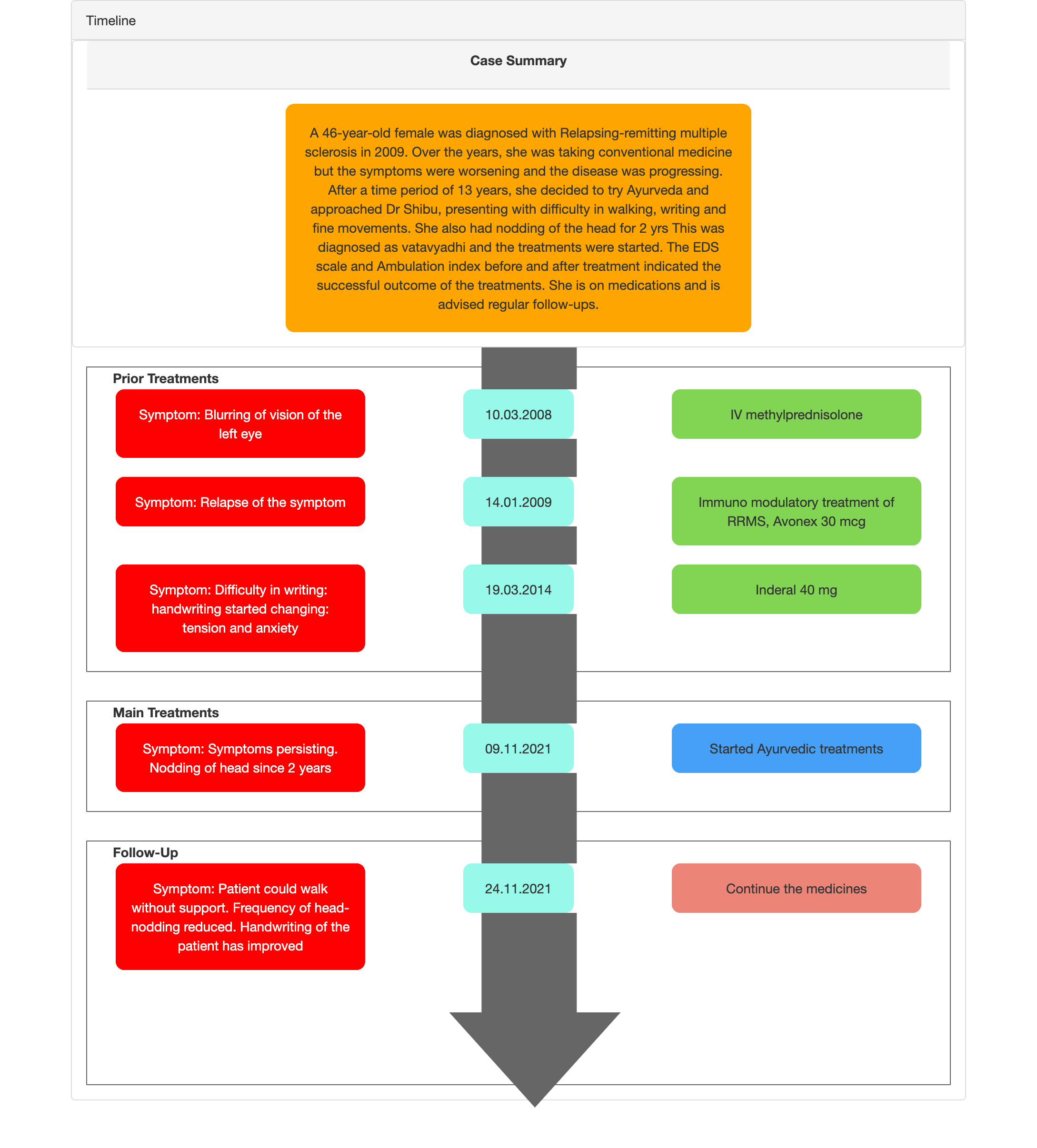
TIMELINE
Image 1. Timeline of events attached below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The patient was a known case of Relapsing remitting multiple sclerosis.
Image 2. Diagnosis proof document dated 2009 added below
Image 3. RRMS graph drawn by the treating physician added below
Ayurvedic Assessment was done based on the clinical evaluation by the ayurvedic physician.
Differential Diagnosis- This does not apply as the patient came with a confirmed diagnosis.
Prognosis- The condition is often mild at the early stages and as it progresses, the symptoms worsens. The prognosis varies widely for RRMS. Some patients rarely have flare ups and go years without having new clinical problems. Others have frequent attacks and require extensive medication treatment. In this case report, in spite of taking conventional medicine, the disease was progressing and symptoms were worsening. With ayurvedic treatments, the patient was able to regain fine movements in 2 weeks.
THERAPEUTIC INTERVENTION
See the tab ‘Treatment details’
FOLLOW-UP AND OUTCOMES
Clinician-based assessment;
Before treatment - Patient walked with support and after treatment- patient could walk without any support.
Frequency of head-nodding reduced.
Video 1. Patient is able to read verses without nodding of head
Video 2. Patient is able to walk without support
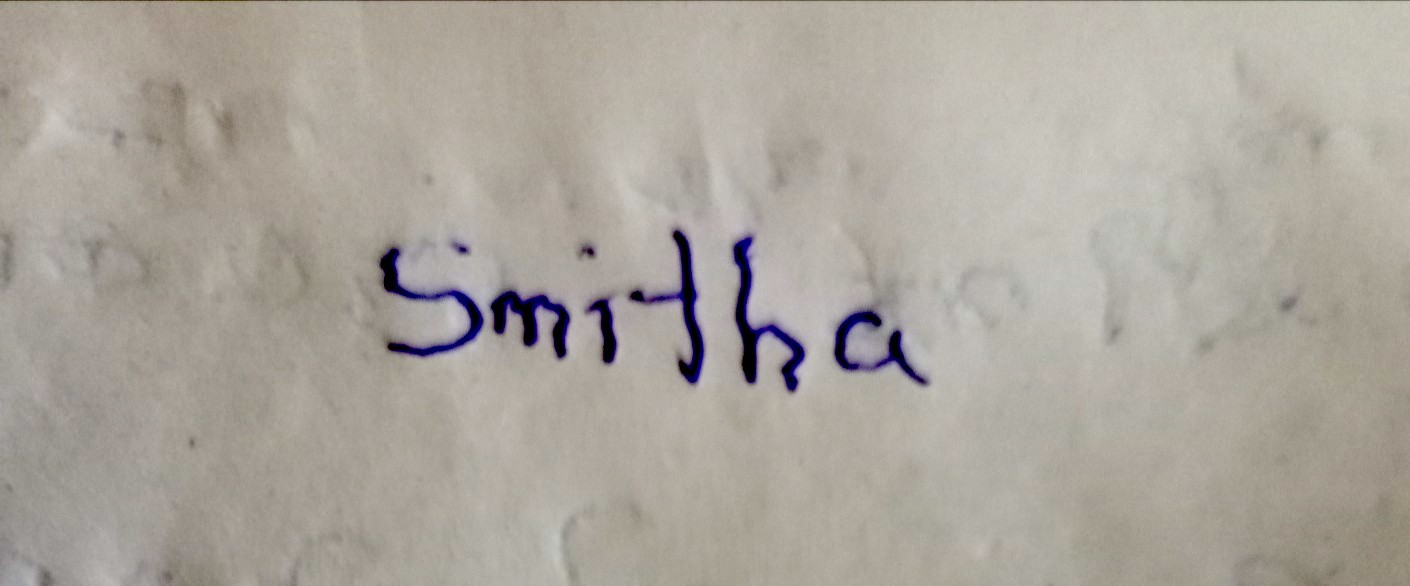
Handwriting of the patient has improved.
The EDS scale was 7 before treatment became 2 after 2 weeks of ayurvedic treatment.
Ambulation index: Left hand was 2 before treatment became 0 and right hand was 3 before treatment became 1 after 2 weeks of treatment.
RRMS graph shows the disease is now stable without any activity.
Table 2. Coordination tests documented before and after ayurvedic treatment added below
On the day of admission
After Udwarthanam
After fulll treatment
Finger to nose test
Not possible
Possible with effort
Possible
Finger test
Not possible
Possible with effort
Possible
Knee-heel test
Possible
Possible with effort
Possible
Dysdiadochokinesia
Not possible
Possible with effort
Possible
Table 3. Fine movements documented before and after treatment.
Fine movement
On the day of admission
After 1 week
After Udwarthanam
Grain picking
Unable
30 grains
250 grains
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported.
DISCUSSION ;
The treatments given were: dhatugata jwara cikitsa, sannipata jwara cikitsa, tikta rasa prayoga followed by madhura rasa prayoga and rasayana cikitsa.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
This case report demonstrates the successful ayurvedic management of multiple sclerosis, in a A 46-year-old female patient, who was suffering from relapsing remitting Multiple sclerosis,with the symptoms progressing and worsening over time.
INFORMED CONSENT
Written consent was obtained from the patient to publish the case report.
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
- Mayo Clinic. Multiple Sclerosis. https://www.yahoo.com
_________________________________________________________________________________________________________________
Image 1. Timeline of events
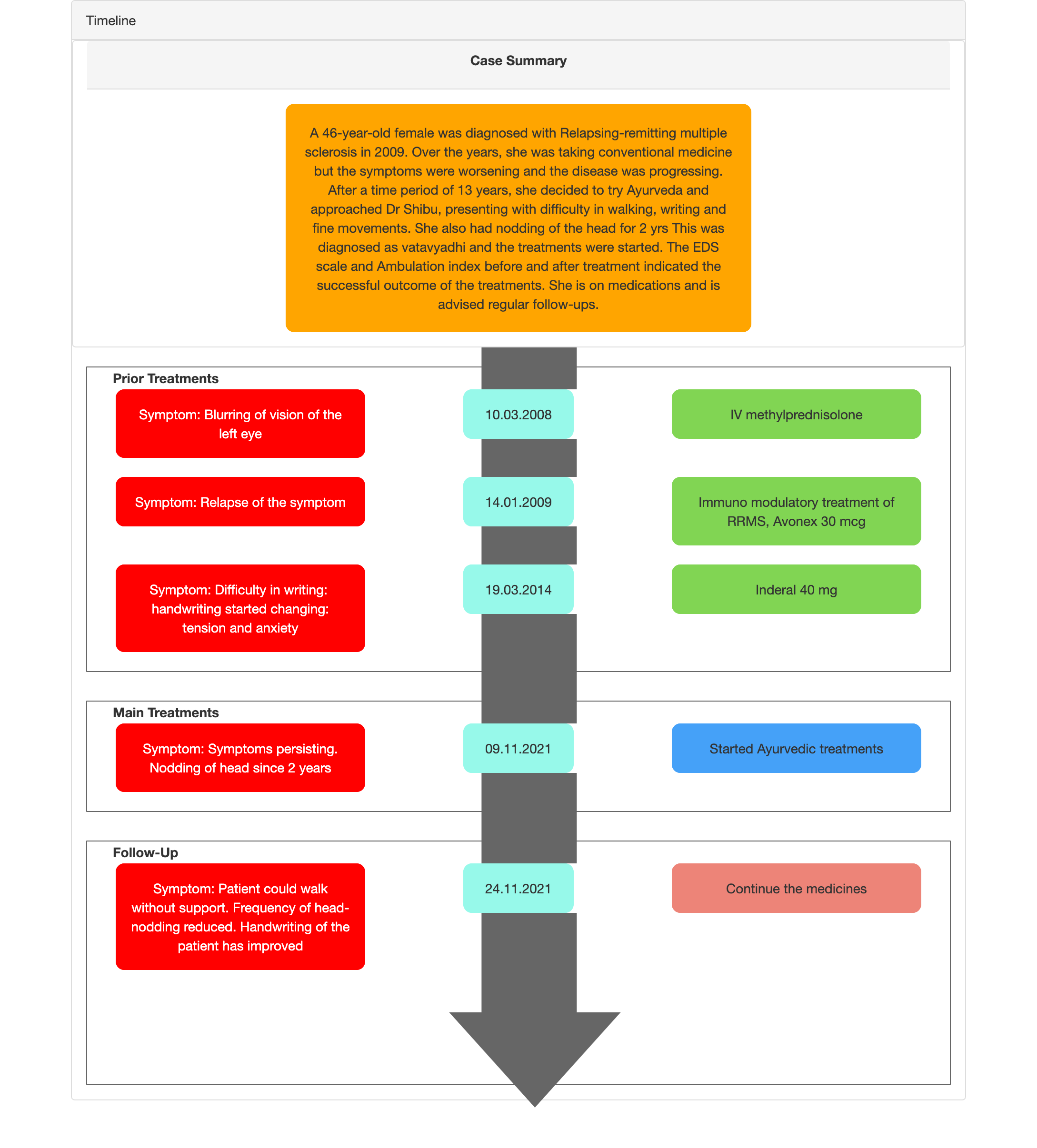
Image 2. Diagnosis proof document dated 2009 added below
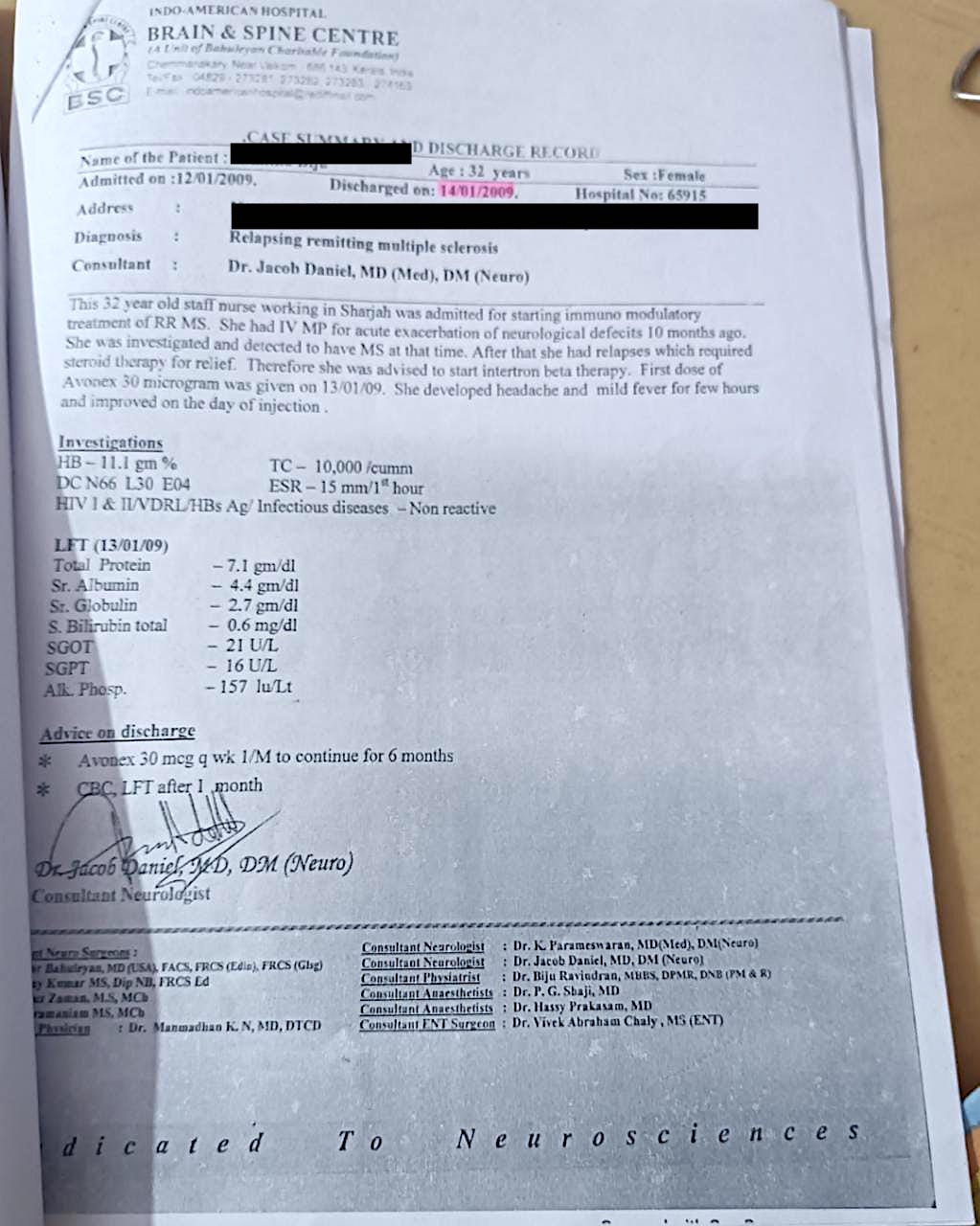
Image 3. RRMS graph drawn by the treating physician added below
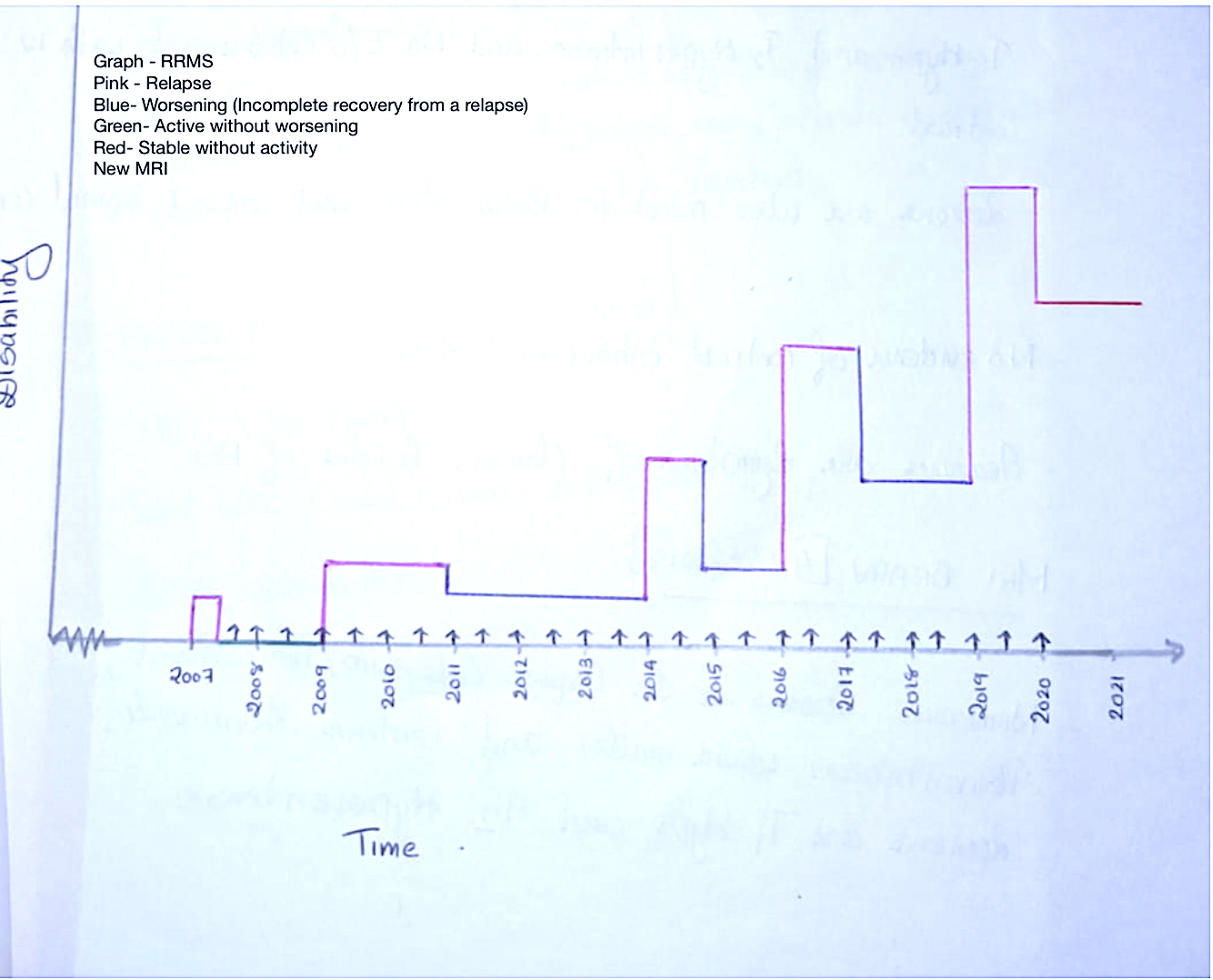
Image 4. Handwriting of the patient before treatment added below
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Multiple sclerosis (MS)
ABOUT THE DISEASE:
Multiple sclerosis (MS) is a potentially disabling disease of the brain and spinal cord (central nervous system). In MS, the immune system attacks the protective sheath (myelin) that covers nerve fibres and causes communication problems between your brain and the rest of your body. Eventually, the disease can cause permanent damage or deterioration of the nerve fibres.
Signs and symptoms of MS vary widely between patients and depend on the location and severity of nerve fibre damage in the central nervous system. Some people with severe MS may lose the ability to walk independently or ambulate at all. Other individuals may experience long periods of remission without any new symptoms depending on the type of MS they have. The common symptoms are Numbness or weakness in one or more limbs that typically occurs on one side of your body at a time, Tingling, Electric-shock sensations, Lack of coordination, Unsteady gait or inability to walk, Partial or complete loss of vision, usually in one eye at a time, often with pain during eye movement, Prolonged double vision, Blurry vision, Vertigo and mood disturbances.
Disease course: Most people with MS have a relapsing-remitting disease course. They experience periods of new symptoms or relapses that develop over days or weeks and usually improve partially or completely. These relapses are followed by quiet periods of disease remission that can last months or even years. Some people with MS experience a gradual onset and steady progression of signs and symptoms without any relapses, known as primary-progressive MS.
In this case report, the patient is a 46-year-old female, diagnosed with Multiple sclerosis who presented with difficulty in walking, writing, and fine movements associated with nodding of the head for 2 years. The patient was normal until 14 years back. In 2008, she developed a sudden blurring of vision for which she took the standard of care. She was diagnosed with Retrobulbar neuritis. An etiological workup was done, and she was discharged. Based on MRI findings, she was provisionally diagnosed with Multiple Sclerosis. Her vision was recovered but developed fatigue that she managed with home remedies. In 2009, the condition relapsed. The biomedical diagnosis was confirmed as Relapsing-remitting Multiple sclerosis with Brain MRI.
By 2014, the patient developed difficulty in writing, she noticed that her handwriting started changing. By 2019, the symptoms worsened, and she developed nodding of the head, an inability to walk and repeated episodes of tremors. Despite taking conventional medicines, the outcome was not satisfactory.
Diagnosis: There are no specific tests for MS. Instead, a diagnosis of multiple sclerosis often relies on ruling out other conditions that might produce similar signs and symptoms.. Blood tests, MRI and spinal tap will help in ruling out other major pathologies.
Image 1. Diagnosis proof document dated 2009 added below
Image 2. RRMS graph drawn by the treating physician added below
There's no cure for multiple sclerosis. However, there are treatments to help speed the recovery from attacks, modify the course of the disease and manage the symptoms.
Reference
- Mayo Clinic. Multiple Sclerosis. https://www.yahoo.com
Image 1. Diagnosis proof document dated 2009
Image 2. RRMS graph drawn by the treating physician
Image 3. Handwriting of the patient before starting the treatment
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Vatavyadhi
ABOUT THE DISEASE:
Vatavyadhi are group of disorders that caused by vitiated vata dosa. They are 80 in number. The classical textbooks explain in detail about the Vatavyadhi, whereas there is no specific chapter dealing with diseases of vitiated pitta or kapha.
Causative factors: Vata vitiation is the main reason for the manifestation of vatavyadhi. Vata gets vitiated by 2 causes- Dhatu kshaya and by Margavarodha.
Samprapti: The aggravated Vata vitiates Strotas with its laghu, ruksha, khara, parusha guna and makes these rikta srotas susceptible to sthansanshraya of dosha. Commenting on Rikta Strotas, Chakrapani elaborated that there is “Snehadi Guna Shunyatvam”. The channels of the body lost their protective sheaths and lost qualities like unctuousness, smoothness and stickiness etc. On occupying the susceptible srotas the vitiated Vata will produce Ekanga (limited to particular parts of the body) or Sarvanga (afflicting the whole body) Vyadhi. Such Vyadhi which is manifested either in a certain portion of the body or the whole body is called Vata Vyadhi. This can present as akarmanyata, shula, supta, sthambha, shosha, raukshya, kriyatmaka and racanatmaka vikruti, and manasika lakshanas.
Classification of vatavyadhi: This can be ashayagata, dhatugata, indriyagata or avrita vata. The symptoms will vary depending upon the sthana where the vitiated vata has manifested.
Sadhyasadhyata: Sandhichuti, Hanustambha, Kunjan, Kubjatva, Ardita, Pakshaghata, Ansashosha, Pangutva Khuddavata, Stambha, Aadhyavata and Majja Asthi Gata Vatavyadhi all these are asadhya. When the disease if of recent origin and the patient is balya, then it can be sadhya or kricchrasadhya.
In this case report, the patient is a known case of Multiple sclerosis and presented with difficulty in walking, writing, fine movements and tremors of the head for 2 years. The ayurvedic diagnosis given by the treating physician was Vatavyadhi, the exact subtype was not specified.
Rationale of treatment: To correct dhatvagni. The line of treatment followed was as follows:
dhatugata jwara cikitsa
sannipata jwara cikitsa
tikta rasa prayoga followed by madhura rasa prayoga
rasayana cikitsa
Reference:
- Archana A Kulkarni et al. Review of Vatavyadhi WSR to Carak Samhita. International Ayurvedic Medical Journal 2021. Available from http://www.iamj.in/posts/2021/images/upload/743_753.pdf
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Maharasnadi Kasayam Kasaya 15 ml + 60 ml of warm water On empty stomach at 6 am and 6 pm 2021-11-11 - 2021-11-24 Sahasra yogam, Kasaya prakaranam Aswagandharistam Arishta 30 ml Twice daily after food 2021-11-11 - 2021-11-24 Bhaishajya ratnavali. Murcharogadhikara Chandraprabha vati Vati 1-0-1 Twice daily after food 2021-11-11 - 2021-11-24 Sharngadhara Samhita. Madhyama Khanda. Vata kalpana.7 Palsipyrin Tab Tablet 1-0-1 Twice daily after food 2021-11-11 - 2021-11-24 Patent * Proprietary medicine Avipatti kara churna + Godanti Bhasma + Abhraka Bhasma Powder Abhraka Bhasma (2.5) quantity specified Twice daily after food 2021-11-11 - 2021-11-24 Avipattikara- Sahasra yogam. Curna prakarana: Godanti Bhasma- Rasatarangini.11.241: Abhraka bhasma- rasatarangini 10.39-42 Neurodiet Tab Tablet 1-0-0 Once daily after food 2021-11-11 - 2021-11-24 Patent * Proprietary medicine Swasasphatikamrutham Syrup 10 ml + 60 ml warm water Twice daily after food 2021-11-11 - 2021-11-24 Patent * Proprietary medicine Kolakulathadi curnam Curna Required quantity Udhvartanam 2021-11-11 - 2021-11-19 CS.Su.3.18 Shashtika Sveda dravya Required quantity Kizhi 2021-11-20 - 2021-11-24 Keraliya kriyakarma -
Outcome Measures
OUTCOME MEASURES
A 46-year-old female, diagnosed with Multiple sclerosis presented with difficulty in walking, writing, and fine movements associated with involuntary nodding of the head for 2 years. The patient was normal until 14 years back. In 2008, she developed a sudden blurring of vision for which she took the standard of care. She was diagnosed with Retrobulbar neuritis. An etiological workup was done, and she was discharged. Based on MRI findings, she was provisionally diagnosed as Multiple Sclerosis. Her vision was recovered but developed fatigue that she managed with home remedies. In 2009, the condition relapsed. The biomedical diagnosis was confirmed as Relapsing-remitting Multiple sclerosis with Brain MRI. By 2014, the patient developed difficulty in writing, she noticed that her handwriting started changing. By 2019, the symptoms worsened, and she developed nodding of the head, an inability to walk and repeated episodes of tremors. In spite of taking conventional medicines, the outcome was not satisfactory. In 2021, she consulted Dr Shibu Varghese to try supportive ayurvedic treatments. The Ayurvedic diagnosis was Vatavyadhi. The line of treatment was to correct dhatvagni, adopt dhatugata and sannipata jvara cikitsa, tikta rasa followed by madhura rasa prayoga and rasayana cikitsa.
Assessment criteria: Subjective parameters were used to assess the treatment outcomes.
Subjective parameters:
Before treatment – the patient walked with support and after treatment- the patient could walk without any support. Frequency of head-nodding reduced. The handwriting of the patient has improved.
The EDS scale was 7 before treatment became 2 after 2 weeks of treatment. The ambulation index was 2 before treatment and became 0 after 2 weeks of treatment.
Video 1. Patient is able to read verses without involuntary nodding of head
Video 2. Patient is able to walk without support
Table 1. Coordination tests documented before and after ayurvedic treatment added below
On the day of admission
After Udwarthanam
After fulll treatment
Finger to nose test
Not possible
Possible with effort
Possible
Finger test
Not possible
Possible with effort
Possible
Knee-heel test
Possible
Possible with effort
Possible
Dysdiadochokinesia
Not possible
Possible with effort
Possible
Table 2. Fine movements documented before and after treatment.
Fine movement
On the day of admission
After 1 week
After Udwarthanam
Grain picking
Unable
30 grains
250 grains
Disease-modifying effect: The patient is in remission.
Image 1. The handwriting of the patient after Ayurvedic treatment is added below
-