Featured Case
-
Abstract
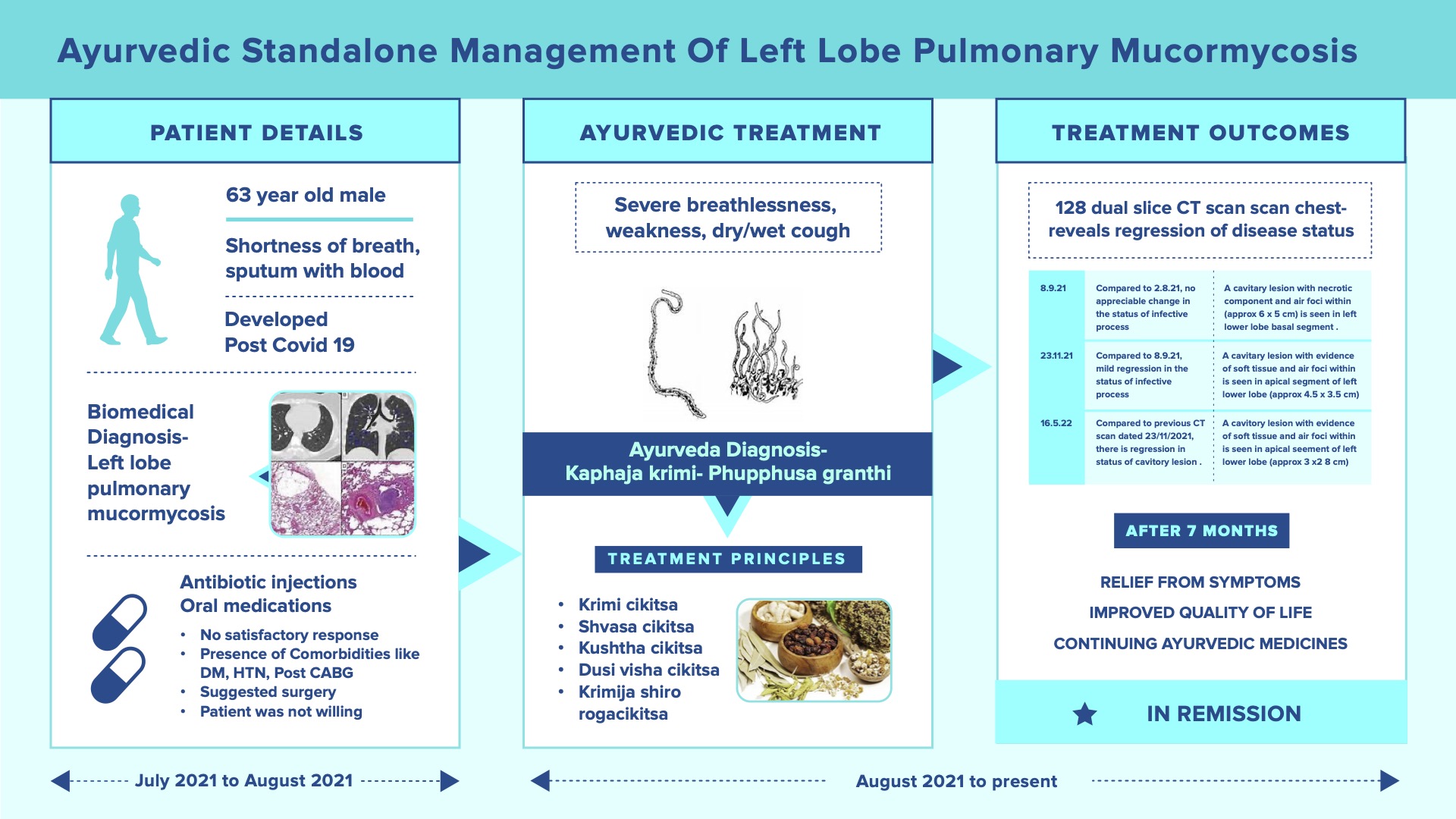
A 63-year-old male patient was suffering from severe breathlessness even when engaged in a simple activity like walking, standing up, or climbing stairs; severe weakness, cough (Dry and Wet) sometimes with fresh blood and weight loss in August 2021. He had a history of Covid 19 Pneumonitis on 10.6.21. Post covid he took 1 week of Inpatient treatment at Orange Hospital for generalized weakness and decreased oral intake (21.6.21- 28.6.21). HRCT Lungs revealed a left lower lobe lesion with consolidation and Bronchoscopy + BAL was planned. The sample was sent for further investigation in which Bacterial C/5 showed Pseudomonas aeruginosa isolated and started antibiotics. Biopsy revealed Fungal Hyphae and Inj Amphotericin B (5 doses given). Follow-up HRCT lungs revealed the same left lobe consolidation lesion and advised surgery and meanwhile continue Injection Amphotericin- B. The risk of surgery and its grave prognosis taking into consideration the age, history of CABG, LV Dysfunction and DM, and HTN were explained to the family. So, the family requested discharge and then approached Dr Rajnikanth. The ayurvedic diagnosis was Kaphaja krimi (Fuffusa gata) and treated along the principles of Krimiroga cikitsa. The treatment principles mentioned for kaphaja krimi, kushta, asthimajjagata kushtha, krimijanya shiroroga, dushivisa, shvasa and raktaja krimi were followed. Within 1 week of starting Ayurvedic medicines, there was an improvement in symptoms. The assessment pre and post-treatment were done based on a 128 Slice Dual Energy CT scan of the chest. The scan done on 16.5.22, showed significant regression in the lung lesions. He is continuing the ayurvedic medicine and is in remission.
-
Summaries
-
Listen
-
Watch
-
View
-
Read

A 63-year-old male patient was suffering from severe breathlessness even when engaged in a simple activity like walking, standing up, or climbing stairs; severe weakness, cough (Dry and Wet) sometimes with fresh blood and weight loss in August 2021. He had a history of Covid 19 Pneumonitis on 10.6.21. Post covid he took 1 week of Inpatient treatment at Orange Hospital for generalized weakness and decreased oral intake (21.6.21- 28.6.21). HRCT Lungs revealed a left lower lobe lesion with consolidation and Bronchoscopy + BAL was planned. The sample was sent for further investigation in which Bacterial C/5 showed Pseudomonas aeruginosa isolated and started antibiotics. Biopsy revealed Fungal Hyphae and Inj Amphotericin B (5 doses given). Follow-up HRCT lungs revealed the same left lobe consolidation lesion and advised surgery and meanwhile continue Injection Amphotericin- B. The risk of surgery and its grave prognosis taking into consideration the age, history of CABG, LV Dysfunction and DM, and HTN were explained to the family. So, the family requested discharge and then approached Dr Rajnikanth. The ayurvedic diagnosis was Kaphaja krimi (Fuffusa gata) and treated along the principles of Krimiroga cikitsa. The treatment principles mentioned for kaphaja krimi, kushta, asthimajjagata kushtha, krimijanya shiroroga, dushivisa, shvasa and raktaja krimi were followed. Within 1 week of starting Ayurvedic medicines, there was an improvement in symptoms. The assessment pre and post-treatment were done based on a 128 Slice Dual Energy CT scan of the chest. The scan done on 16.5.22, showed significant regression in the lung lesions. He is continuing the ayurvedic medicine and is in remission.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Successful ayurvedic standalone management of Left Lobe Pulmonary Mucormycosis
Dr Rajnikanth
ABSTRACT
A 63-year-old male patient was suffering from severe breathlessness even when engaged in a simple activity like walking, standing up, or climbing stairs; severe weakness, coughing (Dry and Wet) sometimes with fresh blood and weight loss in August 2021. He had a history of Covid 19 Pneumonitis on 10.6.21. Post covid he took 1 week of Inpatient treatment at Orange Hospital for generalized weakness and decreased oral intake (21.6.21- 28.6.21). HRCT Lungs revealed a left lower lobe lesion with consolidation and planned for Bronchoscopy + BAL and the sample was sent for further investigation in which Bacterial C/5 showed Pseudomonas aeruginosa isolated and started antibiotics. Biopsy revealed Fungal Hyphae and Inj Amphotericin B (5 doses given). Follow-up HRCT lungs revealed the same left lobe consolidation lesion and advised surgery and meanwhile continue Injection Amphotericin- B. The risk of surgery and its grave prognosis taking into consideration the age, history of CABG, LV Dysfunction and DM, and HTN were explained to the family. So, the family requested discharge and then approached Dr Rajnikanth. The ayurvedic diagnosis was Kaphaja krimi (Fuffusa gata) and treated along the principles of Krimiroga cikitsa. The treatment principles mentioned for kaphaja krimi, kushtha, asthimajjagata kuṣṭha, krimijanya shiroroga, dushivisa, shvasa and raktaja krimi were followed. Within 1 week of starting Ayurvedic medicines, there was an improvement in symptoms. The assessment pre and post-treatment were done based on a 128 Slice Dual Energy CT scan of the chest. The scan done on 16.5.22, showed significant regression in the lung lesions. He is continuing the ayurvedic medicine and is in remission.
KEYWORDS
Standalone, Pulmonary Mucormycosis, Kaphaja Krimi, Phuphusa granthi, Krimi, Aspergillosis, 128 Slice Dual Energy CT
INTRODUCTION
Pulmonary mucormycosis and aspergillosis are rare, and life-threatening infections are caused due to fungi. The documentation available on the clinical cases is in patients suffering from neutropenia, diabetes mellitus, or undergoing treatment involving corticosteroids. These two conditions have been identified as secondary complications in COVID-19 patients, predominantly in critically sick patients.
Diagnostic Criteria; The diagnosis of mucormycosis is made by identifying the causative fungal organisms with the help of histopathological analysis of tissue samples from patients presenting with specific signs and symptoms. From the culture tests, the diagnosis and the causative organism can be confirmed.
Symptoms; The more frequent symptoms are fever, non-productive cough, and progressive dyspnea. The less frequent symptoms are Pleuritic chest pain, pleural effusion and hemoptysis. If the major pulmonary blood vessels are invaded by the hyphae, then it can cause life-threatening hemoptysis. The infection can also spread to the adjacent organs like the diaphragm, pleura and chest wall.
Treatment options; Initial treatment of mucormycosis starts with an early aggressive surgical debridement of the tissues that are affected. Then they are combined with amphotericin B deoxycholate (AmB) or liposomal amphotericin B (L-AmB).
Prognosis: Early detection of Black Fungus can be successfully treated. But if the patient does not respond to the antibiotic treatment, it can cause grave complications like blindness, bone infection, meningitis, brain abscess, sepsis and haemorrhage in the infected organ. This 63-year-old male patient was diagnosed case of Left Lobe Pulmonary Mucormycosis (Aspergillosis) and tried Antibiotic Injection but did not respond. Surgery was advised, but the prognosis was grave owing to his age, Diabetes, Hypertension, and LV Dysfunction. But with Ayurvedic treatment, he got relief from his symptoms and the Dual Energy CT Scan showed a decrease in the lesions.
PATIENT INFORMATION
A 63-year-old male patient was suffering from severe breathlessness even when engaged in a simple activity like walking, standing up, or climbing stairs; severe weakness, cough (Dry and Wet) sometimes with fresh blood, and weight loss since July 2021.
Medical History: In July 2021, the patient got admitted to a modern hospital with complaints of shortness of breath on exertion, cough with blood-stained expectoration, generalised weakness for 4-5 days. H/O Covid-19 Pneumonitis on 10.6.21- treated conservatively at home. Post covid he took 1 week of Inpatient treatment at Orange Hospital for generalised weakness and decreased oral intake (21.6.21- 28.6.21). From the Hospital Records- On examination- The patient was oriented, tachypnoea +, vitals stable, RS- left lower lobe reps + with decreased air entry. HRCT Lungs revealed a left lower lobe lesion with consolidation and planned for Bronchoscopy + BAL and a sample was sent for further investigation in which Bacterial C/5 showed Pseudomonas aeruginosa isolated and started antibiotics. Biopsy revealed Fungal Hyphae and Inj Amphotericin B (5 doses given). Follow-up HRCT lungs revealed the same left lobe consolidation lesion. So surgery was recommended and meanwhile continue Inj Amphotericin- B. The risk of surgery and its grave prognosis taking into consideration the age, H/O CABG, LV Dysfunction, DM and HTN were explained to the family. So the family requested discharge and then opted for Ayurveda. The patient is a known diabetic since 8 years and Hypertensive since 5 years, and is on conventional medication for the same.
CLINICAL FINDINGS/PHYSICAL EXAMINATION
On 22.8.21- 30x22x30 size soft tissue density lesion (From the Treating Physician’s notes)
TIMELINE
Image 1. Timeline of events added below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The biomedical diagnosis was confirmed based on the clinical presentation and the Investigation reports.
Image 2. 128 Slice Dual Energy CT Scan of the Chest (P+C) dated 8.9.2021 added below
Ayurvedic Assessment was done based on the investigation reports and the clinical evaluation by the ayurvedic physician.
Differential Diagnosis- The diagnosis was confirmed with the 128 Slice Dual Energy CT Scan
Prognosis- Early detection of Black Fungus can be successfully treated. But if the patient does not respond to the antibiotic treatment, it can cause grave complications like blindness, bone infection, meningitis, brain abscess, sepsis and haemorrhage in the infected organ. This 63-year-old male patient was diagnosed case of Left Lobe Pulmonary Mucormycosis (Aspergillosis) and tried Antibiotic Injection but did not respond. Surgery was advised, but the prognosis was grave owing to his age, DM, HTN, and LV Dysfunction. But with Ayurvedic treatment, he got relief from his symptoms and the Dual Energy CT Scan showed a decrease in the lesions.
THERAPEUTIC INTERVENTION
See the tab ‘Treatment details’
FOLLOW-UP AND OUTCOMES
Clinician-based assessment; The patient appears better, and seems to be having a good satvabala, as compared to the debilitated look he had earlier. With just 1 week of Ayurvedic medications, an improvement was seen in symptoms. As on 23.11.21, all symptoms were relieved except for occasional blood in the sputum.
Patient-assessed: Not relevant.
Image 3. 128 Slice Dual Energy CT Scan of the Chest (P+C) dated 23.11. 2021 added below
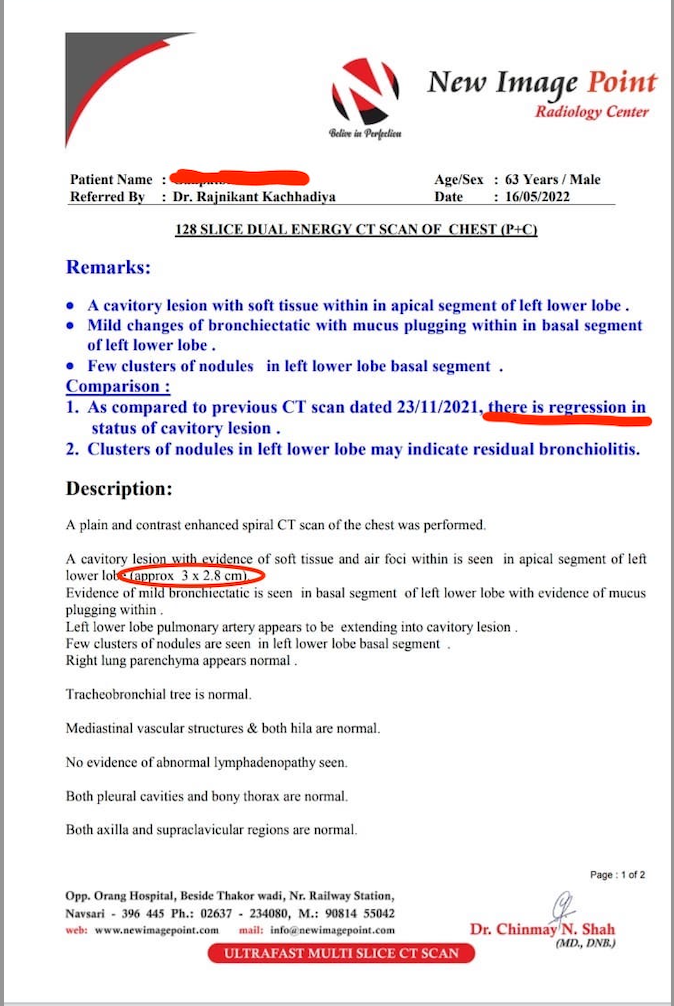
Image 4. 128 Slice Dual Energy CT Scan of the Chest (P+C) dated 16.5. 2022 added below
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient and the imaging done.
Adverse and unanticipated events; None reported.
DISCUSSION ;
Based on the clinical presentation and the CT Scan of the Chest reports, basically, Krimiroga cikitsa was followed. The treatment principles mentioned for Kaphaja Krmi, Kustha, Ashthimajjagata Kustha, Krmijanya siroroga, Dusivisa, Svasa and Raktaja Krimi were followed.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
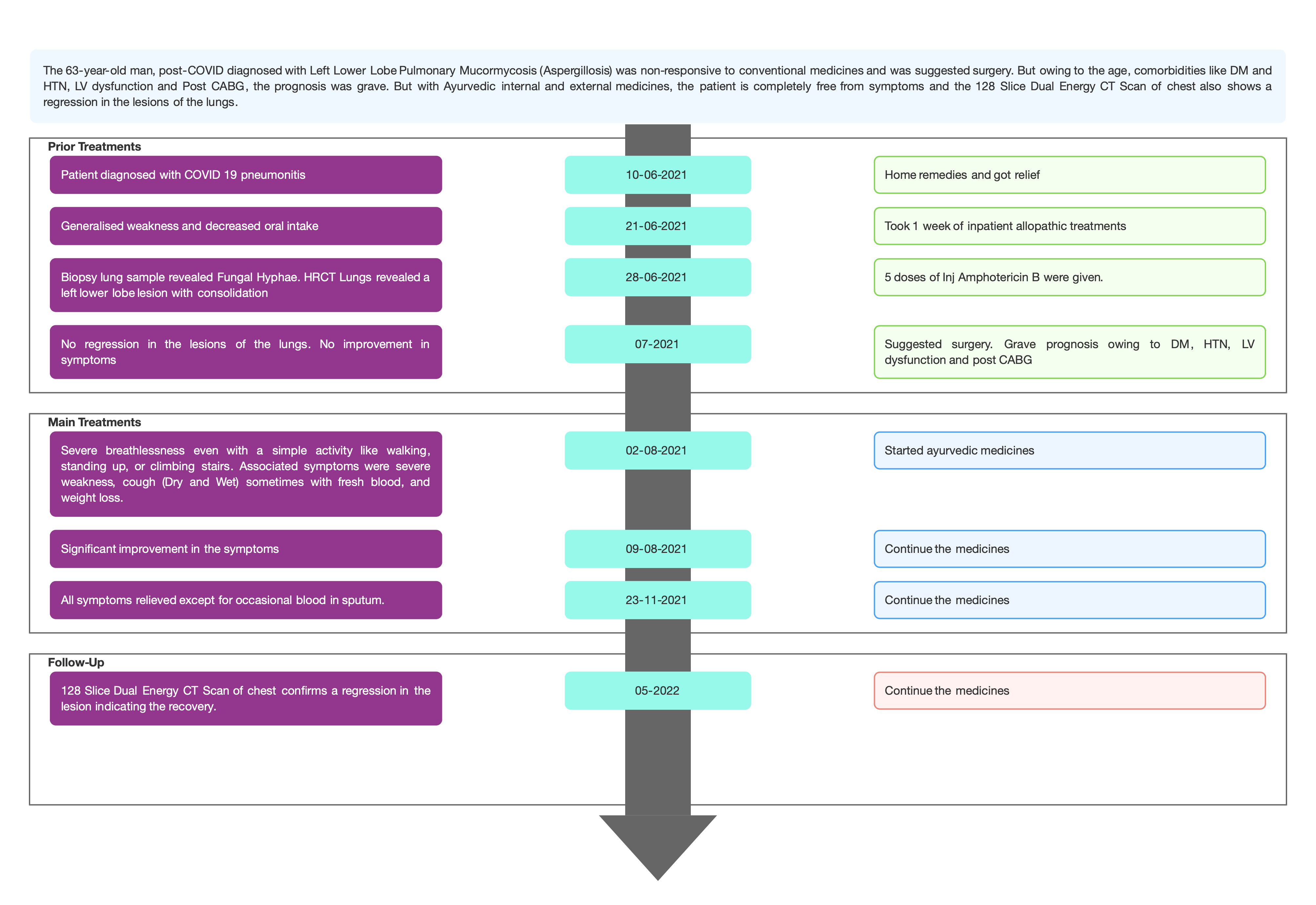
The 63-year-old man, post-COVID diagnosed with Left Lower Lobe Pulmonary Mucormycosis (Aspergillosis) was non-responsive to conventional medicines and was suggested surgery. But owing to the age, comorbidities like DM and HTN, LV dysfunction and Post CABG, the prognosis was grave. But with Ayurvedic internal and external medicines, the patient is completely free from symptoms and the 128 Slice Dual Energy CT Scan of chest also shows a regression in the lesions of the lungs.
INFORMED CONSENT
Written consent was obtained from the patient to publish the case report.
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
- Johnson AK, Ghazarian Z, Cendrowski KD, Persichino JG. Pulmonary aspergillosis and mucormycosis in a patient with COVID-19. Med Mycol Case Rep. 2021 Jun;32:64-67. doi: 10.1016/j.mmcr.2021.03.006. Epub 2021 Apr 7. PMID: 33842203; PMCID: PMC8025540.)
Image 1. Timeline of events
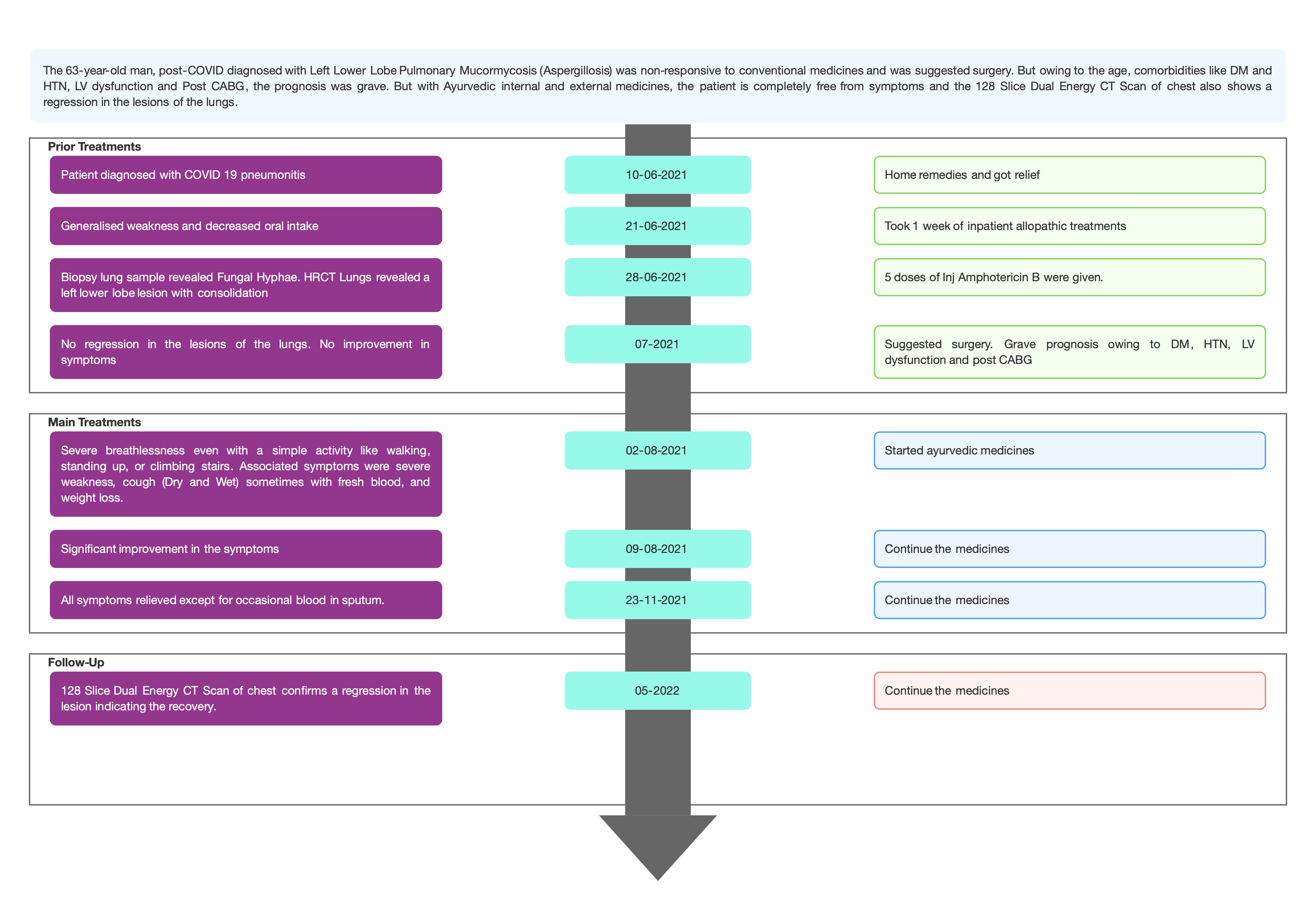
Image 2. 128 Slice Dual Energy CT Scan of the Chest (P+C) dated 8.9.2021
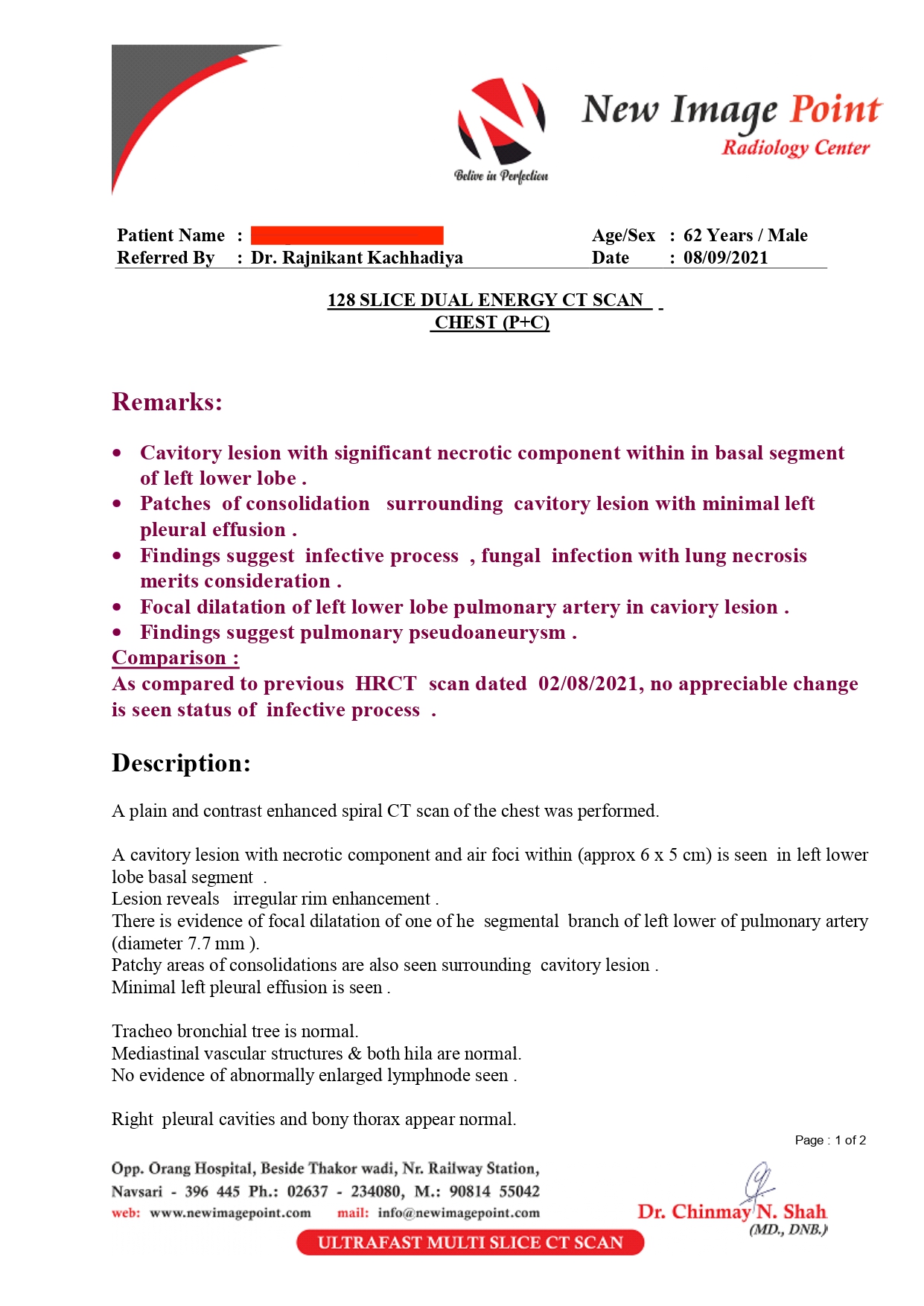
Image 3. 128 Slice Dual Energy CT Scan of the Chest (P+C) dated 23.11. 2021
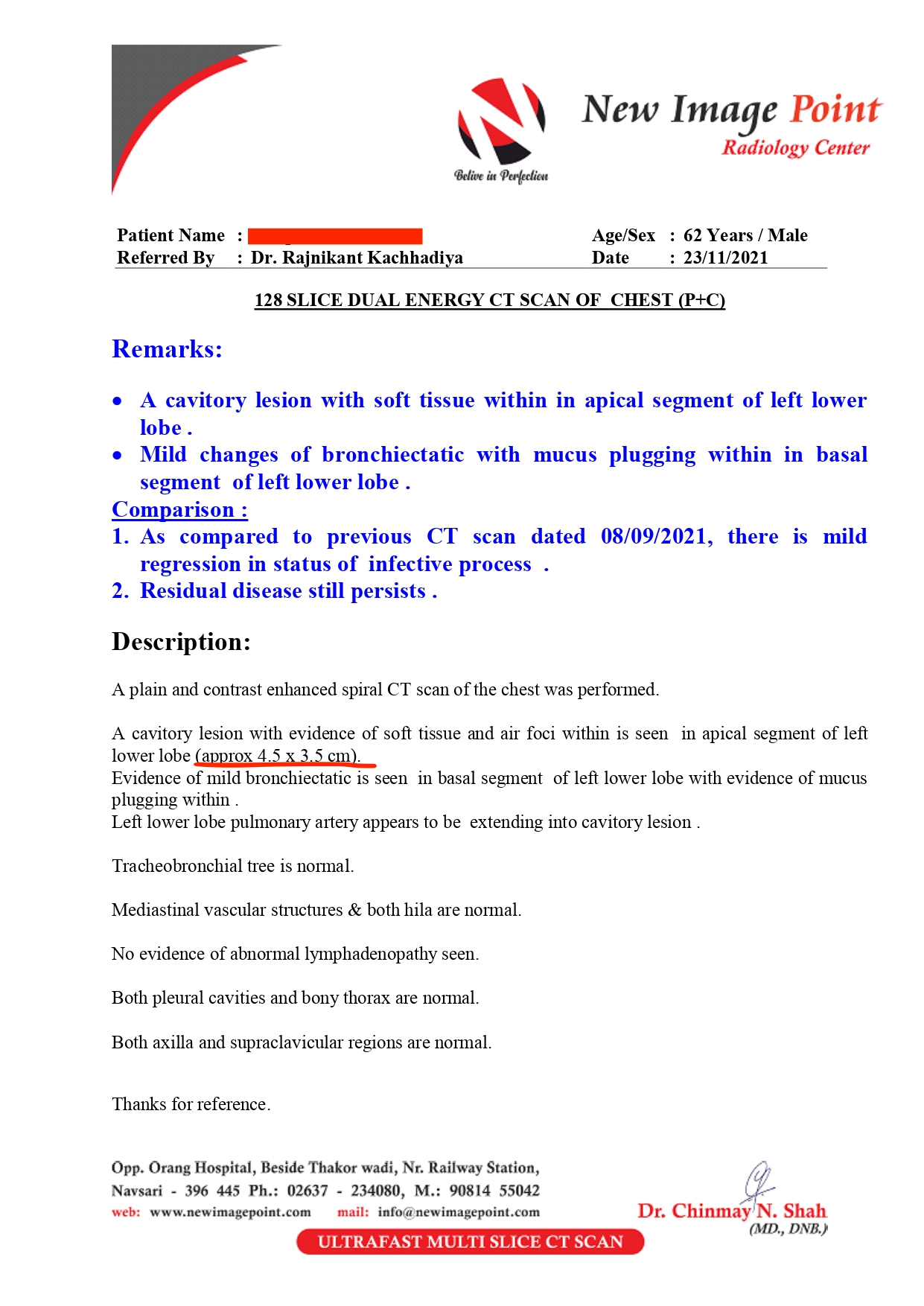
Image 4. . 128 Slice Dual Energy CT Scan of the Chest (P+C) dated 16.5. 2022
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS- Left Lobe Pulmonary Mucorrmycosis (Aspergillosis)
ABOUT THE DISEASE:
Pulmonary mucormycosis and aspergillosis are rare, and life-threatening infections caused due to fungi. The documentation available on the clinical cases is in patients suffering from neutropenia, diabetes mellitus, or undergoing treatment involving corticosteroids. These two conditions have been identified as secondary complications in COVID-19 patients, predominantly in critically sick patients. (Johnson AK, Ghazarian Z, Cendrowski KD, Persichino JG. Pulmonary aspergillosis and mucormycosis in a patient with COVID-19. Med Mycol Case Rep. 2021 Jun;32:64-67. doi: 10.1016/j.mmcr.2021.03.006. Epub 2021 Apr 7. PMID: 33842203; PMCID: PMC8025540.)
Diagnostic Criteria; The diagnosis of mucormycosis is made by identifying the causative fungal organisms by doing the histopathological analysis of tissue samples from patients presenting with specific signs and symptoms. From the culture tests, the diagnosis and the causative organism can be confirmed.
This patient is a 63-year-old male, who was a post-COVID-19 patient. His diagnosis of Left lobe pulmonary mucormycosis was confirmed based on the clinical presentation and by a 128 Slice Dual Energy CT Scan of the Chest (P+C) which revealed a fungal infection with lung necrosis. A lesion with necrotic component and air foci within (approx. 6 x 5 cm) is seen in the left lower lobe basal segment dated 8.9.21. The report also states that as compared to the previous HRCT Scan dated 2/8/21, there is no appreciable change.
Image 1. 128 Slice Dual Energy CT Scan of the Chest (P+C) dated 8.9.2021 added below
Symptoms; The more frequent symptoms are fever, nonproductive cough, and progressive dyspnea. The less frequent symptoms are Pleuritic chest pain, pleural effusion and hemoptysis. If the major pulmonary blood vessels are invaded by the hyphae, then it can cause life-threatening hemoptysis. The infection can also spread to the adjacent organs like the diaphragm, pleura and chest wall.
This patient presented with severe breathlessness even when engaged in a simple routine activity like walking, standing up, or climbing stairs; severe weakness, cough (Dry and Wet) sometimes with fresh blood, and weight loss.
Treatment options; Initial treatment of mucormycosis starts with an early aggressive surgical debridement of the tissues that are affected. Then they are combined with amphotericin B deoxycholate (AmB) or liposomal amphotericin B (L-AmB).
This patient tried 1 course of Amphotericin Injections. But the follow-up HRCT still revealed a left lobe lesion and was advised surgery. But the prognosis was very grave due to his age, DM, HTN, and LV Dysfunction and a Post CABG patient.
Prognosis: Early detection of Black Fungus can be successfully treated. But if the patient does not respond to the antibiotic treatment, it can cause grave complications like blindness, bone infection, meningitis, brain abscess, sepsis and haemorrhage in the infected organ. This 63-year-old male patient was diagnosed case of Left Lobe Pulmonary Mucormycosis (Aspergillosis) and tried Antibiotic Injection but did not respond. Surgery was advised, but the prognosis was grave owing to his age, Diabetes, Hypertension, and LV Dysfunction. But with Ayurvedic treatment, he got relief from his symptoms and the Dual Energy CT Scan showed a decrease in the lesions
-
Ayurveda Diagnosis
AYURVEDIC DIAGNOSIS; KAPHAJA KRMI (FUFFUSA GATA KRIMI)
ABOUT THE DISEASE;
The word Krmi is derived from dhatu ‘kunya himsAyAm’ (Siddhantakaumudi) which means ‘to kill' or to ‘yield harmful effect’. Ashtanga Hrdaya mentions that krimi are present all over the biosphere. Their Utpatti Sthanas are told as parvata (mountain), vana (forest), oushadhi (plants), pashu (animals), apsu (water).
After the Vedic period, the description of Krimi is found in Samhita Kala, where Caraka has mentioned Krimiroga in the Vimana sthana of Caraka Samhita, in the parlance of Krimija Hridroga & Sirasula, and an indirect reference in Janapadodhvamsa. The Susruta Samhita on the other hand has described Krimiroga in Nidana and Cikitsa sthana. Susruta mentions that Kushtha is a Upasargika Roga indicating that it is contagious, which in turn implies the role of the microbes. Acaryas have described Krimi roga as a primary disease and also as a causative factor for other diseases e.g. siroroga, and hridroga.
Nidana- Factors responsible for the growth of Krimi are intake of food in indigested state, excess use of madhura and amla rasa, pishtanajaggery, milk, kusumba oil, til oil, fish, anoopmamsa, sedentary life style, excess day sleeping and use of dietetic incompatibilities.
Due to causative aggravating factors, Kapha and Pitta get aggravated. It generates different types of Krimi. These Krimi reside at various places in the body like amasaya, pakvasaya, dhamani and rakta etc.विंशतिविधाः क्रिमयः पूर्वमुद्दिष्टा नानाविधेन प्रविभागेनान्यत्र सहजेभ्यः; ते पुनः प्रकृतिभिर्विभज्यमानाच्चतुर्विधा भवन्ति; तद्यथा- पुरीषजाः, श्लेष्मजाः, शोणितजा, मलजाश्चेति॥९॥ (CS.Vi.7)
There are 20 types of Krimi, which can be generally classified as Bahya and Abhyantara. The main four types of krmi are purishaja, shleshmaja, shonitaja and malaja, that can be categorised into bahya and abhyantara. Another type of classification is Drishya and Adrishya. The chikitsa sutra for krimi is Apakarshaṇa (Extraction measures), Prakriti Vighata (Antagonistic measures) and Nidana Parivarjana (Avoidance of causative factors).
The patient was diagnosed as Kaphaja Krimi by the treating physician based on the clinical presentation. As this is infesting the lungs, it has been mentioned as Fuffusa gata. The line of treatment followed, and the pathyapathya was as indicated in Krimi roga. Along with this shvasa, kushtha, raktaja krimi, krimija sirasula line of treatments were also followed.
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Svasakutara Rasa Tablet 1-1-1 After Food with warm water 2021-08-02 - 2021-08-12 AFI.Vol 1.20.49 Vyadhiharana Rasa Tablet 1 pinch per day 2 gms for 15 days 2021-08-02 - 2021-08-25 Patent & Proprietary medicine Serenkottai Nei Capsule Capsule 1-1-1 With warm water after food 2021-08-02 - 2022-01-24 Patent & Proprietary medicine Rasagandhi Mezhugu Capsule 1-0-1 With warm water after food 2021-08-02 - 2021-12-23 Classical Siddha Medicine. Pulipani Vaidyam – 500 Krimikutara Rasa Tablet 2-2-2 With warm water after food 2021-08-02 - 2021-10-10 Rasa Tantra Sara- Siddha Yoga Sangraha Kharaliya Rasayana Krimikutara Rasa Tablet 2-2-2 With warm water after food 2021-12-24 - 2022-01-24 Rasa Tantra Sara- Siddha Yoga Sangraha Kharaliya Rasayana Punarnava, vaca, haridra, daruharidra, sunthi, vamsapatra Lepa Required quantity Apply as leap on the chest, once a day for 20 minutes 2021-08-03 - 2021-08-09 Anubhuta yoga Gandhaka rasayana Capsule 1-1-1 With warm water after food 2021-08-02 - 2021-09-22 Yogaratnakara Rasayana Adhikara.1-4 Palasa Bija Powder 13 gms per day For fumigation, once a day 2021-08-02 - 2021-08-12 Anubhuta prabhuta yoga Palasa Bija Powder 13 gms per day For fumigation, once a day 2021-10-23 - 2022-01-23 Anubhuta yoga Palasa Bija Powder 13 gms per day For fumigation, once a day 2022-03-05 - 2022-03-20 Anubhuta yoga Bhallataka Curna Powder 35-40 gms per day For fumigation, once a day 2021-10-23 - 2022-01-22 Anubhuta yoga Vilvadi Gulika Powder 100 tablets powdered Mixed with the dhupana dravya 2021-10-23 - 2022-01-22 AH.Utt,36.84-85 Dusivisari Gulika Powder 100 tablets powdered Mixed with the dhupana dravya 2021-08-02 - 2021-08-12 AH.Utt.35 Dusivisari Gulika Powder 100 tablets powdered Mixed with the dhupana dravya 2022-03-05 - 2022-03-20 AH.Utt.35 Vidanga curna Curna Required quantity Used as jalapana 2021-08-02 - 2021-08-12 Anubhuta dravya prayoga Vidanga curna Curna Required quantity Used as jalapana 2021-09-23 - 2021-10-22 Anubhuta dravya prayoga Vidanga curna Curna Required quantity Used as jalapana 2022-03-05 - 2022-03-20 Anubhuta dravya prayoga Pushkaramula curna Curna Required quantity Used as jalapana 2021-12-03 - 2021-12-03 Anubhuta dravya prayoga Kaphasura Kvatha Syrup 3 tsp After Food Thrice Daily 2021-08-02 - 2021-08-02 Patent & Proprietary medicine Malla sindura + Svasakutara rasa + Abhraka Bhasma + Svasa Kasa Cintamani + Pravala Pisti Curna Malla sindura 3 gms + Svasakutara rasa 60 tablets + Abhraka Bhasma 10gm + Svasa Kasa Cintamani 15 ta Made into 20 packets oe equal quantity. 1 ppt mixed with honey in the evening 2021-08-03 - 2021-08-13 Anubhuta yoga Wheeziwin Tablet Tablet 1-0-1 With warm water after food 2021-08-03 - 2021-09-10 Patent & Proprietary medicine Karbogi Tablet Tablet 1-0-1 With warm water 2021-08-03 - 2021-08-25 Patent & Proprietary medicine Amalaki rasayana+ Malla sindura Lehya 100gm of Amalaki Rasayana mixed with 3 gm of Malla Sindura 1/2 tsp morning and evening mixed with warm water. 2021-08-13 - 2021-08-25 Amalaki rasayana- Bhavaprakasha Nighantu. Haritakyadi Varga.39-40. Malla sindura- Rasatantra. 13 Ed. 472-73 Trailokyacintamani Rasa Tablet 1-0-1 After Food with warm water 2021-08-13 - 2021-10-10 Rajendra Sara Sangraha. Jvara Adhikara Tarilokyacintamani Rasa Tablet 1-0-1 After Food with warm water 2022-01-25 - 2022-03-04 Rajendra Sara Sangraha. Jvara Adhikara Nagarjunabhra Rasa Tablet 1-0-1 After Food with warm water 2021-08-13 - 2021-10-10 Bhaisajya Ratnavali. Hikka svasa cikitsa.36.65-68. Nagarjunabhra Rasa Tablet 1-0-1 After Food with warm water 2021-11-23 - 2022-03-04 Bhaisajya Ratnavali. Hikka svasa cikitsa.36.65-68. Vranaropahari Rasa Tablet 1-0-1 After Food with warm water 2021-08-26 - 2022-03-04 Patent & Proprietary medicine Mayuracandrika Bhasma Bhasma 2 pinch SOS Whenever there is vomitting 2021-08-26 - 2021-09-10 Siddha Yoga Sangraha Brhatvatacintamani Rasa Tablet 1-0-1 With warm water, after food 2021-08-26 - 2022-12-21 Bhaishajya Ratnakara.4.6985 Krmighna Vati Vati 2-2-2 With warm water 2021-08-26 - 2022-01-24 Patent & Proprietary medicine Kanakasava Asava 4 tsp After food, twice daily 2021-09-11 - 2021-09-11 Bhaishajya Ratnavali. 16.115-119 Krmimudgara Rasa Tablet 1-1-1 With warm water 2021-09-11 - 2022-01-24 Yogaratnakara. Purvardham. Vol 1. Pg 413. Bhallatakadya Vati Vati 1-1-1 With warm water 2021-10-11 - 2022-01-22 Basavarajeeyam Bhallatakadya Vati Vati 1-1-1 With warm water 2021-11-23 - 2022-02-22 Basavarajeeyam Somajivani Syrup 3 tsp In the morning and evening. 2021-11-23 - 2021-11-23 Patent & Proprietary medicine Van Mezhugu Tablet 1 OD With warm water 2021-12-24 - 2022-01-24 Siddha Medicine Hemagarbha Pottali Pottali 10 rounds Given in the morning and evening 2022-02-23 - 2022-03-04 Rasamrta Rasayana Vajikarana Adhyaya. 9.210-222. Rasagarbha Pottali Pottali 10 rounds Given in the morning and evening 2022-02-23 - 2022-03-04 Rasayogasagara. Vol 2.581 Hemagarbha Pottali Pottali 10 rounds Given in the morning and evening 2022-03-21 - 2022-12-31 Rasamrta Rasayana Vajikarana Adhyaya. 9.210-222. Rasagarbha Pottali Pottali 10 rounds Given in the morning and evening 2022-03-21 - 2022-12-31 Rasayogasagara. Vol 2.581 Suddha guggulu Tablet 2-0-2 After Food Thrice Daily 2022-02-23 - 2022-03-04 Patent & Proprietary medicine Suddha guggulu Tablet 2-0-2 After Food Thrice Daily 2022-03-21 - 2022-12-31 Patent & Proprietary medicine -
Outcome Measures
OUTCOME MEASURES;
The patient is a 63-year-old male presented with severe breathlessness even when engaged in a simple activity like walking, standing up, or climbing stairs; severe weakness, cough (Dry and Wet) sometimes with fresh blood, and weight loss since July 2021.He had a history of Covid 19 Pneumonitis on 10.6.21. Post covid he took 1 week of Inpatient treatment at Orange Hospital for generalized weakness and decreased oral intake (21.6.21- 28.6.21). HRCT Lungs revealed a left lower lobe lesion with consolidation. He was on medication for diabetes, and hypertension and also suffered from LV dysfunction. He was advised surgery and the grave prognosis was explained to the family due to the associated complaints.
Assessment criteria; Both subjective and objective parameters were used for assessment.
Subjective assessment- The patient appears better, and seems to be having a good satvabala, as compared to the debilitated look he had earlier. With just 1 week of Ayurvedic medications, an improvement was seen in symptoms. As on 23.11.21, after 3 months of ayurvedic treatment, all symptoms were relieved except for occasional blood in the sputum.
Objective Parameters; The 128 Slice Dual Energy CT Scan of the Chest (P+C) was done before, after and during follow-up.
Image 1. 128 Slice Dual Energy CT Scan dated 23.11.2021 added below
Image 2. 128 Slice Dual Energy CT Scan dated 16.5.2022 added below
Table 1. The impressions of the 128 Slice Dual Energy Ct Scan are tabulated as follows
Dates
Findings
Impressions
8.9.21
Compared to 2.8.21, no appreciable change in the status of infective process
A cavitary lesion with necrotic component and air foci within (approx 6 x 5 cm) is seen in left lower lobe basal segment .
23.11.21
Compared to 8.9.21, mild regression in the status of infective process
A cavitary lesion with evidence of soft tissue and air foci within is seen in apical segment of left lower lobe (approx 4.5 x 3.5 cm).
16.5.22
Compared to previous CT scan dated 23/11/2021, there is regression in status of cavitory lesion .
A cavitory lesion with evidence of soft tissue and air foci within is seen in apical seement of left lower lobe (approx 3 x2 8 cm)
Disease Modifying Effect: The patient is in remission and is still continuing the medicines
Image 1. 128 Slice Dual Energy CT Scan dated 23.11.2021
Image 2. 128 Slice Dual Energy CT Scan dated 16.5.2022
-