Featured Case
-
Abstract
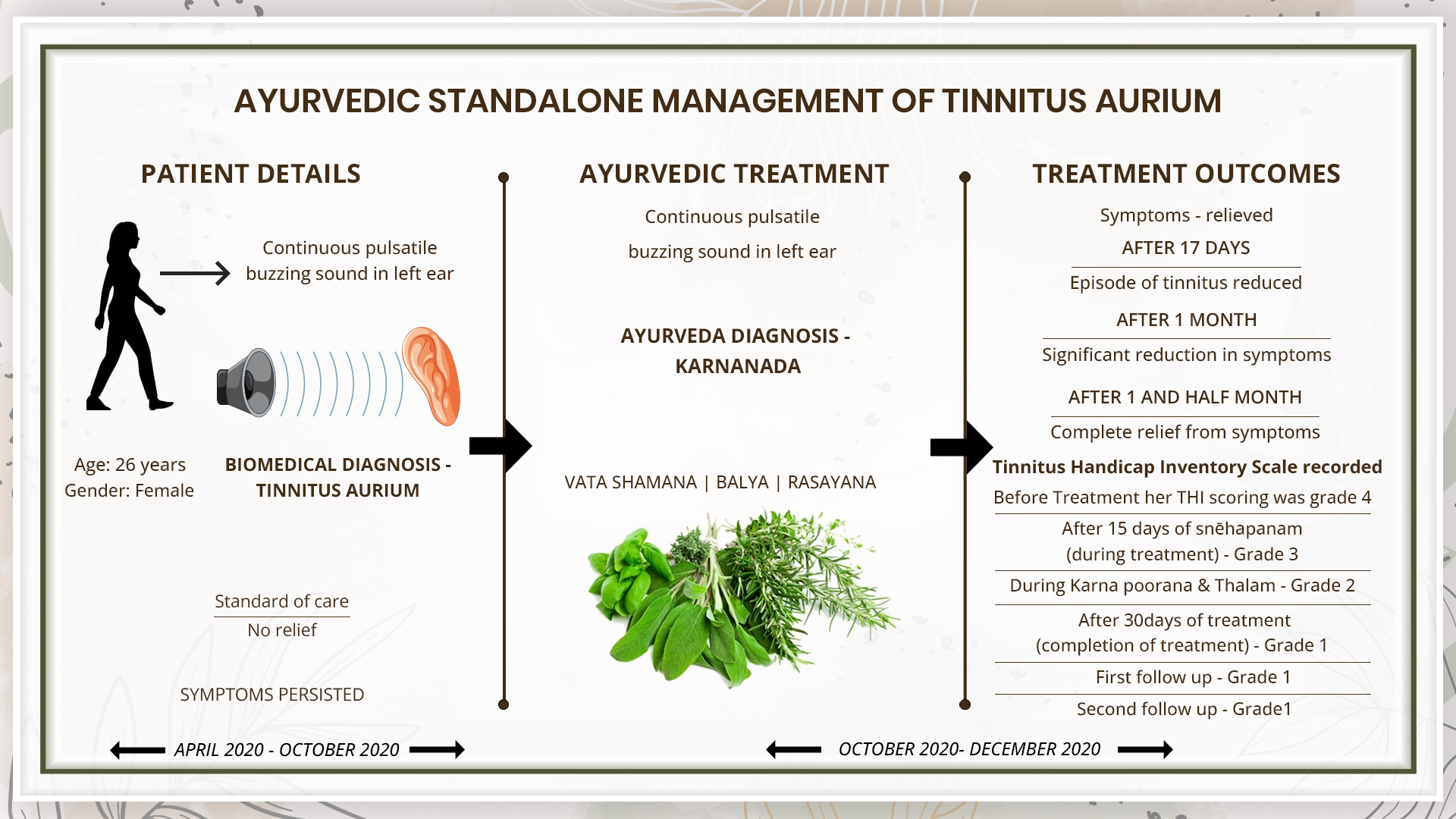
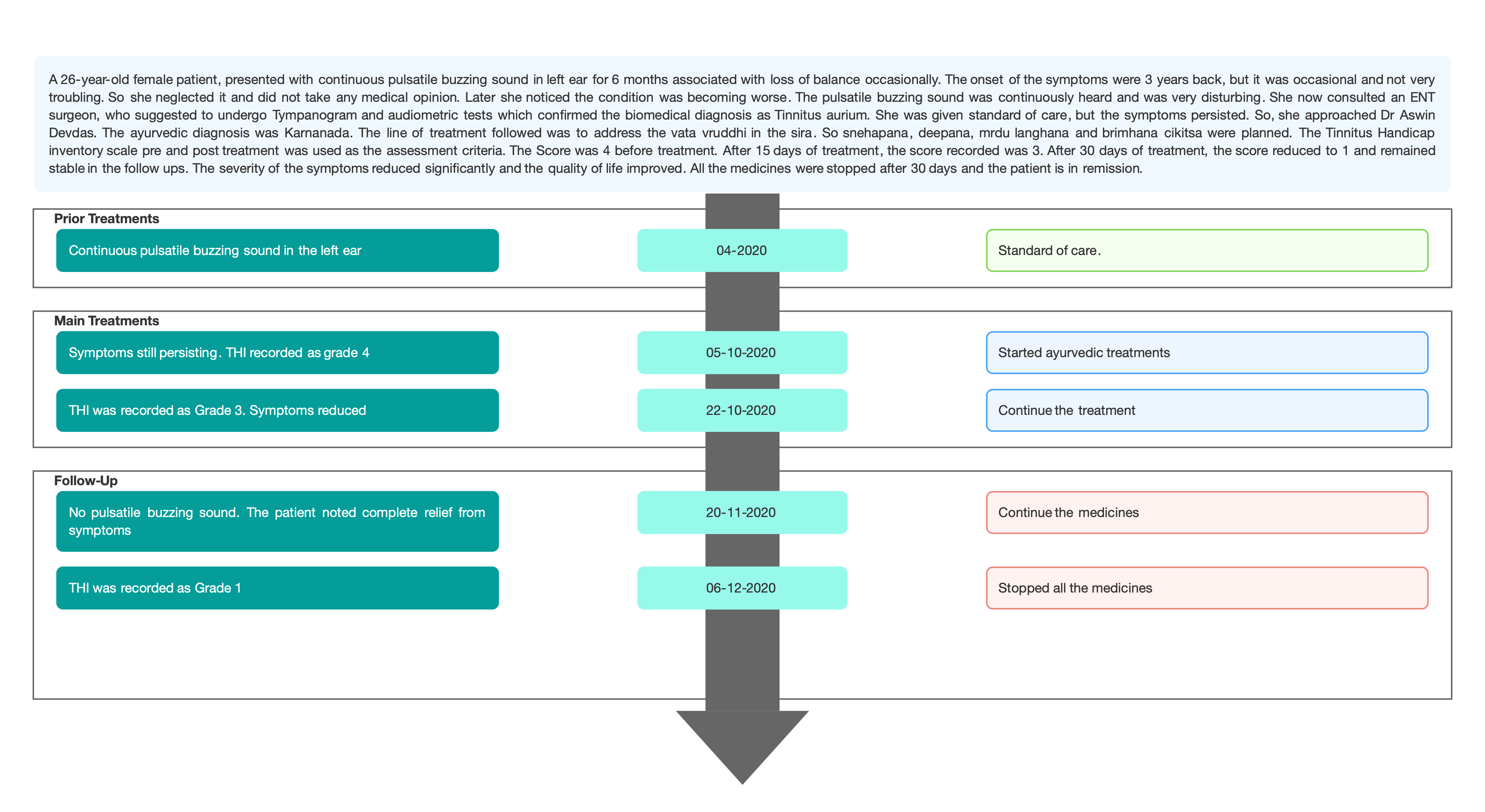
A 26-year-old female patient, presented with continuous pulsatile buzzing sound in left ear for 6 months associated with loss of balance occasionally. The onset of the symptoms were 3 years back, but it was occasional and not very troubling. So she neglected it and did not take any medical opinion. Later she noticed the condition was becoming worse. The pulsatile buzzing sound was continuously heard and was very disturbing. She now consulted an ENT surgeon, who suggested to undergo Tympanogram and audiometric tests which confirmed the biomedical diagnosis as Tinnitus aurium. She was given standard of care, but the symptoms persisted. So, she approached Dr Aswin Devdas. The ayurvedic diagnosis was Karnanada. The line of treatment followed was to address the vata vruddhi in the sira. So snehapana, deepana, mrdu langhana and brimhana cikitsa were planned. The Tinnitus Handicap inventory scale pre and post treatment was used as the assessment criteria. The Score was 4 before treatment. After 15 days of treatment, the score recorded was 3. After 30 days of treatment, the score reduced to 1 and remained stable in the follow ups. The severity of the symptoms reduced significantly and the quality of life improved. All the medicines were stopped after 30 days and the patient is in remission.
-
Summaries
-
Listen
-
Watch
-
View
-
Read
A 26-year-old female patient, presented with continuous pulsatile buzzing sound in left ear for 6 months associated with loss of balance occasionally. The onset of the symptoms were 3 years back, but it was occasional and not very troubling. So she neglected it and did not take any medical opinion. Later she noticed the condition was becoming worse. The pulsatile buzzing sound was continuously heard and was very disturbing. She now consulted an ENT surgeon, who suggested to undergo Tympanogram and audiometric tests which confirmed the biomedical diagnosis as Tinnitus aurium. She was given standard of care, but the symptoms persisted. So, she approached Dr Aswin Devdas. The ayurvedic diagnosis was Karnanada. The line of treatment followed was to address the vata vruddhi in the sira. So snehapana, deepana, mrdu langhana and brimhana cikitsa were planned. The Tinnitus Handicap inventory scale pre and post treatment was used as the assessment criteria. The Score was 4 before treatment. After 15 days of treatment, the score recorded was 3. After 30 days of treatment, the score reduced to 1 and remained stable in the follow ups. The severity of the symptoms reduced significantly and the quality of life improved. All the medicines were stopped after 30 days and the patient is in remission.
-
-
Timeline
-
Tabulated Summary
-
Narrative
TITLE OF CASE
Standalone successful ayurvedic management of Tinnitus Aurium - A case report
Dr Aswin T Das
ABSTRACT
A 26-year-old female patient, presented with continuous pulsatile buzzing sound in left ear for 6 months associated with loss of balance occasionally. The onset of the symptoms were 3 years back, but it was occasional and not very troubling. So she neglected it and did not take any medical opinion. Later she noticed the condition was becoming worse. The pulsatile buzzing sound was continuously heard and was very disturbing. She now consulted an ENT surgeon, who suggested to undergo Tympanogram and audiometric tests which confirmed the biomedical diagnosis as Tinnitus aurium. She was given standard of care, but the symptoms persisted. So, she approached Dr Aswin Devdas. The ayurvedic diagnosis was Karnanada. The line of treatment followed was to address the vata vruddhi in the sira. So snehapana, deepana, mrdu langhana and brimhana cikitsa were planned. The Tinnitus Handicap inventory scale pre and post treatment was used as the assessment criteria. The Score was 4 before treatment. After 15 days of treatment, the score recorded was 3. After 30 days of treatment, the score reduced to 1 and remained stable in the follow ups. The severity of the symptoms reduced significantly and the quality of life improved. All the medicines were stopped after 30 days and the patient is in remission.
KEYWORDS
Tinnitus, karnanada, case report, standalone, Tinnitus handicap inventory scale
INTRODUCTION
Tinnitus is the perception of sound in the absence of a corresponding external acoustic stimulus. With prevalence ranging from 10% to 15%, tinnitus is a common disorder. Many people habituate to the phantom sound, but tinnitus severely impairs the quality of life of about 1–2% of all people. Tinnitus can be associated with hearing loss, acoustic neuromas, drug toxicity, ear diseases, and depression. Tinnitus can last for many years and can interfere with sleep and concentration.
Diagnostic criteria: Assessment of patients includes a detailed case history, measurement of hearing function, quantification of tinnitus severity, and identification of causal factors, associated symptoms, and comorbidities. No objective test is available for most tinnitus cases, and diagnosis is made on the basis of medical history and an assessment of the effect on the patient and his or her family. Important questions include the location and character of the tinnitus, particularly whether it has a rhythmical or pulsatile component. Pulsatile tinnitus can in rare cases be objectively detected by auscultation.
Tinnitus handicap inventory scale (THI) was documented at baseline to assess the outcome of the treatments. The Grade was 4 prior to starting the treatment.
Treatments: Most widely used treatments for tinnitus involve counselling and the best evidence is available for cognitive behavioral therapy. New pathophysiological insights have prompted the development of innovative brain-based treatment approaches to directly target the neuronal correlates of tinnitus.
Prognosis: There is no absolute cure for Tinnitus. But treatments help improve the quality of life.
PATIENT INFORMATION
A 26-year-old female patient, presented with a continuous pulsatile buzzing sound in her left ear for 6 months associated with loss of balance occasionally.
Medical History: The onset of symptoms was 3 years back, which was occasional and not disturbing. So she neglected and did not take any consultation. Later she noticed the condition becoming worse and started to hear the sound continuously, which was disturbing. So she consulted an ENT surgeon, who suggested taking Tympanogram and audiometric tests which showed bilateral ‘A’ type tympanogram and hearing sensitivity within normal limits bilaterally. She was given standard care. Still, the condition persisted. So she opted for Ayurvedic treatment.
CLINICAL FINDINGS/PHYSICAL EXAMINATION
Routine Ear examinations:
External ear examination- Both Right and Left normal
External auditory canal- Tympanic membrane- Corn of light - present
No perforation noted
Rinne test- AC > BC (both ear)
Weber test- Lateralised towards right ear
Absolute Bone Conduction Test: Right ear- Normal Left ear- Reduced
TIMELINE
Image 1. Timeline of events attached below
DIAGNOSTIC ASSESSMENT
Modern Diagnostic parameter: The biomedical diagnosis was made based on Tympanogram and audiometric tests which showed bilateral ‘A’ type tympanogram, and hearing sensitivity within normal limits bilaterally.
Ayurvedic Assessment was done based on the clinical evaluation by the ayurvedic physician.
Differential Diagnosis- This does not apply as the patient came in with a definite diagnosis.
Prognosis- While there is no cure, most people with tinnitus get used to it over time; for a minority, it remains a significant problem. The primary treatment for tinnitus is talk therapy, sound therapy, or hearing aids. There are no effective drugs that treat tinnitus. In this case report, the condition was neglected in the beginning as the sound was not heard continuously. Later there was a continuous pulsatile buzzing sound in the left ear associated with loss of balance occasionally. With standard care, no improvement was noted, she hence opted for Ayurvedic treatment. With 30 days of Ayurvedic treatment, the severity of the condition reduced and the quality of life of the patient improved.
THERAPEUTIC INTERVENTION
See the tab ‘Treatment details’
FOLLOW-UP AND OUTCOMES
Clinician-based assessment; Subjective parameters were assessed. Pain reduced after 3 days of treatment. The patient attained complete symptomatic relief within 7 days of treatment. No pain in the abdomen, normal bowels, and hunger were restored.
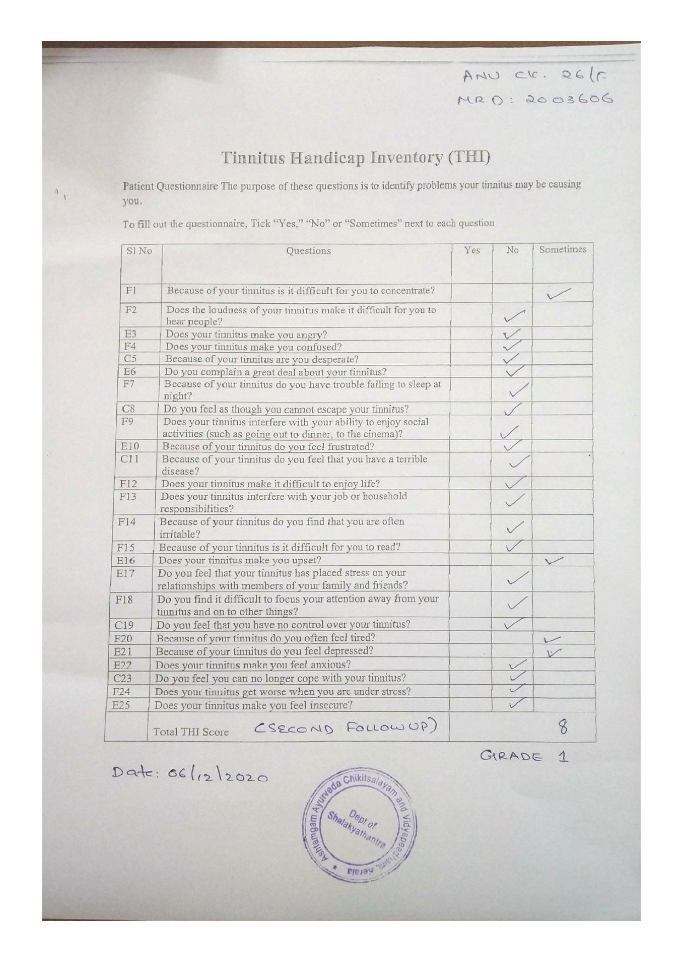
Patient assessed: THI (Tinnitus handicap inventory scale) was graded before, during and after treatment and follow ups to assess the outcomes of the treatment. They were documented as follows:
• Before Treatment her THI scoring was grade 4
• After 15 days of snehapanam (during treatment) -Grade 3
• During Karna poorana and Thalam- Grade 2
• After 30 days of treatment (completion of treatment)-Grade 1
• First follow up- Grade 1
• Second follow up- Grade1
Image 2. THI at baseline dated 5.10.2020 added below
Image 3. THI during treatment dated 22.10.2020 added below
Image 4. THI after treatment dated 5.11.2020 added below
Image 5. THI during first follow-up dated 22.11.2020 added below
Image 6. THI during second follow-up dated 6.12.2020 added below
Intervention adherence and tolerability – The patient adhered to the prescribed treatments and tolerated the treatments well.
Method of assessment- By monitoring the patient.
Adverse and unanticipated events; None reported.
DISCUSSION ;
Karnanada is one of the most common karna roga and it affects one’s daily routine. Due to vata dosha predominance in this condition, vatahara measures were taken into consideration.
The treatment was started with initial langhana which is not vata vardhana but at the same time dipana in action, keeping in mind the importance of mrdu langhana before starting brmhana. As per the protocol, shaddharana curnam was given for 7 days. Along with it, dusparshakadi kashaya was given considering the presence of bhrama (giddiness) associated with the same complaint. Dusparshaka is very effective in diseases affecting the indriya. After one week, snehapana was started with kalyanaka ghrita as shamana at night time, considering the site of roga and the aushadha kala specified. This ghrita was selected considering its indication in moha and unmada and thus giving priority to the site concerned as well as considering the probable nidana of stress. Along with this sidhamakaradwaja was administered with honey considering its vatas hamana, sukshma guna, and action on indriyas, rasayana and balya karma. Apart from this, Karnapoorana (bahya snehana karma) was done with vilwam pachottyadi tailam which is vata hara initiating shamana of sthanika dosha. Along with this, dhanwantaram 101 avarti was given as murdha tailam taking into account the vata vriddhi in sira.
PATIENT’S PERSPECTIVE
Not available.
LEARNING POINTS/TAKE-HOME MESSAGES
This case report demonstrates the successful ayurvedic management of a chronic case of Tinnitus aurium in a 26-year-old female, who was not responding satisfactorily to the standard of care.
INFORMED CONSENT
Written consent was obtained from the patient to publish the case report.
CONFLICT OF INTEREST
None declared.
FUNDING
None
REFERENCE
- Langguth B, Kreuzer PM, Kleinjung T, De Ridder D. Tinnitus: causes and clinical management. Lancet Neurol. 2013;12(9):920-930. doi:10.1016/S1474-4422(13)70160-1
- Savage J, Waddell A. Tinnitus. BMJ Clin Evid. 2014;2014:0506. Published 2014 Oct 20.
- Baguley D, McFerran D, Hall D. Tinnitus. The Lancet. 2013 Nov 9;382(9904):1600-7.
Image 1. Timeline of events added below
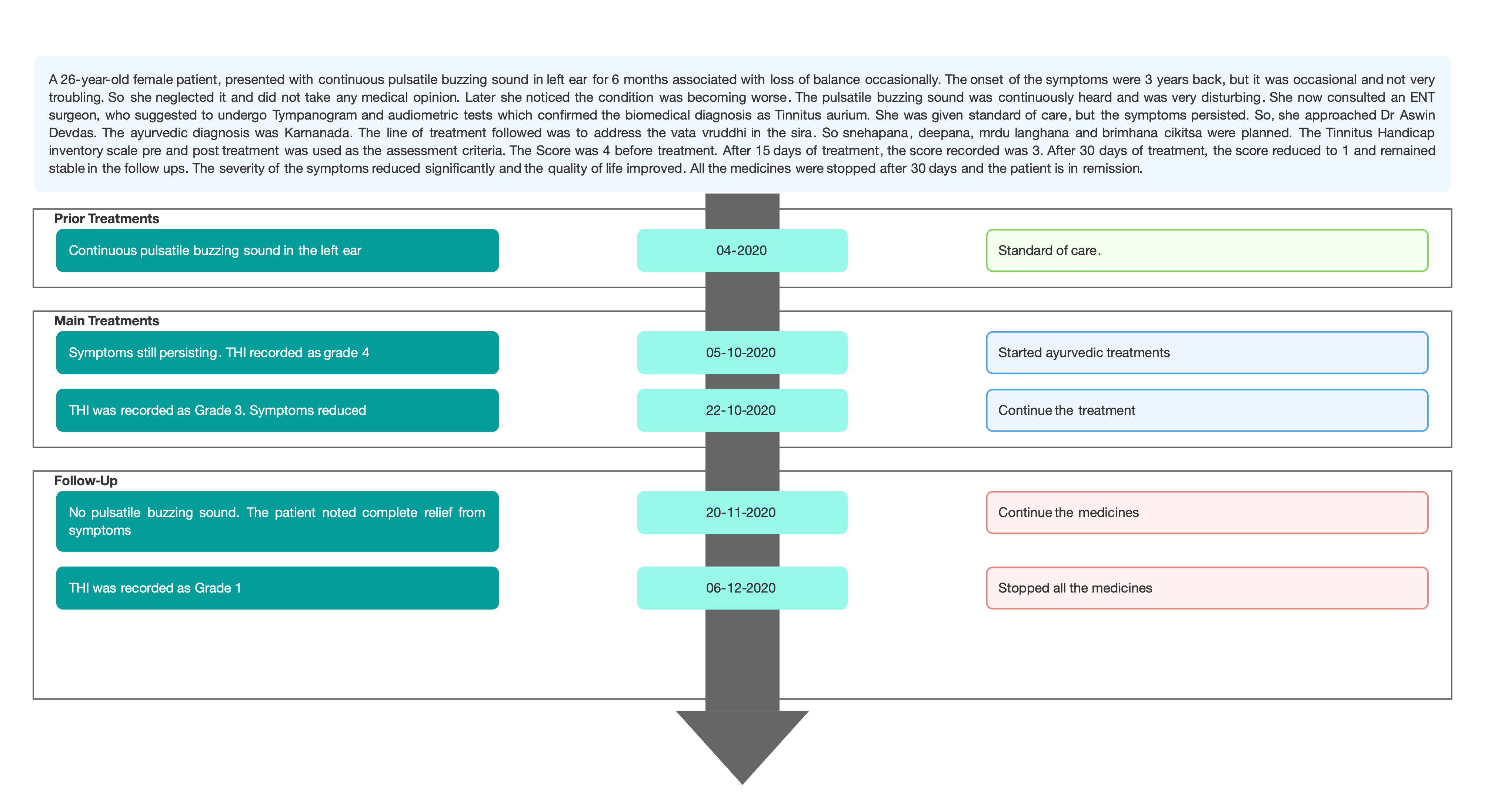
Image 2. THI at baseline dated 5.10.2020 added below
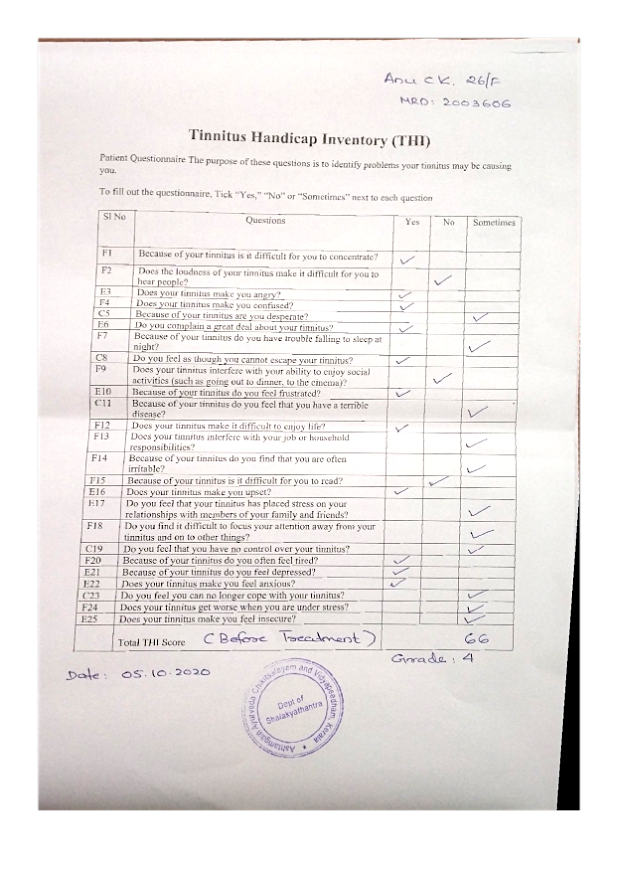
Image 3. THI during treatment dated 22.10.2020 added below
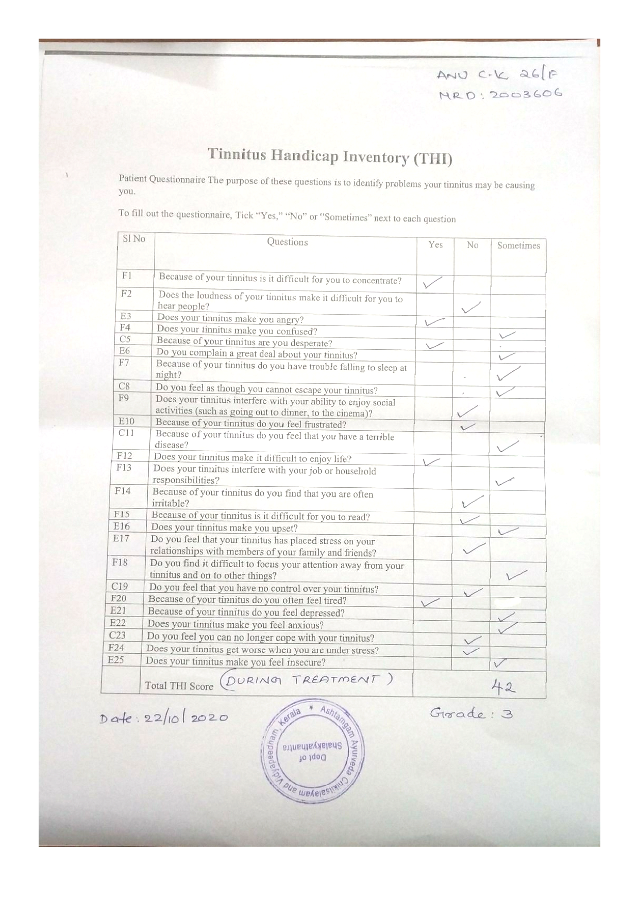
Image 4. THI after treatment dated 5.11.2020 added below
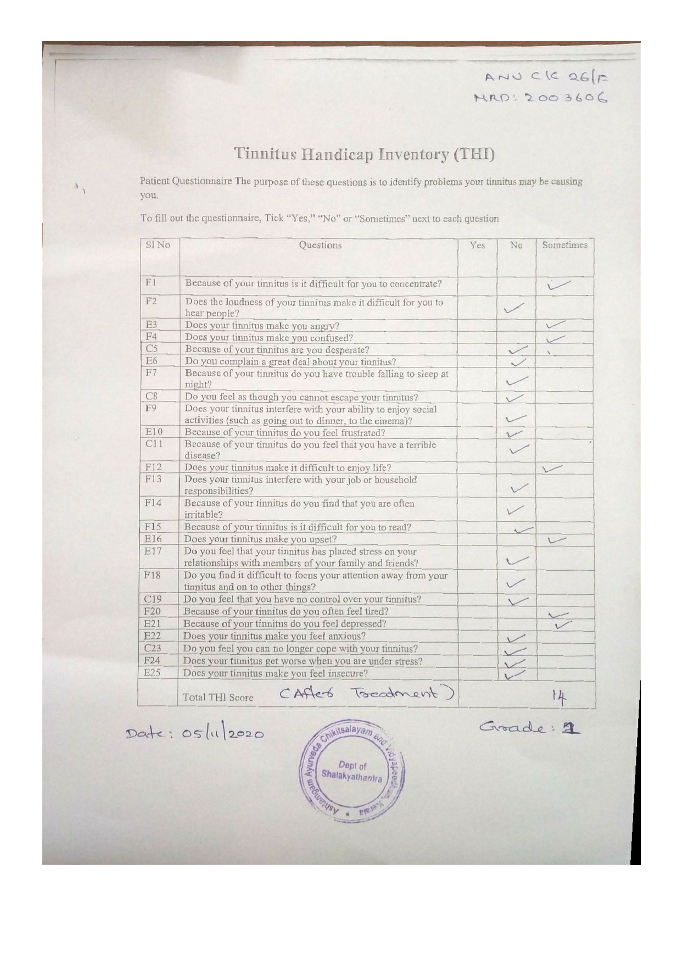
Image 5. THI during first follow-up dated 22.11.2020 added below
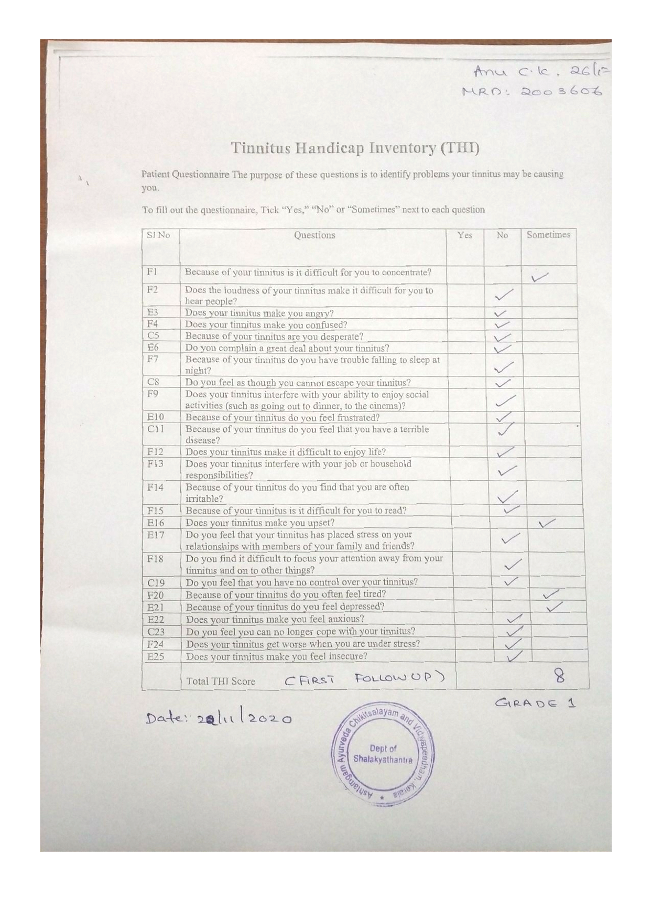
Image 6. THI during second follow-up dated 6.12.2020 added below
-
Immersive Learning
-
Modern Diagnosis
MODERN DIAGNOSIS: Tinnitus aurium
ABOUT THE DISEASE:
Tinnitus is the perception of sound in the absence of a corresponding external acoustic stimulus. With prevalence ranging from 10% to 15%, tinnitus is a common disorder. Many people habituate to the phantom sound, but tinnitus severely impairs the quality of life of about 1–2% of all people. Tinnitus can be associated with hearing loss, acoustic neuromas, drug toxicity, ear diseases, and depression. Tinnitus can last for many years and can interfere with sleep and concentration.
Diagnostic criteria: Assessment of patients includes a detailed case history, measurement of hearing function, quantification of tinnitus severity, and identification of causal factors, associated symptoms, and comorbidities. No objective test is available for most tinnitus cases, and diagnosis is made on the basis of medical history and an assessment of the effect on the patient and his or her family. Important questions include the location and character of the tinnitus, particularly whether it has a rhythmical or pulsatile component. Pulsatile tinnitus can in rare cases be objectively detected by auscultation.
In this case report, the patient is a 26-year-old female, who was suffering from a continuous pulsatile buzzing sound in her left ear for 6 months associated with loss of balance occasionally. The onset of the symptoms was 3 years back, but it was occasional and not very troubling. So she neglected it and did not take any medical opinion. Later she noticed the condition was becoming worse. The pulsatile buzzing sound was continuously heard and was very disturbing. She now consulted an ENT surgeon, who suggested to undergo Tympanogram and audiometric tests which confirmed the biomedical diagnosis as Tinnitus aurium. She was given standard of care, but the symptoms persisted.
Tinnitus handicap inventory scale (THI) was documented at baseline to assess the outcome of the treatments. The Grade was 4 prior to starting the treatment.
Image 1. THI patient questionnaire before treatment dated 5.10.2020 added below.
Treatments: Most widely used treatments for tinnitus involve counselling and the best evidence is available for cognitive behavioural therapy. New pathophysiological insights have prompted the development of innovative brain-based treatment approaches to directly target the neuronal correlates of tinnitus.
Prognosis: There is no absolute cure for Tinnitus. But treatments help improve the quality of life.
Reference
- Langguth B, Kreuzer PM, Kleinjung T, De Ridder D. Tinnitus: causes and clinical management. Lancet Neurol. 2013;12(9):920-930. doi:10.1016/S1474-4422(13)70160-1
- Savage J, Waddell A. Tinnitus. BMJ Clin Evid. 2014;2014:0506. Published 2014 Oct 20.
- Baguley D, McFerran D, Hall D. Tinnitus. The Lancet. 2013 Nov 9;382(9904):1600-7.
-
Ayurveda Diagnosis
AYURVEDA DIAGNOSIS: Karnanada
ABOUT THE DISEASE:
Karnanada is basically caused by vitiated vata dosa in which a person hears different types of sound in absence of any relevant external stimulus. Taking into consideration the clinical presentation, this can be correlated with tinnitus, a disease with multifactorial etiology. It may be concerned with the unhealthy condition of only ear, ear with a disease of the head, only disease of the head or may be associated with a general body condition.
In Karnanada patient can hear different types of sound in the ear which can be unilateral or bilateral and stable or transient type. This sound may vary in pitch, quality and loudness. It might be a swishing, hissing, roaring, clicking, or a rustling type of noise. It is more irritating in a silent environment as at night when the masking effect of ambient noise from the environment is absent. It is a symptom, not a disease and causes might be present in the external, middle or inner ear in the 8th nerve or inside the brain.
Causative factors: Acarya Sushruta has not described the common Karnaroga Nidanas but Yogratnakara has explained Samanya Karnaroga Nidanas. According to him Avashyaya,, Jalakrida, Karnakandu, Mithyayoga of Shastras leads to the vitiation of vata. Further this Dushita vata vitiates other doshas, that localises in the Karna siras and cause aural diseases.
In this case report, the patient is a 26-year-old female patient, suffering from a continuous pulsatile buzzing sound in the left ear for 6 months associated with loss of balance occasionally. She tried the standard of care but did not get relief. Hence she opted for ayurvedic management. Based on the clinical evaluation, the diagnosis was made as Karnanada.
Complications: Karnanada if left untreated can lead to Karna badhirya. The patients who are vulnerable to a vata imbalance, can be affected faster. This can further cause sleeping and irritation problems, annoyance and hypersensitivity.
Treatment: Four disease namely Karnashula, Karnanada, Karna badhirya and Karna kshveda generally treated with same line of treatment. (Sushruta Samhita. 21.4) Vata pacifying herbs and therapies like Snehana, Svedana, Nasya, Karnapoorana, Shiro and Padabhyanga supported with balya, medhya aushadha will help manage the condition successfully.
Rationale of treatment in this patient: Karnanada is one of the most common karna roga and it affects one’s daily routine. Due to vata dosha predominance in this condition, vatahara measures were taken into consideration.
The treatment was started with initial langhana which is not vata vardhana but at the same time dipana in action, keeping in mind the importance of mrdu langhana before starting brmhana. As per the protocol, shaddharana curnam was given for 7 days. Along with it, dusparshakadi kashaya was given considering the presence of bhrama (giddiness) associated with the same complaint. Dusparshaka is very effective in diseases affecting the indriya. After one week, snehapana was started with kalyanaka ghrita as shamana at night time, considering the site of roga and the aushadha kala specified. This ghrita was selected considering its indication in moha and unmada and thus giving priority to the site concerned as well as considering the probable nidana of stress. Along with this sidhamakaradwaja was administered with honey considering its vata shamana, sukshma guna, and action on indriyas, rasayana and balya karma. Apart from this, Karnapoorana (bahya snehana karma) was done with vilwam pachottyadi tailam which is vata hara initiating shamana of sthanika dosha. Dhanwantaram 101 avarti was given as murdha tailam taking into account the vata vrudhi in sira.
Reference:
- Anubha Jain & Mukesh Kumar Gupta: An ayurvedic review of Karnanada WSR Tinnitus. International Medical Journal (online) 2021. doi:10.46607/iamj1709042021
-
Treatment
Name of Medicine Dosage Form Dosage Mode of Administrtation From - To (Date) Medicine Reference Shaddharanam Curnam Curna 10 gms With warm water, before breakfast 2020-10-05 - 2020-10-11 AS.Utt.34 Dusparshakadi Kasaya Kasaya 15 ml + 45 ml warm water At 6 pm 2020-10-05 - 2020-10-11 AH.Ci.8.63-64 Kalyanaka Ghrita Ghrita 25 ml At 10 pm 2020-10-05 - 2020-10-18 AH.Utt.6. 26-31 Siddhamakaradhvaja Curna 125 mg With honey, once daily 2020-10-05 - 2020-10-18 Rasatarangini Nimbamritaadi erandam Taila Taila 20 ml Virecana 2020-10-19 - 2020-10-19 AH.Ci.21.58-61 Vilvam pachottyaadi tailam Taila 10 ml Karnapoorana 2020-10-22 - 2020-11-05 Sahasra yogam. Taila prakarana Dhanawantharam 101 avarthi Taila Required quantity Sirothalam 2020-10-22 - 2020-11-05 Sahasra yogam. Taila prakarana Dusparshakadi panajala Panam Required quantity Oral, when required 2020-10-22 - 2020-11-05 Anubhuta dravya prayoga -
Outcome Measures
OUTCOME MEASURES
A 26-year-old female patient, presented with continuous pulsatile buzzing sound in left ear for 6 months associated with loss of balance occasionally. The onset of the symptoms were 3 years back, but it was occasional and not very troubling. So she neglected it and did not take any medical opinion. Later she noticed the condition was becoming worse. The pulsatile buzzing sound was continuously heard and was very disturbing. She now consulted an ENT surgeon, who suggested to undergo Tympanogram and audiometric tests which confirmed the biomedical diagnosis as Tinnitus aurium. She was given a standard of care, but the symptoms persisted. So, she approached Dr Aswin Devdas. The ayurvedic diagnosis was Karnanada.
Assessment criteria: Both subjective and objective criteria were used for assessing the outcomes.
Subjective parameters: The severity of the symptoms reduced significantly and the quality of life improved. All the medicines were stopped after 30 days and the patient is in remission.
Objective parameters: The patient questionnaire Tinnitus handicap inventory scale (THI) was documented pre and post-ayurvedic treatments are as follows:
· Before Treatment her THI scoring was grade 4
· After 15 days of snehapanam (during treatment) - Grade 3
· During Karna poorana and Thalam- Grade 2
· After 30 days of treatment - Grade 1
· First follow up- Grade 1
· Second follow up- Grade1
Image 1. THI at baseline dated 5.10.2020 added below
Image 2. THI during treatment dated 22.10.2020 added below
Image 3. THI after treatment dated 5.11.2020 added below
Image 4. THI during first follow-up dated 22.11.2020 added below
Image 5. THI during second follow-up dated 6.12.2020 added below
-